Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
DAS METABOLISCHE SYNDROM Lajos Szollár Vorstand der Pathophysiologie Semmelweis Universität, 2006

2
Todesuhrsache weltweit 2005
AIDS Tuberculose Malaria Kardiovasculäre Erkrankungen Krebs Kronische Lungenerkrankungen Diabetes Lancet 2005, 366: 1512

3
(Rastliche Lebensstyl) Embryonale Entwicklung
Warum ? – Das metabolische Syndrom Zu vieles Essen Sedentary lifestyle (Rastliche Lebensstyl) ? Ungeignetes Essen Gene Umgebung Embryonale Entwicklung
 Ungeignetes Essen. Gene. Umgebung. Embryonale Entwicklung.")
4
Risiko von ischemische Herzkrankheit nach
“traditionelle” und “nicht-traditionelle” Risikofaktoren The Québec Cardiovascular Study 30 Traditionelle Risikofaktoren Nicht-traditionelle Risikofaktoren 25 20.8 (<0.001) 20 Odds ratio* 15 9.1 (0.01) 10 4.4 (0.01) 4.7 5 2.8 1.8 A triad of non-traditional metabolic markers found in viscerally obese middle-aged men (hyperinsulinemia, raised apolipoprotein B concentration and small LDL particles) increases the risk of ischemic heart disease by 20-fold. KW: risk factors, obesity 1.0 1.0 1 2 3 Traditionell: LDL-cholesterol, triglyceride und HDL-cholesterol Nicht-traditionell: Insulin, apolipoprotein B und small, dense LDL * Odds ratios are adjusted for systolic blood pressure, family history of IHD and medication use Lamarche B et al. JAMA (1998) 279:
 20. Odds ratio* (0.01) (0.01) A triad of non-traditional metabolic markers found in viscerally obese middle-aged men (hyperinsulinemia, raised apolipoprotein B concentration and small LDL particles) increases the risk of ischemic heart disease by 20-fold. KW: risk factors, obesity Traditionell: LDL-cholesterol, triglyceride und HDL-cholesterol. Nicht-traditionell: Insulin, apolipoprotein B und small, dense LDL. * Odds ratios are adjusted for systolic blood pressure, family history of IHD. and medication use. Lamarche B et al. JAMA (1998) 279:")
5
Das metabolische Syndrom
Hochdruck Dyslipoproteinemie Insulinresistance Diabetes (II) Atherosclerose Obesität CHK
 Atherosclerose. Obesität. CHK.")
7
5 alarmierende Fakten Prevalenz von Typ 2 Diabetes und seine cardiovasculäre Komplikationen steigt Weltweit. Vorbeugende Konditionen und Risikofaktoren von Typ 2 Diabetes sind auch häufiger geworden. Die Warscheinlichkeit von Komplikationene von Diabetes – hauptsächlich cardiovasculäre Erkrankungen ist von der Dauer des Diabetes abhängig. Diabetes Behandlung ist teuer. Die Anzahl von Jugendlichen mit Typ 2 Diabetes steigt. Zimmet, P., Nature, (6865): p Alberti, K.G Diabetes Voice, 2002, 47
: p Alberti, K.G Diabetes Voice, 2002, 47.")
8
Schuldige Evolution? Millionen Jahren 50 Jahren H. Australopithecus
H. erectus H. sapiens H. McDonald’s Millionen Jahren 50 Jahren

9
Das metabolische Syndrom
Definition Prevalence (Haufigkeit) Pathophysiologie Entstehen Komplikationen, Folgen Behandlung
 Pathophysiologie. Entstehen. Komplikationen, Folgen. Behandlung.")
10
Das metabolische Syndrom
Definition Prevalence (Haufigkeit) Pathophysiologie Entstehen Komplikationen, Folgen Behandlung
 Pathophysiologie. Entstehen. Komplikationen, Folgen. Behandlung.")
11
Das metabolische Syndrom
Symultane auftreten von bestimmte kardiovasculäre Risikofaktoren: Centrale Adiposität Hyperinsulinämie/Insulinresistenz Hochdruck Atherogene Dyslipidämie

12
Die 4 Leitsymptome des metabolischen Syndroms

13
Zusammentreffen mehrerer Risikofaktoren: Das metabolische Syndrom
• HDL-Cholesterin < 40mg/dL (1 mmol/L) M < 50mg/dL (1,3 mmol/L) F • Nüchtern-Triglyceride > 150mg/dL (1,71mmol/L) • Taillenumfang > 102cm M (94) > 88cm F (8O) Body-Mass-Index > 30 kg/m2 M > 28 kg/m2 F Systolischer Blutdruck >140mmHg und/oder diastolischer Blutdruck >90 mmHg. • Nüchternblutzucker > 110 mg/dL (6,1 mmol/L)
 M. < 50mg/dL (1,3 mmol/L) F. • Nüchtern-Triglyceride > 150mg/dL (1,71mmol/L) • Taillenumfang. > 102cm M (94) > 88cm F (8O) Body-Mass-Index. > 30 kg/m2 M. > 28 kg/m2 F. Systolischer Blutdruck >140mmHg und/oder diastolischer Blutdruck >90 mmHg. • Nüchternblutzucker > 110 mg/dL (6,1 mmol/L)")
14
Insulin Resistance (T2DM, IFG, IGT)
World Health Organization Klinische Voraussetzungen für das metabolische Syndrom Insulin Resistance (T2DM, IFG, IGT) + 2 veitere Symptome BP > 140/90 mmHg oder anti-HT Medikation Plasma TG > 1.7 mmol/L HDL-C < 1 mmol/L (M); < 1.3 mmol/L (F) BMI > 30 kg/m2 oder W/H >0.9 (M) or > 0.85 (F) Urin albumin > 20 mg/min or Alb/Cr > 30 mg/g KW: metabolic syndrome, MS, risk factors, obesity, insulin resistance, WHO, diabetes, BMI, BP, HDL
 + 2 veitere Symptome. BP > 140/90 mmHg oder anti-HT Medikation. Plasma TG > 1.7 mmol/L. HDL-C < 1 mmol/L (M); < 1.3 mmol/L (F) BMI > 30 kg/m2 oder W/H >0.9 (M) or > 0.85 (F) Urin albumin > 20 mg/min. or Alb/Cr > 30 mg/g. KW: metabolic syndrome, MS, risk factors, obesity, insulin resistance, WHO, diabetes, BMI, BP, HDL.")
15
Kinder 7-17 Jahre in China (2002)
Übergewicht Obesität Große Städten Mittelgroße Reiche Dörfe Arme

16
Männlich Weiblich Centrale Obesität Centrale Obesität
Periphere Obesität

18
Das metabolische Syndrom
Definition Prevalence (Häufigkeit) Pathophysiologie Entstehen Komplikationen, Folgen Behandlung
 Pathophysiologie. Entstehen. Komplikationen, Folgen. Behandlung.")
19
Altersabhängige Auftreten (Prevalence) von metabolische Syndrom
4.33 Männer Frauen 50 45 40 35 30 25 20 15 10 5 Prevalence, % KW: metabolic syndrome, MS, NHANES III, gender, men, women, ATP III, age, prevalence 20-29 40-49 50-59 60-69 > 70 30-39 Älter (Jahren) Ford ES, et al. JAMA. 2002;287: 113C
 Ford ES, et al. JAMA. 2002;287: C.")
20
Das metabolische Syndrom
Prevalence 20% - 30% der mittelalterliche Bevölkerung in hochindustrialisierte Länder hat das metabolische Syndrom 2010: Million (USA) Kalff et al estimated that 20% to 30% of middle-aged individuals living in highly industrialized countries are affected by the cluster of illnesses associated with the metabolic syndrome, including obesity, hypertension, dyslipidemia, and glucose intolerance.1 By the year 2010, there could be as many as 50 to 75 million people in the United States with manifestations of the metabolic syndrome.2 References 1. Kalff KG, et al. Aviat Space Environ Med Dec;70(12): 2. Hansen BC. Ann N Y Acad Sci Nov 18;892:1-24. Kalff KG, et al. Aviat Space Environ Med Dec;70(12): Hansen BC. Ann N Y Acad Sci Nov 18;892:1-24.
 Kalff et al estimated that 20% to 30% of middle-aged individuals living in highly industrialized countries are affected by the cluster of illnesses associated with the metabolic syndrome, including obesity, hypertension, dyslipidemia, and glucose intolerance.1. By the year 2010, there could be as many as 50 to 75 million people in the United States with manifestations of the metabolic syndrome.2. References. 1. Kalff KG, et al. Aviat Space Environ Med Dec;70(12): Hansen BC. Ann N Y Acad Sci Nov 18;892:1-24. Kalff KG, et al. Aviat Space Environ Med Dec;70(12): Hansen BC. Ann N Y Acad Sci Nov 18;892:1-24.")
21
Das metabolische Syndrom
Definition Prevalence (Haufigkeit) Pathophysiologie Entstehen Komplikationen, Folgen Behandlung
 Pathophysiologie. Entstehen. Komplikationen, Folgen. Behandlung.")
22
Die Patogenese des metabolischen Syndroms

23
Mitokondriale Defekte Katecholamine Steroide METABOLISCHE SYNDROME
Welche Faktoren ? Mitokondriale Defekte STRESS Adipozytokine Radicale Metabolische Gedächtnis metabolische Set-Points Neuropeptide Toxine Katecholamine Steroide Insulinresistenz METABOLISCHE SYNDROME

24
Das metabolische Syndrome und associirte CV Risikofaktoren
Hochdruck Abdominale Obesität Atherosclerose Hyperinsulinaemie Insulin Wiederstand Diabetes Hypercoagulabilität The metabolic syndrome is characterized by insulin resistance, visceral distribution of body fat, dyslipidaemia, hypertension, and a prothrombotic state. All the components of the metabolic syndrome are associated with endothelial injury and dysfunction, the primary event that results in atherosclerosis. In particular, it is characterised by the lipid triad of elevated triglycerides, low high-density lipoprotein (HDL), and small, dense low-density lipoprotein (LDL) particles.1 Reference 1. Deedwania PC. Am J Med 1998;105(1A);1S-3S. Endotheliale Dysfunktion Dyslipidaemie TG “small dense” LDL HDL Deedwania PC. Am J Med 1998;105(1A);1S-3S.
, and small, dense low-density lipoprotein (LDL) particles.1. Reference. 1. Deedwania PC. Am J Med 1998;105(1A);1S-3S. Endotheliale Dysfunktion. Dyslipidaemie. TG small dense LDL. HDL Deedwania PC. Am J Med 1998;105(1A);1S-3S.")
25
Regulationsstörungen
Adipositas Insulin Resistence Regulationsstörungen Pro- inflammatorische Zustand Atherogene Dyslipidemie KW: metabolic syndrome, MS, risk factors, obesity, insulin resistance Pro- thrombotische Zustand Glucose Hochdruck

26
Das metabolische Syndrom
Androide Obesität Atherogenie dyslipidaemie - TG > 1,7; HDL-C < 1 mmol/l ; „small-dense”, oxidierte LDL ; apo B > 1,2 g/L Hochdruck Inzulin resistance / Hyperinsulinaemia (FG, IGT, „clamp”, inzulin Spiegel, HOMA) Pro-inflammatorische Zustand ESR; WBC; hsCRP > 5 mg/L Prothrombotic Zustand Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa Microalbuminurie Urine Albumine > 150 mg/h Microvasculäre angina
 Pro-inflammatorische Zustand. ESR; WBC; hsCRP > 5 mg/L. Prothrombotic Zustand. Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa. Microalbuminurie. Urine Albumine > 150 mg/h. Microvasculäre angina.")
27
Obesität Relative Risiko von Typ 2 Diabetes 100 80 60 40 20 <22
93.2 80 60 54.0 40.3 40 27.6 20 15.8 8.1 1.0 2.9 4.3 5.0 <22 22.0– 22.9 23.0– 23.9 24.0– 24.9 25.0– 26.9 27.0– 28.9 29.0– 30.9 31.0– 32.9 33.0– 34.9 35 BMI (kg/m2) Colditz et al.Ann Intern Med 1995; 122: 481-6
 Colditz et al.Ann Intern Med 1995; 122:")
28
Zentrale Obesität (CETP) VLDL-apoB Intra-abdominale Fet
Insulin resistance Freie Fetsäuren TG Small, dense LDL HDL/HDL2 Cascade of events in the metabolic syndrome. KW: risk factor, lipoprotein, HDL, triglyceride, Hepatische Lipase Brunzell 2001

29
Obesität und Koronarerkrankung: 26 -Jahre Inzidence in Man
<50 years 50+ years 600 500 440 366 400 350 333 300 255 Incidence/1,000 177 200 100 KW: metabolic syndrome, MS, CHD, risk factor, obesity, men, BMI, Framingham <25 25-<30 30+ BMI Framingham Herz Studie Hubert HB et al. Circulation 1983;67:

30
Intra-abdominale (viscerale) Fett Das gefärliche innere Fett!
Front Viscerale Fett KW: abdominal obesity, metabolic syndrome, visceral fat, Subcutane Fett Back 3

31
-der Taillenumfang zwischen Untere Rippen und die Hüfte. -CT
Abdominale Fett: Abmessung -der Taillenumfang zwischen Untere Rippen und die Hüfte. -CT Despres et al. BMJ 322:716,2001

32
Viscerale Adipositas und kardiovasculäre Risiko
OGTT Glucose Insulin 1 1,2 15.0 200 400 800 1000 1200 600 Areal 1,2 1,2 Areal 12.0 1 1,2 1,2 1 1 1,2 9.0 1,2 1 1 (mmol/l) (pmol/l) 1 1,2 1 1 1,2 6.0 Nonobese Obese VF niedrig Obese VF hoch 1,2 3.0 1,2 KW: abdominal obesity, metabolic syndrome, glucose, insulin, visceral fat, 0.0 -30 30 60 90 120 150 180 -30 30 60 90 120 150 180 Time (min) Time (min) 1 significant vs nicht Obes 2 significant vs Obes mit niedrige VF VF: viscerale Fettgewebe (VAT: visceral adipos tissue Pouliot MC et al.: Diabetes (1992) 41: 1
 (pmol/l) 1. 1, , Nonobese. Obese VF niedrig. Obese VF hoch. 1, ,2. KW: abdominal obesity, metabolic syndrome, glucose, insulin, visceral fat, Time (min) Time (min) 1 significant vs nicht Obes. 2 significant vs Obes mit niedrige VF. VF: viscerale Fettgewebe. (VAT: visceral adipos tissue. Pouliot MC et al.: Diabetes (1992) 41:")
33
Endokrine Folgen der viscerale Adipositas
Insulin (pmol/L) Apo B (g/L) KW: abdominal obesity, metabolic syndrome, visceral fat, Teillenumfang (cm) Teillenumfang (cm)
 Apo B (g/L) KW: abdominal obesity, metabolic syndrome, visceral fat, Teillenumfang (cm) Teillenumfang (cm)")
34
Stress Selye Janos 1938 Stress = unspezifische Antwort der Körper auf irgendein Belastung WHO Definition 1998 Stress = Das integrierte Stressantwort ist Teil der homeostatische Gleichgewicht nötig für Evolution und Überleben. Veränderungen des endocrinen, neuralen und immune Antworte auf Stress spielen in der Etiologie und Pathogenese alle häufigsten Gesundheitsproblemen eine wesentliche Rolle.

35
Stress und Obesität Sociale Hierarchie Lärm Kronische Stress
beim Arbeit TV Zu vieles Essen Ungenügend Sport Scandale Arbeitslosigkeit Affäre

36
Stressregelung in Fettzellen IL-6 TNF- Adipozytokine
+ Hypothalamus ACTH CRH-R2 Gewichtsabnahme CRH Hypophyse IL-6 TNF- Adipozytokine CRH-R1 Gewichtsabnahme CRH-R2 + 11 HSD Adrenalocortex Kortisol CRH-Rezeptor Gewichtszunahme Stresscopin Viszerale Fettzunahme Insulinresistenz Proc Natl Acad Sci USA 2002;99:7484-9 Proc Natl Acad Sci USA 2002;99: Mol Psychiatry 2002;7:967-74 J Clin Endocrinol Metab 2001;86:2281-8 Diabetes 2000;49:532-8

37
Chronische Entzündung Aktivierung der CRH-POMC-Nebennieren Axe
Genetische Empfindlichkeit Stress Etiologie Chronische Entzündung Aktivierung der CRH-POMC-Nebennieren Axe Phenotypen Deprimiert Mager Deprimiert Obes Nicht Deprimiert Obes

38
Zusammenfassung der Pathomechanismus von IRS

39
Das metabolische Syndrom
Androide Obesität Atherogenie dyslipidaemie - TG > 1,7; HDL-C < 1 mmol/l ; „small-dense”, oxidierte LDL ; apo B > 1,2 g/L Hochdruck Inzulin resistance / Hyperinsulinaemia (FG, IGT, „clamp”, inzulin Spiegel, HOMA) Pro-inflammatorische Zustand ESR; WBC; hsCRP > 5 mg/L Prothrombotic Zustand Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa Microalbuminurie Urine Albumine > 150 mg/h Microvasculäre angina
 Pro-inflammatorische Zustand. ESR; WBC; hsCRP > 5 mg/L. Prothrombotic Zustand. Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa. Microalbuminurie. Urine Albumine > 150 mg/h. Microvasculäre angina.")
40
Triglyceride-reiche Lipoproteine: Größe, und Zusammensetzung

41
Exogene und Endogene Lipidtransport

42
Biochemie der Lipoprotein Metabolismus
Leber Arterienwand Macrophag Chylomicron remnant: Leber (Hepatozyten) aufnahme: LDL receptor related protein receptor. LDL : Leber aufnahme: LDL receptor Ox-LDL: Aufnahme bei Macrophagen: scavenger receptor class A (SR-A) oder CD36. Nascent HDL: entfernt cholesterol von Zellen durch ATP-binding cassette transporter-1 (ABC1). Lecithin-cholesterol acyltransferase (LCAT): Cholesterol Esterifizierung Reifung der nascent pre-b HDL (flach) ins a-HDL (Kugelformig). Lipoproteine mit ApoB: VLDL, IDL, - cholesteryl ester transfer protein (CETP). HDL Cholesteryl ester (CE) wird by hepatische scavenger receptor class B type I (SR-BI) Receptor entfernt. Santamarina-Fojo S, et al: Curr Opin Lipidol 2000, 11:
 aufnahme: LDL receptor related protein receptor. LDL : Leber aufnahme: LDL receptor. Ox-LDL: Aufnahme bei Macrophagen: scavenger receptor class A (SR-A) oder CD36. Nascent HDL: entfernt cholesterol von Zellen durch ATP-binding cassette transporter-1 (ABC1). Lecithin-cholesterol acyltransferase (LCAT): Cholesterol Esterifizierung. Reifung der nascent pre-b HDL (flach) ins a-HDL (Kugelformig). Lipoproteine mit ApoB: VLDL, IDL, - cholesteryl ester transfer protein (CETP). HDL Cholesteryl ester (CE) wird by hepatische scavenger receptor class B type I (SR-BI) Receptor entfernt. Santamarina-Fojo S, et al: Curr Opin Lipidol 2000, 11:")
43
HDL Metabolismus und reverse Cholesterol Transport
Figure 42 Chylomicrons are synthesized by the liver as well as the small intestine. Lipoprotein lipase lipolysis produces not only chylomicron remnants but also pre-b-HDL (also known as small HDL, surface remnants or nascent HDL). Pre-b-HDL is a primary acceptor of free cholesterol from the peripheral tissues (especially macrophages). Cholesterol and phospholipids are liberated from the peripheral tissues (via the ABCA-1 receptor). Large/spheric HDL is formed when pre-b-HDL binds with free cholesterol, apo A-I and apo A-II (both synthesized in the liver), a reaction catalyzed by lecithin cholesterol acyltransferase (LCAT). HDL may exert its cardioprotective effect by promoting cholesterol catabolism in two ways: HDL (acting as a reverse cholesterol transporter) travels to the liver, where it is recognized by the Cla-1/SR-B I receptor, ingested, and catabolized; HDL transfers CEs to TG-rich particles via cholesterol ester transfer protein (CETP) to form chylomicron remnants and LDL, which are then transported to tissues and catabolized. KW: lipids, lipoprotein, HDL, reverse cholesterol transport, ABCA-1, RCT, cholesterol efflux cholesteryl ester transfer protein (CETP). ATP-binding cassette transporter-1 (ABC1).
. Pre-b-HDL is a primary acceptor of free cholesterol from the peripheral tissues (especially macrophages). Cholesterol and phospholipids are liberated from the peripheral tissues (via the ABCA-1 receptor). Large/spheric HDL is formed when pre-b-HDL binds with free cholesterol, apo A-I and apo A-II (both synthesized in the liver), a reaction catalyzed by lecithin cholesterol acyltransferase (LCAT). HDL may exert its cardioprotective effect by promoting cholesterol catabolism in two ways: HDL (acting as a reverse cholesterol transporter) travels to the liver, where it is recognized by the Cla-1/SR-B I receptor, ingested, and catabolized; HDL transfers CEs to TG-rich particles via cholesterol ester transfer protein (CETP) to form chylomicron remnants and LDL, which are then transported to tissues and catabolized. KW: lipids, lipoprotein, HDL, reverse cholesterol transport, ABCA-1, RCT, cholesterol efflux. cholesteryl ester transfer protein (CETP). ATP-binding cassette transporter-1 (ABC1).")
44
Hypertriglyceridemie—Unabhängige Risikofaktor für Koronarerkrankung
150 132 93 100 81 Ereignisse/ 1,000 in 8 Jahren 44 50 KW: hypertriglyceridemia, CHD, risk factor, PROCAM, TG <200 (157/3,593) (84/903) (14/106) 800 (3/37) PROCAM Studie TG (mg/dL) Assmann G et al. Am J Cardiol. 1992;70:
 (84/903) (14/106) 800 (3/37) PROCAM Studie. TG (mg/dL) Assmann G et al. Am J Cardiol. 1992;70:")
45
Cardiovasculäre Erkrankungen
und HDL-C Spiegel 160 140 Männer Frauen 120 Rate per 1000 100 80 60 KW: CHD, risk factor, HDL, men, women, gender 40 20 <34 35-54 >55 <34 35-54 >55 HDL Cholesterol, mg/dL Kannel WB. Am J Cardiol. 1983;52:9B-12B.

46
Atherogene Dyslipidaemie:
hoche nüchtern Triglyceride-Spiegel Niedrige HDL-cholesterol "small-dense" LDL Postprandiale Hypertriglyceridaemie

47
Atherogene Dyslipidaemie
Metabolische Syndrome Hypercholesterolaemia Typ II Diabetes Gemischte Hyperlipidaemie Hypertriglyceridaemie Anti-atherogene HDL Atherogene LP mit Apo B VLDL VLDL Remnants IDL LDL; Dense LDL Low concentrations of HDL particles, manifesting as low levels of HDL cholesterol, are a characteristic feature of the major forms of dyslipidaemia that are encountered in clinical practice. In addition, they have elevated levels of atherogenic apolipoprotein B (apo B)-containing particles, especially small, dense LDL and VLDL. As a result, these patients have reduced reverse cholesterol transport and enhanced cholesterol deposition within the arterial wall leading to increased atherogenesis. KW: HDL, dyslipidemia, LDL, VLDL, apoB, sdLDL Cholesterol Ablagerung in die Arterien Reverse Cholesterol Transport Atherogenese
-containing particles, especially small, dense LDL and VLDL. As a result, these patients have reduced reverse cholesterol transport and enhanced cholesterol deposition within the arterial wall leading to increased atherogenesis. KW: HDL, dyslipidemia, LDL, VLDL, apoB, sdLDL. Cholesterol Ablagerung in die Arterien. Reverse Cholesterol Transport Atherogenese ")
48
Atherogenese durch „small dense” LDL
Figure 44 The accumulation of abnormal lipoprotein particles (e.g. Lp-B:C-III) results in abnormal VLDL, which is rich in apo C-III. The enzymatic breakdown of this abnormal VLDL produces large amounts of small dense LDL instead of large buoyant LDL. Small dense LDL is poorly recognized by the LDL receptor (the first part of the usual metabolic pathway) and, instead, it is recognized by non-regulated scavenger receptors on the surface of macrophages, which ingest it and eventually transform into foam cells. Thus, small dense LDL is more atherogenic, making the individual more susceptible to AS. Small dense LDL is common in diabetes, metabolic syndrome or combined dyslipidemia. KW: lipids, lipoprotein, sdLDL, small dense LDL
 results in abnormal VLDL, which is rich in apo C-III. The enzymatic breakdown of this abnormal VLDL produces large amounts of small dense LDL instead of large buoyant LDL. Small dense LDL is poorly recognized by the LDL receptor (the first part of the usual metabolic pathway) and, instead, it is recognized by non-regulated scavenger receptors on the surface of macrophages, which ingest it and eventually transform into foam cells. Thus, small dense LDL is more atherogenic, making the individual more susceptible to AS. Small dense LDL is common in diabetes, metabolic syndrome or combined dyslipidemia. KW: lipids, lipoprotein, sdLDL, small dense LDL.")
49
Zusammenhang zwischen LDL Größe und andere Lipidprofil Parametern
HDL cholesterol (mmol/l) Triglyceride (mmol/l) Chol/HDL chol 5.0 2.5 10.0 r=-0.52 p<0.0001 r=0.44 p<0.0001 r=-0.45 p<0.0001 4.0 2.0 8.0 3.0 1.5 6.0 2.0 1.0 4.0 1.0 0.5 2.0 KW: triglycerides, HDL, lipoprotein, LDL, risk factor, dense LDL, 235 240 245 250 255 260 265 270 235 240 245 250 255 260 265 270 235 240 245 250 255 260 265 270 LDL Größe (Å) LDL Größe (Å) LDL Größe (Å) Després JP: Ann Med (2001) 33:
 Triglyceride. (mmol/l) Chol/HDL chol r= p< r=0.44. p< r= p< KW: triglycerides, HDL, lipoprotein, LDL, risk factor, dense LDL, LDL Größe (Å) LDL Größe (Å) LDL Größe (Å) Després JP: Ann Med (2001) 33:")
50
Apo B, LDL Größe und chronische Herzkrankheit Risiko
7 6.20 6 5 Odds Ratio for CHD Apo B 4 Kleiner LDL Größere LDL 2.00 3 KW: CHD, risk factor, apoB, LDL, Quebec 2 1.00 1 120 mg/dL größte LDL durchmesser (nm) >25.64 <120 mg/dL 25.64 Quebec Studie Lamarche B, et al. Circulation. 1997;95:69-75.
 > <120 mg/dL. Quebec Studie. Lamarche B, et al. Circulation. 1997;95:")
51
Das metabolische Syndrom
Androide Obesität Atherogenie dyslipidaemie - TG > 1,7; HDL-C < 1 mmol/l ; „small-dense”, oxidierte LDL ; apo B > 1,2 g/L Hochdruck Inzulin resistance / Hyperinsulinaemia (FG, IGT, „clamp”, inzulin Spiegel, HOMA) Pro-inflammatorische Zustand ESR; WBC; hsCRP > 5 mg/L Prothrombotic Zustand Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa Microalbuminurie Urine Albumine > 150 mg/h Microvasculäre angina
 Pro-inflammatorische Zustand. ESR; WBC; hsCRP > 5 mg/L. Prothrombotic Zustand. Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa. Microalbuminurie. Urine Albumine > 150 mg/h. Microvasculäre angina.")
52
Titolo: Haemodynamic consequences of the metabolic syndrome
Haemodynamic consequences of the metabolic syndrome (pressure and volume overload), mostly related to hyperinsulinemia, not only predispose to arterial hypertension but also to cardiac overload. KW: obesity, dyslipydemia, hypertension, diabetes, fatty acid, abdominal fat, insulin, insulin resistance
, mostly related to hyperinsulinemia, not only predispose to arterial hypertension but also to cardiac overload. KW: obesity, dyslipydemia, hypertension, diabetes, fatty acid, abdominal fat, insulin, insulin resistance.")
53
Das metabolische Syndrom
Androide Obesität Atherogenie dyslipidaemie - TG > 1,7; HDL-C < 1 mmol/l ; „small-dense”, oxidierte LDL ; apo B > 1,2 g/L Hochdruck Inzulin resistance / Hyperinsulinaemia (FG, IGT, „clamp”, inzulin Spiegel, HOMA) Pro-inflammatorische Zustand ESR; WBC; hsCRP > 5 mg/L Prothrombotic Zustand Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa Microalbuminurie Urine Albumine > 150 mg/h Microvasculäre angina
 Pro-inflammatorische Zustand. ESR; WBC; hsCRP > 5 mg/L. Prothrombotic Zustand. Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa. Microalbuminurie. Urine Albumine > 150 mg/h. Microvasculäre angina.")
54
Kardiovasculäre Erkrankungen in Typ II Diabetes
mit niedrige HDL-Cholesterol Spiegel Hyperglycemie Hochdruck Fibrinolyse Atherogene Dyslipidemie Insulin Resistance Hyperinsulinemie Entzündlcihe Zusatnad Simplified overview of the "metabolic syndrome iceberg" underlying the hyperglycemic state of the abdominally obese patients with the metabolic syndrome or type 2 diabetes. Thus, hyperglycemia only represents the tip of a huge athero-thrombotic, inflammatory profile resulting from the presence of abdominal obesity and associated with a substantially increase in the risk of cardiovascular disease. KW: metabolic syndrome, risk factors, CHD, diabetes, HDL Abdominale obesität Hyperglycemie: Spitze des Eisberg des metabolischen Syndrom

56
Häufigkeit (Prevalence) von Typ II und Typ I Diabetes. 1997-2O1O
Millionen Jahr EHJ, 2OO3, Suppl.B6

57
DeFronzo RA et al., Diabetes Care 1998
Type 2 Diabetes Diabetes Diagnose Insulin Resistance Proinsulin Freisetzung FFA Insulin Blut Glucose Normale Glukose Tolerance impaired Glukose Tolerance Diabetes IFG DeFronzo RA et al., Diabetes Care 1998

58
DeFronzo RA et al., Diabetes Care 1998
? ? ? Insulin Glucose Normal Prädiabetes impaired Glucose Tolerance Diabetes IFG DeFronzo RA et al., Diabetes Care 1998

59
WHO Obesität Primäre (Genetische) Insulin Resistance Pro- Atherogene
Physische Inactivität Primäre (Genetische) Insulin Resistance Pro- inflammatorische Zustand Atherogene Dyslipidemie KW: metabolic syndrome, MS, risk factors, obesity, insulin resistance, WHO Pro- thrombotische Zustand Blut Hochdruck Glucose Spiegel
 Insulin Resistance. Pro- inflammatorische. Zustand. Atherogene. Dyslipidemie. KW: metabolic syndrome, MS, risk factors, obesity, insulin resistance, WHO. Pro- thrombotische. Zustand. Blut. Hochdruck. Glucose. Spiegel ")
60
Zusammenhang :Zentral abdominale Fett (Rtg) und Empfindlichkeit auf Insulin (clamp)
Carey et al. Diabetes 45:633, 1996

61
Ser/Thr phosphorylierung von IRS Moleküle induziert Insulin Resistence
Insulin Rezeptor Signalübertragung Ser/Thr phosphorylierung von IRS Moleküle induziert Insulin Resistence Le Roith et al., Diabetes Care 24:588 (2001)
")
62
Zusammenhang zwischen freie Fettsäurenspiegel und Insulinresistance in gestreifte Muskulaturzellen
Randle et al.: J Clin Invest 106:171, 2000

63
Psychosociale Stress Fettsäurenspiegel :
Type A Personalität, Anxietät, Depression, Arbeitslosigkeit, vitale Erschöpfung, Gehaltsunterschiede Hemingway et al.,BMJ 318:1460 (1999)
")
64
Depression und Mortalität nach AMI
Überleben P<0.001 In patients with MI degree of depression predicts mortality. KW: mortality, depression, MI BDI=Beck Depression Inventory Tagen nach Miokardinfarkt Lespérance F & al.Circulation 2002;105:1049

65
Das metabolische Syndrom
Androide Obesität Atherogenie dyslipidaemie TG > 1,7; HDL-C < 1 mmol/l ; „small-dense”, oxidierte LDL ; apo B > 1,2 g/L Hochdruck Inzulin resistance / Hyperinsulinaemia (FG, IGT, „clamp”, inzulin Spiegel, HOMA) Pro-inflammatorische Zustand ESR; WBC; hsCRP > 5 mg/L Prothrombotic Zustand Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa Microalbuminurie Urine Albumine > 150 mg/h Microvasculäre angina
 Pro-inflammatorische Zustand. ESR; WBC; hsCRP > 5 mg/L. Prothrombotic Zustand. Lp(a) > 40 mg/dL; fibr.:3,85 g/L; PAI-1, tPa. Microalbuminurie. Urine Albumine > 150 mg/h. Microvasculäre angina.")
66
Proinflammatorische Zustand
Proinflammatorishce Zytokine (IL-6 & TNF) Adiponectin Akutphasenproteine (AFP) weitere Steigerung der Entzündung C-reactive Protein (CRP) Fibrinogen Serum Amyloid A KW: inflammation, cytokine
 Adiponectin. Akutphasenproteine (AFP) weitere Steigerung der Entzündung. C-reactive Protein (CRP) Fibrinogen. Serum Amyloid A. KW: inflammation, cytokine.")
67
Proinflammatorische Zustand
Fett gewebe Leber Zytokine Unstabiles Plaque CRP KW: inflammation, cytokine, adipocyte, liver, CRP Apo B Diabetes HDL Prothrombotische Zustand

68
Monozytenaktivierung durch das metabolische Syndrom
Leber Leber Fettgewebe Leber verfettung NASH TG / HDL Adipo Q, Leptin CRP b-carotene, Retinoide PPARg Agonisten Glucose AGE frei Fettsäuren Small dense LDL S1P, LPA, TGFb Monozyt Platchen atherogene Lipoproteine aktivierte Endothezelle calcifizierung Osteoblast Osteoclast Modifizierte LDL activierte mesenchymale Zellen calcifizierte Lesion lipid reich Lesion Schaumzelle PD Dr. Thomas Langmann Inst fürClinische Chemie und Laboratorische Medicine Universität Regensburg

69
Endothelstress durch Eisen
Hemopexin Haptoglobin Fe Hemoglobin H2O2 O2- • Fe Fe Fe Methemoglobin H2O2 O2- • Fe Fe Fe Sensitizierung Stress Adaptation CO Fe Fe Fe Heme Abbau Bilirubin Fe Fe HO-1 Fe Fe Fe Oxidative Schaden Oxidative wiederstand Ferritin Endothelium Ferroxidase Eisenspeicher Erythrozyt Mononucleare Zelle Polymorphonucleare Zelle LDL Fe Heme Balla J. et al. J Biol Chem. 1992;267: Balla J. et al. PNAS. 1993;90: Balla J. et al. Blood. 2002;100: Balla J. et al. Kidney Int. 2006;69: Endothelstress durch Eisen

70
Folgen der Entzündliche Zustand

73
Das metabolische Syndrom
Definition Prevalence (Haufigkeit) Pathophysiologie Entstehen Komplikationen, Folgen Behandlung
 Pathophysiologie. Entstehen. Komplikationen, Folgen. Behandlung.")
75
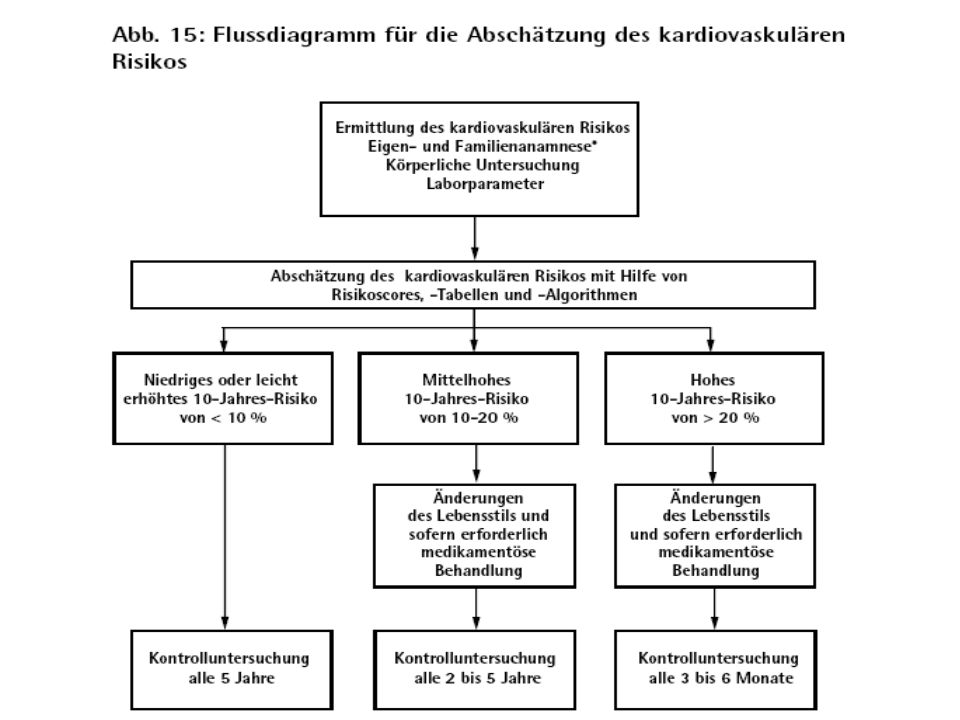
Lebensstyl vs. Medikamentöse Behandlung
Bekannte Studien Lebensstyl Metformin Sulph Acarbose TZD Orlist absolut Da Quing % DPS % % DPP % % % Metf. 8% TRIPOD % % STOP-NIDDM % % XENDOS % % Chinese Study % % % Herlihy et al. Diabetologia 2000, Wenying, et al. Chinese J. Endocrinol Chiasson JL, et al. Lancet 2002 Pan XR et al. Diabetes Care 1997; 20: , Tuomilehto et al. N Engl J Med 2001; 344: , Knowler WC et al. N Engl J Med 2002; 346:

76
Motivation ! Ziel der Behandlung Körpergewicht >5%
Fett einnahme < 30% (der tägliche Energiezufuhr) Saturiertes fett einnahme < 10% (täglich) Fibre einnahme 15g/1000 kcal Physicalische Aktivität 4 Stunden/woche Motivation ! Schwarz P. et al. TUMAINI Präventionsprogramm, Diabetes und Stoffwechsel 09/2003 Tuomilehto et al. N Engl J Med 2001; 344:
 Saturiertes fett einnahme < 10% (täglich) Fibre einnahme 15g/1000 kcal. Physicalische Aktivität 4 Stunden/woche. Motivation ! Schwarz P. et al. TUMAINI Präventionsprogramm, Diabetes und Stoffwechsel 09/2003. Tuomilehto et al. N Engl J Med 2001; 344:")
77
normale impaired (IGT) Typ II Diabetes ß-Zellen Funktion Glucose Insulin Resistance
 Typ II Diabetes ß-Zellen Funktion Glucose Insulin Resistance")
78
Sport Fitness IGF,GH Stress Kalorien Cortisol

79
ApoA-I/C-III/A-IV/A-V
Gene associert mit familiale combinierte hyperlipidemie und dem metabolischen syndrom USF1 PDX1 Renin FAS/HSL ABCA1 Insulin Blood Pressure Lipogenesis/ TG hydrolysis HDL 11q21 1q21 20q13 HNF4a ApoA-I Insulin ApoC-III GLUT2 ApoA-IV Aldolase ApoA-V GAPDH FABP1 Glucokinase ApoA-I/C-III/A-IV/A-V USF1 HNF4a Triglyceride/ HDL metabolism Glucose metabolism Shoulders et al., 2004 PD Dr. Thomas Langmann Inst Clin Chem und LabMed Uni Regensburg

Ähnliche Präsentationen













>")



>")


