Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
14. Zürcheroberländer Gastro-Meeting 2014
Update und praxisrelevante Aspekte der Gastroenterologie

2
17. 30. Refluxkrankheit. Dr. Alf Karpf 17. 55
17.30 Refluxkrankheit Dr. Alf Karpf Neues und altes zum Reizdarm Dr. Hansueli Ehrbar Pause Fettleber Dr. Georg Bansky Erhöhte Amylase! Wie weiter ? Was der Grundversorger wissen muss. Dr. Marco Bernardi Roundtable – Diskussion Nachtessen

3
Fit in Gastroenterologie 2015 Schifflände Maur
Mittwoch, 21. Januar 2015 17.30 h Gastrointestinale Blutung Emesis Dyspepsie und Helicobacter pylori Colitis ulcerosa Therapie und Verlaufskontrolle

4
Refluxkrankheit Dr. Alf G. Karpf Facharzt Gastroenterologie FMH
Facharzt Innere Medizin FMH Poststr. 2, 8610 Uster

5
Befindlichkeitsstörung oder schwerwiegende Erkrankung ?
Reflux Befindlichkeitsstörung oder schwerwiegende Erkrankung ? Sowohl als auch!

6
Refluxrankheit - Epidemiologie
Prävalenz Hausarzt- besuch % 20 %

7
Refluxkranheit - Epidemiologie
Peptische Reflux Funktionelle Läsionen Dyspepsie % % > 50 % % 20 – 40 % > 50 %

8
Body-Mass Index und Reflux
Risikofaktoren: BMI und Rauchen BMI „lineare“ Abhängigkeit „Dosis-Wirkung-Beziehung“ BMI > 30: Risiko 3x erhöht Body-Mass Index and Symptoms of Gastroesophageal Reflux in Women B.C. Jacobsen et.al. NEJM 2006

9
Refluxkrankheit - Epidemiologie
NERD GERD Hiatus- hernie Patholog. Reflux Oeso- phagitis Barrett- Oesoph. Adeno- karzinom 10 % 10 % 10 % 10 % 50 % 5 % 0.5 % 0.05 % 0.005 %

10
Los Angeles Klassifikation Refluxoesophagitis Stadium A
The LA Classification – Grade A reflux esophagitis Under the LA Classification system,18 Grade A reflux esophagitis is defined as one (or more) mucosal break, no longer than 5 mm, that does not extend between the tops of two mucosal folds. This is shown here schematically, together with an endoscopy image of typical Grade A reflux esophagitis. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent
 mucosal break, no longer than 5 mm, that does not extend between the tops of two mucosal folds. This is shown here schematically, together with an endoscopy image of typical Grade A reflux esophagitis. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent.")
11
Los Angeles Klassifikation Refluxoesophagitis Stadium B
The LA Classification – Grade B reflux esophagitis Grade B reflux esophagitis is defined as one (or more) mucosal break, more than 5 mm long, that does not extend between the tops of two mucosal folds, according to the LA Classification system.18 Grade B reflux esophagitis is shown here schematically, together with a typical endoscopy image. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent
 mucosal break, more than 5 mm long, that does not extend between the tops of two mucosal folds, according to the LA Classification system.18 Grade B reflux esophagitis is shown here schematically, together with a typical endoscopy image. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent.")
12
Los Angeles Klassifikation Refluxoesophagitis Stadium C
The LA Classification – Grade C reflux esophagitis According to the LA Classification system,18 Grade C reflux esophagitis is defined as one (or more) mucosal break that is continuous between the tops of two or more mucosal folds, but which involves less than 75% of the circumference. This is shown here schematically, together with an endoscopy image of typical Grade C reflux esophagitis. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent
 mucosal break that is continuous between the tops of two or more mucosal folds, but which involves less than 75% of the circumference. This is shown here schematically, together with an endoscopy image of typical Grade C reflux esophagitis. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent.")
13
Los Angeles Klassifikation Refluxoesophagitis Stadium D
The LA Classification – Grade D reflux esophagitis Grade D reflux esophagitis is defined as one (or more) mucosal break that involves at least 75% of the esophageal circumference under the LA Classification system.18 Grade D reflux esophagitis is shown here schematically, together with a typical endoscopy image. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent
 mucosal break that involves at least 75% of the esophageal circumference under the LA Classification system.18 Grade D reflux esophagitis is shown here schematically, together with a typical endoscopy image. Lundell et al 1999, Published with permission from Professor G Tytgat and Professor J Dent.")
14
Refluxkrankheit - Epidemiologie
NERD GERD Hiatus- hernie Patholog. Reflux Oeso- phagitis Barrett- Oesoph. Adeno- karzinom 10 % 10 % 10 % 10 % 50 % 5 % 0.5 % 0.05 % 0.005 %

15
Epidemiologie Barrett-Prävalenz US 5.6%!
Long segment Barrett > 3 cm Short segment Barrett < 3 cm Hayeck et al. Dis Esophagus 2010

16
Barrett Definition Barrett oder Endobrachyösophagus ist ein prämaligner metaplastischer Prozess, bei dem das Plattenepithel des distalen Oesophagus durch ein spezialsiertes intestinales Zylinderepithel (Dünndarm) mit Becherzellen ersetzt ist, welches resistenter ist gegenüber Säure und Galle. Diagnose: Endoskopie mit Biopsie
 mit Becherzellen ersetzt ist, welches resistenter ist gegenüber Säure und Galle. Diagnose: Endoskopie mit Biopsie.")
17
Spechler SJ, Souza RF. N Engl J Med 2014;371:836-845.
Diagnostic Features of Barrett's Esophagus Figure 1. Diagnostic Features of Barrett's Esophagus. The diagnosis of Barrett's esophagus requires endoscopic evidence that columnar mucosa extends above the gastroesophageal junction and lines the distal esophagus, plus esophageal-biopsy results that confirm the presence of columnar metaplasia. Endoscopically, the gastroesophageal junction is identified as the most proximal extent of the gastric folds (dashed white line). Salmon-colored columnar mucosa extends in tongue-shaped projections above the gastroesophageal junction, lining the distal esophagus. A biopsy specimen obtained at the level of the upper white dot reveals the junction between esophageal stratified squamous epithelium and intestinal metaplasia with distinctive, intestinal-type goblet cells, which establishes the diagnosis of Barrett's esophagus. Intestinal metaplasia may not be uniformly distributed throughout the entire columnar-lined esophagus, however. In this example, a biopsy specimen taken from the columnar-lined esophagus closer to the gastroesophageal junction (at the level of the lower white dot) shows cardiac mucosa composed of mucus-secreting columnar cells without goblet cells. Some gastroenterology societies (e.g., the British Society of Gastroenterology) accept evidence of cardiac mucosa alone as diagnostic of Barrett's esophagus, but U.S. gastroenterology societies require evidence of intestinal metaplasia for a definitive diagnosis. Photomicrographs (hematoxylin and eosin) provided by Drs. Kevin Turner and Robert Genta. Spechler SJ, Souza RF. N Engl J Med 2014;371:
. Salmon-colored columnar mucosa extends in tongue-shaped projections above the gastroesophageal junction, lining the distal esophagus. A biopsy specimen obtained at the level of the upper white dot reveals the junction between esophageal stratified squamous epithelium and intestinal metaplasia with distinctive, intestinal-type goblet cells, which establishes the diagnosis of Barrett s esophagus. Intestinal metaplasia may not be uniformly distributed throughout the entire columnar-lined esophagus, however. In this example, a biopsy specimen taken from the columnar-lined esophagus closer to the gastroesophageal junction (at the level of the lower white dot) shows cardiac mucosa composed of mucus-secreting columnar cells without goblet cells. Some gastroenterology societies (e.g., the British Society of Gastroenterology) accept evidence of cardiac mucosa alone as diagnostic of Barrett s esophagus, but U.S. gastroenterology societies require evidence of intestinal metaplasia for a definitive diagnosis. Photomicrographs (hematoxylin and eosin) provided by Drs. Kevin Turner and Robert Genta. Spechler SJ, Souza RF. N Engl J Med 2014;371:")
18
Barrett-Oesophagus

19
Barrett Irreversibel. Keine „Heilung“ durch hoch dosierte PPI-Therapie oder Anti-Refluxchirurge(Fundoplicatio) Barrettmukosa hat ein kleines aber nicht vernachlässigbares Risiko für die Entwicklung eines Adenokarzinoms Barrettmukosa kann endoskopisch „zerstört“ werden

20
Refluxkrankheit Behandlungsziele
Beschwerdefreiheit Komplikationen vermeiden

21
Refluxkrankheit - Komplikationen
NERD GERD Barrett- Oesophagus Nicht progressiv, extraösophageale Manifestationen Striktur, Ulkus, Blutung, extraösophageale Manifestationen Adeno- karzinom

22
Fallvorstellung 1 1949 m 1954 Lungentuberkulose 2002 Herpes zoster
2006 Barrettösophagus ED 2009 Barrettösophagus Nichtraucher Alkohol, unregelmässig, <100 g/Woche Medikamente: Agoptopn 15 mg/Tag

23
Überwachungsgastroskopien bei Barrett-Oesophagus
2006 2009 2013

24
Fallvorstellung 1 Diagnose Barrettösophagus, High grade Dysplasie
Therapie Mukosektomie USZ Prof. P. Bauerfeind Barrettkarzinom pT1a(m3) G2, L0, V0 Radiofrequenzablation (BarrxTM) für Restbarrett PPI und Zantic
 G2, L0, V0. Radiofrequenzablation (BarrxTM) für Restbarrett. PPI und Zantic.")
25
Fallvorstellung 2 1958 m 2000 Chronische Refluxkrankheit ED
2005 Barrettösophagus ED Biopsie: keine Dysplasie Nikotin PY Alkohol regelmässig, g/Woche Medikamente: Gelomyrtol regelmässig, PPI selten

27
Fallvorstellung 2 Selbständiger Unternehmensberater Vater 77 LJ Bronchuskarzinom (Raucher) Aktuelle Beschwerden Dysphagie seit 4 bis 6 Wochen Retrosternales Brennen bei Orangensaft/Weisswein Gewicht konstant, BMI 30 kg/m2, guter AZ

29
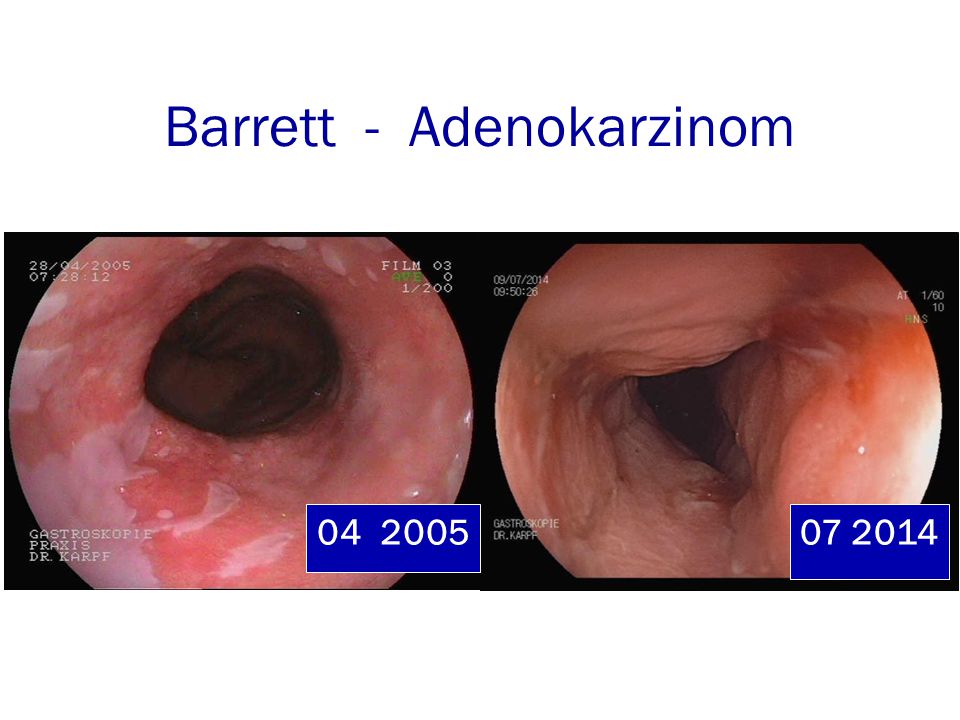
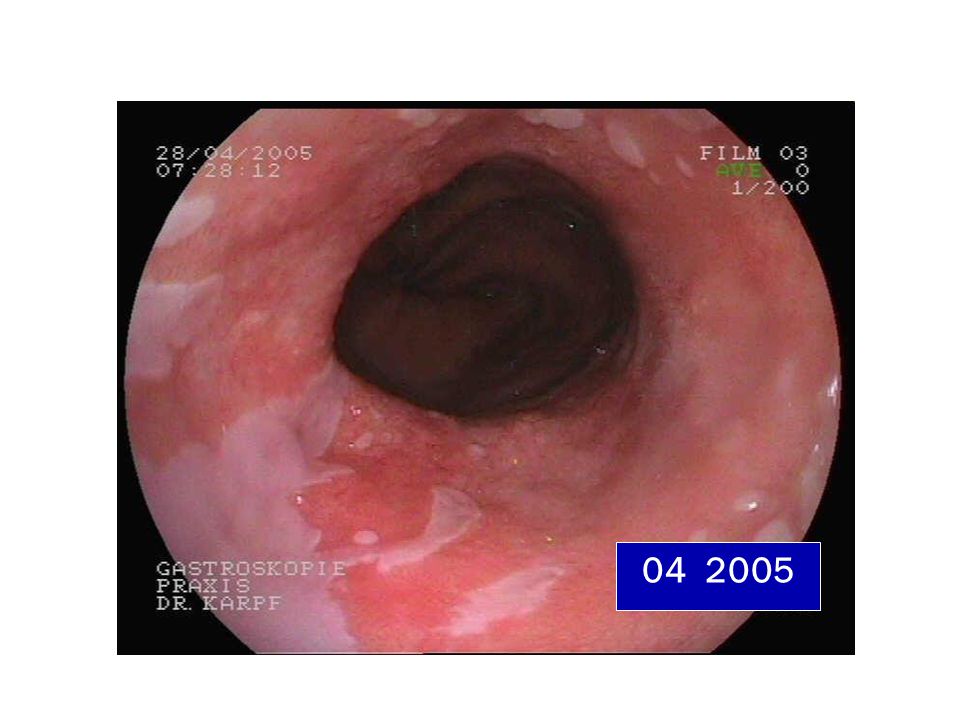
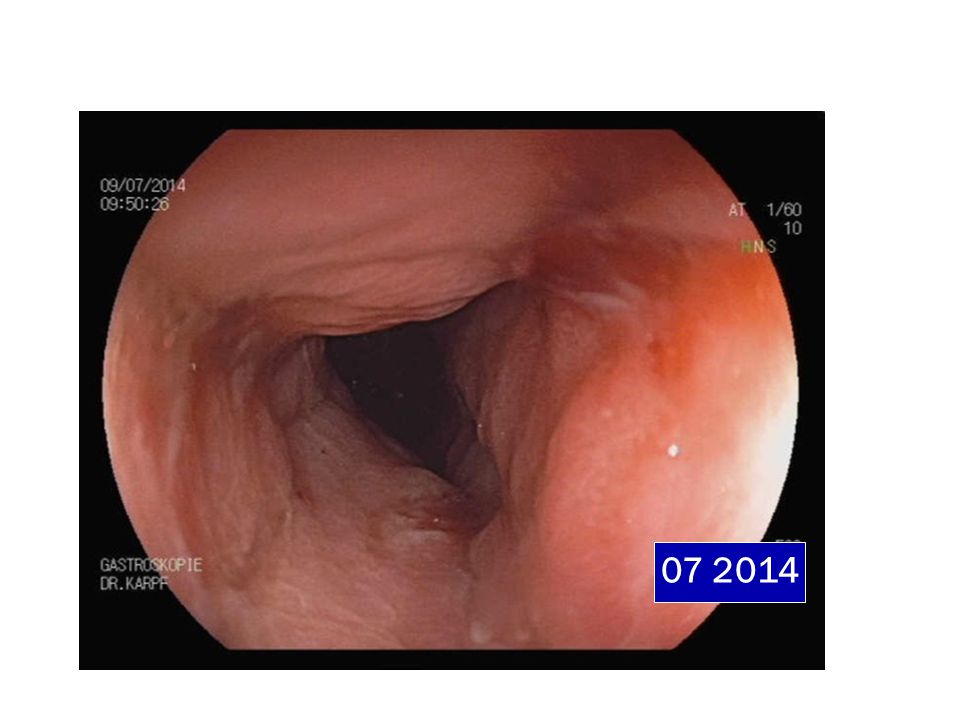
Barrett - Adenokarzinom
30
Fallvorstellung 2 Diagnose Adenocarcinom im Barrett-Oesophagus
C,uT2-3, uN1, cM1 (paraaortal,Cy) Barrettösophagus (ED 2005) Kolonpolypen (Tubuläre Adenome, LGD) Sigmadivertikulose Adipositas Chronischer Nikotin und Alkoholkonsum
 Barrettösophagus (ED 2005) Kolonpolypen (Tubuläre Adenome, LGD) Sigmadivertikulose. Adipositas. Chronischer Nikotin und Alkoholkonsum.")
31
Fallvorstellung 2 Therapie Port-Implantation
4 Zyklen Chemotherapie FLOT Protokoll Metabolische frühresponse Re-Evaluation Ev. Radiochemotherapie nach Cross-Studie Nach 4. Chemozyklus PET-CT, Relaparoskopie Abdominothorakale en bloc Oesophagektomie

32
Fazit Fallvorstellungen
Reflux ist nicht harmlos! Das Oesophaguskarzinom hat eine schlechte Prognose 3 Jahresüberleben 30 bis 60% 5 Jahresüberleben 20%

33
Lagergren, Bergström et al. NEJM 1999
Refluxkrankheit SYMPTOMATIC GASTROESOPHAGEAL REFLUX AS A RISK FACTOR FOR ESOPHAGEAL ADENOCARCINOMA Adenokarzinom Kardiakarzinom Odds-Ratio Chronischer Reflux (1x Woche) Nächtlicher Reflux Schwerer Reflux Adenokarzinom % Barrett-Oesophagus Lagergren, Bergström et al. NEJM 1999
 Nächtlicher Reflux Schwerer Reflux Adenokarzinom 62% Barrett-Oesophagus. Lagergren, Bergström et al. NEJM")
34
Barrett Screening ? Surveillance? Therapie? Mukosektomie?
Radiofrequenzablation(RFA), BarrxTM Operation
, BarrxTM. Operation.")
35
Barrett Kein Screening in der Allgemein-Bevölkerung
BSG Guidelines GUT 2013 Hvid-Jensen Fed al. N Engl J Med 2011;365:

36
Barrett Karzinominzidenz
% % % % Computermodell 0.5% Inzidenz: Surveillance Intervall 4 Jahre Ann Intern Med 2012:157(11):
:")
37
Surveillance Die langsame Progression prämaligner Läsionen im Barrett zum Karzinom ist die Ratio für eine Überwachungsstrategie Es gibt keine wissenschaftlich gesicherte Evidenz für eine Reduktion der Mortalität durch eine Surveillance Es gibt Hinweise, dass die Karzinome, die im Rahmen einer Surveillance entdeckt werden, eine bessere Prognose haben.

38
Risikofaktoren für Barrett und Adenokarzinom des Oesophagus
Alter, Kaukasier, Männer, Raucher, Chronischer Reflux Ja Adipositas (viszerale Adipositas), Metabolisches Syndrom Erosive Oesophagitis, Axiale Hiatushernie Positive Familienanamnese, Fleischkonsum GERD Erstdiagnose < 30 Jahre - Schlafapnoe Frühgeburt Nein Tiefes Geburtsgewicht HPV-Infektion St.J.Spechler N Engl J Med 2014;371:836-45
, Metabolisches Syndrom. Erosive Oesophagitis, Axiale Hiatushernie. Positive Familienanamnese, Fleischkonsum. GERD Erstdiagnose < 30 Jahre. - Schlafapnoe. Frühgeburt. Nein. Tiefes Geburtsgewicht. HPV-Infektion. St.J.Spechler N Engl J Med 2014;371:")
39
Protektive Faktoren für Barrett und Adenokarzinom des Oesophagus
NSAR, Statin-Therapie Ja Helicobacter pylori Infektion Hoher Früchte- und Gemüsekonsum Exposition UV-Strahlung - Stillende Frauen Hochgewachsene St.J.Spechler N Engl J Med 2014;371:836-45

40
Barrett Screening Hochrisikogruppen
> 50 Lebensjahr und chronischer Reflux Männer, Raucher, Adipositas Surveillance: Endoskopie mit Biopsie alle 3 bis 5 Jahre (2 Jahre in Hochrisikogruppe)
")
41
Dysplasie.. und jetzt? 2/3 der low grade Dysplasie (LGD) bleiben stabil oder sind regressiv Ein Teil der LGD sind regressiv (60-85%) Ein kleiner Teil zeigt ein Progression zu einer high grade Dysplasie (HGD) (10-28%) Follow up 26 bis 48 Monate Skacel et al. Am J Gastroenterol 1999 Weston et al. Am J Gastroenterol 2001
 (10-28%) Follow up 26 bis 48 Monate. Skacel et al. Am J Gastroenterol Weston et al. Am J Gastroenterol")
42
Cumulative Incidence of Esophageal Adenocarcinoma and of Esophageal Adenocarcinoma or High-Grade Dysplasia Figure 2. Cumulative Incidence of Esophageal Adenocarcinoma and of Esophageal Adenocarcinoma or High-Grade Dysplasia. Shown is the cumulative incidence of esophageal adenocarcinoma (Panel A) and of esophageal adenocarcinoma or high-grade dysplasia (Panel B) among patients with Barrett's esophagus, according to the presence or absence of low-grade dysplasia on baseline endoscopy. Kaplan–Meier plots include data from the first year after the index endoscopy. Hvid-Jensen Fed al. N Engl J Med 2011;365:
 and of esophageal adenocarcinoma or high-grade dysplasia (Panel B) among patients with Barrett s esophagus, according to the presence or absence of low-grade dysplasia on baseline endoscopy. Kaplan–Meier plots include data from the first year after the index endoscopy. Hvid-Jensen Fed al. N Engl J Med 2011;365:")
43
Dysplasie LGD und Erosionen: PPI und Kontrollbiopsie in einigen Monaten LGD kann transient sein, nur ein kleiner %-Satz entwickelt eine HGD HGD hat ein hohes Karzinomrisiko

44
Surveillance Endoskopie Stufenweise Biopsie Zoom und Chromoendoskopie
Seattle Protokoll vs. Färben, NBI, FICE DNA-Aneupleudy, p53

45
Endoskopie Ueberwachung
Barrett ohne Dysplasie: 3 bis 5 Jahre Barrett mit LGD: alle 6 bis 12 Monate Barrett mit HGD: Endoskopische Therapie St.J.Spechler N Engl J Med 2014;371:836-45

46
Behandlungstrategie Chirurgie Ablation Mukosektomie Radio- (RFA)
chemotherapie LGD HGD Frühkarzinom Fortgeschrittenes Karzinom

47
Endoskopie Indikationen
Chronische GERD (> 5 Jahre) 1 bis 2x wöchentlich therapiebedürftiger Reflux (Antazida, H2-Blocker, PPI, Milch..etc) Männer > 50.Lebensjahr Nächtlicher Reflux BMI > 30 kg/m2, viszerale Adipositas Rauchen
 1 bis 2x wöchentlich therapiebedürftiger Reflux (Antazida, H2-Blocker, PPI, Milch..etc) Männer > 50.Lebensjahr. Nächtlicher Reflux. BMI > 30 kg/m2, viszerale Adipositas. Rauchen.")
48
Endoskopie Indikationen
GERD mit persistierenden Beschwerden unter PPI-Therapie oder rasches Rezidiv nach Absetzten Schwere erosive Refluxösopphagitis nach 2 Montaten PPI-Therapie zum Barrett Ausschluss

49
Endoskopie Indikation
Chronischer Reflux Dysphagie Blutung, Anämie Rezidivierendes Erbrechen Upper Endoscopy for Gastrenteroeseophageal Reflux Disease: Best PracticeAdvice From the Clinical Guidelines Commitee of the AmericanCollege of Physicans Ann Intern Med. 2012;157(11):
:")
50
FAZIT Reflux ist nicht harmlos Kein allgemeines Barrett Screening
Index Endoskopie der Risikogruppen NERD oder ERD, Barrett ? Barrett Surveillance 2- bis 5-jährlich

Ähnliche Präsentationen












 kann einerseits als akute Attacke im Sinne eines Einzelereignisses.>")






