Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Was gab es Neues bei der AHA
zur Herzinsuffizienz? Der Konsiliararzt Der Kardiologe Der Internist Der Allgemeinarzt

3
The Cardiac Arrhythmia Suppression Trial
n = 1498, VES after MI, Encainide, flecainide, moricizine Die Rhythmusstörungen verschwanden, aber… “There was an excess of deaths due to arrhythmia and deaths due to shock after acute recurrent MI in patients treated with encainide or flecainide.“ Echt et al., NEJM 1991; 324: 781

4
„Der Kardiologe als Consiliarius“
1. Impact of transfusion on postoperative MI or death (FOCUS TRIAL) Blutkonserven bei Hb < 10 oder bei Symptomen 2016 Pat. nach TEP, 82 Jahre Ergebnis: kein Unterschied (Tod, MI, Angina) bis auf mehr Schlaganfälle und mehr TVT
 Blutkonserven bei Hb < 10 oder bei Symptomen Pat. nach TEP, 82 Jahre. Ergebnis: kein Unterschied (Tod, MI, Angina) bis auf. mehr Schlaganfälle und mehr TVT.")
5
„Chirurgische Studien“
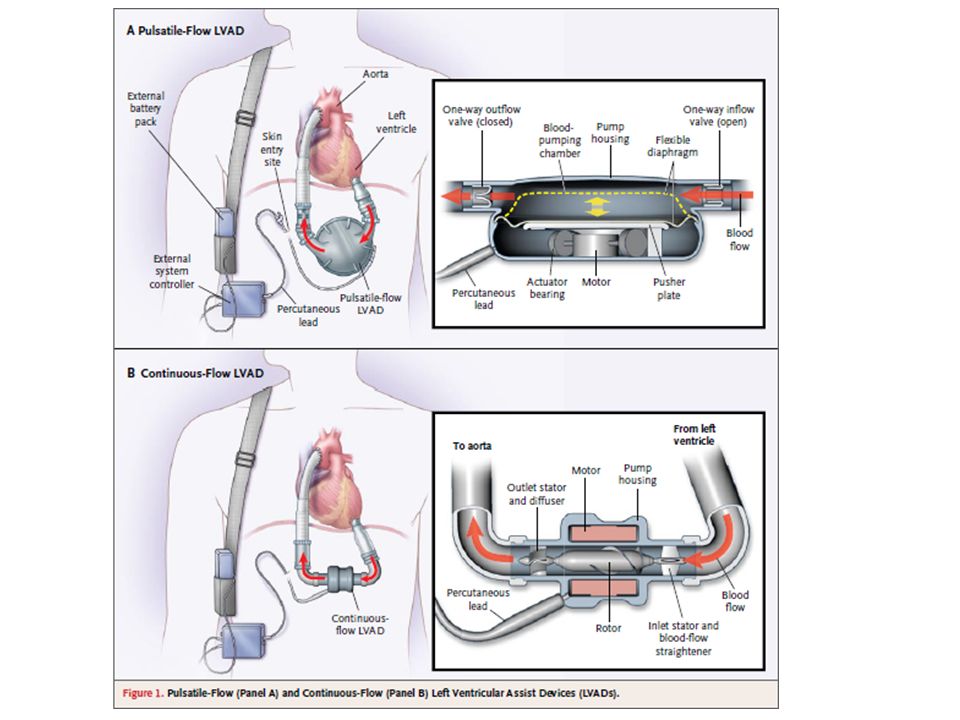
2. Outcomes of patients with advanced HF treated with either a pulsatile or continous flow LVAD (HEARTMATE II Destination Therapy Trial) Ergebnis: Countinous flow device sehr viel besser, (nach 2 Jahren leben noch 58 vs. 24 %)
 Ergebnis: Countinous flow device sehr viel besser, (nach 2 Jahren leben noch 58 vs. 24 %)")
7
Advanced Heart Failure Treated with Continuous-Flow Left Ventricular Assist Device

8
Vergleich der REMATCH- und der aktuellen Studie
1. Rose et al., N Engl J Med 2001;345:

9
„Chirurgische Studien“
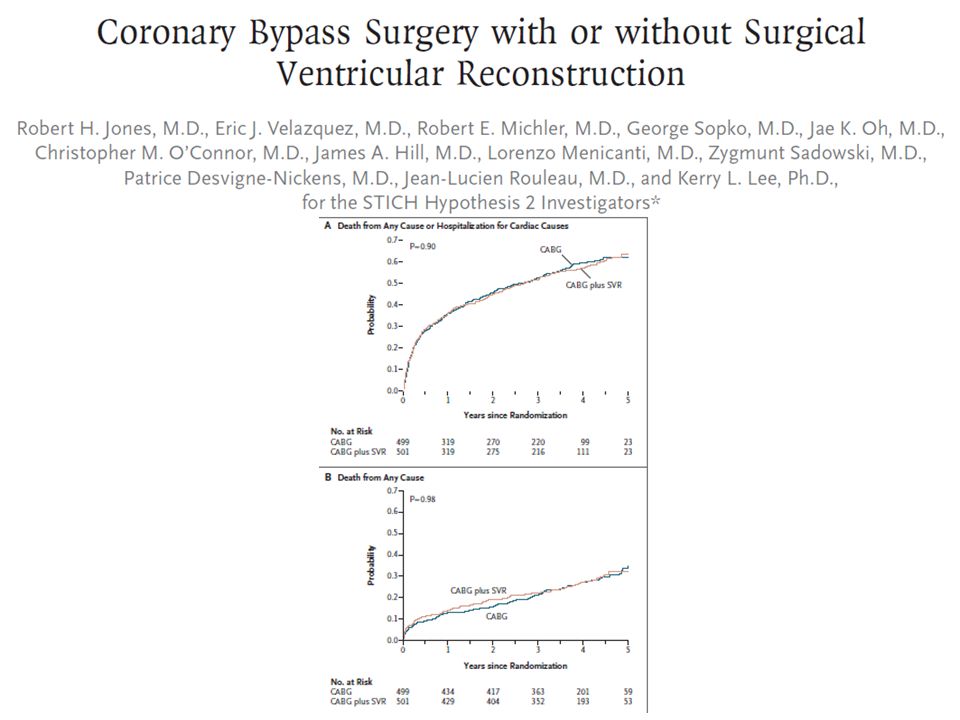
3. Influence of baseline global and regional cardiac function on outcome of patients randomised to CABG with or without surgical ventricular reconstruction Ergebnis: kein Unterschied, auch nicht in irgendeiner Subgruppe

11
„Kardiologische Studien“
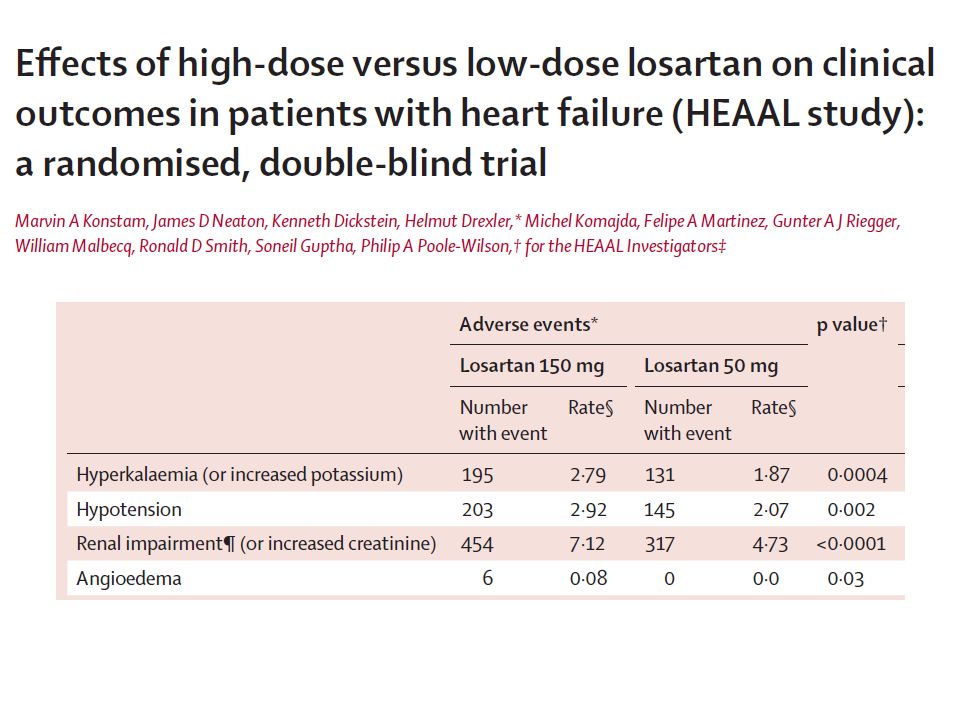
4. Comparison of low-dose versus high-dose Losartan treatment on morbidity and mortality in ACE-I-intolerant patients with heart failure and reduced LVEF (<40%)(HEAAL-Study) 50/150 mg, Ergebnis: bessere Wirkung aber auch mehr NW: Renal impairment (n=454 vs 317), hypotension (203 vs 145), and hyperkalaemia (195 vs 131)
(HEAAL-Study) 50/150 mg, Ergebnis: bessere Wirkung aber auch mehr NW: Renal impairment (n=454 vs 317), hypotension (203 vs 145), and hyperkalaemia (195 vs 131)")
12
www. the lancet. com Published online November 17, 2009 DOI:10
lancet.com Published online November 17, 2009 DOI: /S (09)
")
13
Eff ects of high-dose versus low-dose losartan on clinical outcomes in patients with heart failure (HEAAL study): a randomised, double-blind trial Death or admission for HF

15
„Medikamenten-Studien“
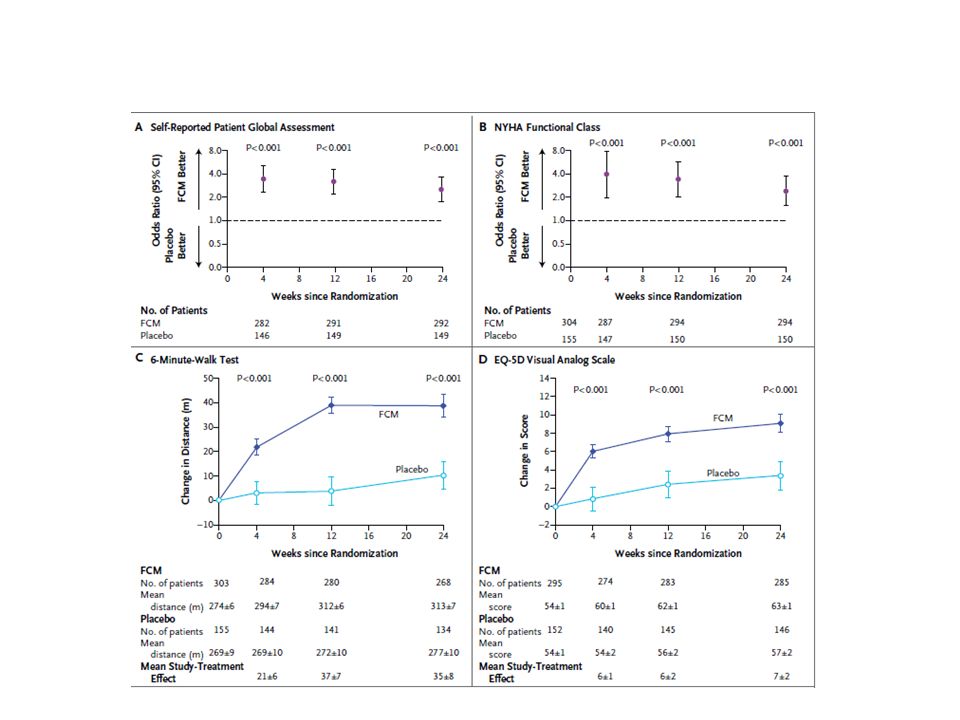
5. Ferric carboxymaltose assessment in patients with iron deficiency and chronic HF with and without anemia (FAIR-HF) Ergebnis: Sowohl bei Pat. mit als auch ohne Anaemie deutliche Besserung des Befindens
 Ergebnis: Sowohl bei Pat. mit als auch ohne Anaemie. deutliche Besserung des Befindens.")
16
N = 459, 67 years, MI 57 %, NYHA III, EF < 40%, (ferritin level <100 μg per liter or between 100 and 299 μg per liter, if the transferrin saturation was <20%), and a hemoglobin level of 9.5 to 13.5 g per 100 ml, Results were similar in patients with anemia and those without anemia!

18
A Trial of Darbepoetin Alfa in Type 2 Diabetes and Chronic Kidney Disease
Hemoglobin Levels among Patients With Darbepoetin Alfa or Placebo. Age: 68 A1c: 7,0, Crea: 1,8 HF : 33% KHK: 44% MI : 18% Pfeffer M et al. N Engl J Med 2009;361:

19
Kaplan-Meier Estimates of the Probability of the Primary and Secondary End Points
Pfeffer M et al. N Engl J Med 2009;361: Figure 2. Kaplan-Meier Estimates of the Probability of the Primary and Secondary End Points. Panel A shows the primary cardiovascular composite end point. The secondary end points of deaths from any cause (Panel B), fatal or nonfatal congestive heart failure (Panel C), fatal or nonfatal myocardial infarction and myocardial ischemia (Panel D), and fatal or nonfatal stroke (Panel E) are also shown. P values are not adjusted for multiple comparison. Adverse events: stroke: 101 vs.53, death: 412 vs.395, VTE: 41 vs. 23, ATE: 178 vs 144
, fatal or nonfatal congestive heart failure (Panel C), fatal or nonfatal myocardial infarction and myocardial ischemia (Panel D), and fatal or nonfatal stroke (Panel E) are also shown. P values are not adjusted for multiple comparison. Adverse events: stroke: 101 vs.53, death: 412 vs.395, VTE: 41 vs. 23, ATE: 178 vs 144.")
20
77 years, NYHA III, EF 30%, Crea 1,33, BNP ~4000
Conclusion: Heart failure therapy guided by N-terminal BNP did not improve overall clinical outcomes or quality of life compared with symptom-guided treatment. Pfisterer et al., JAMA. 2009;301:

21
Zusammenfassung pathophysiologisches Denken in der Medizin kann allenfalls dazu dienen, neue Hypothesen zu formulieren Die Bedeutung einer Klinischen Studie kann nicht überschätzt werden Wir müssen outcome-Studien fordern, bevor wir Therapieprinzipien ändern/akzeptieren Surrogatparameter können uns fehlleiten!

Ähnliche Präsentationen










 bei Herzinsuffizienz>")


 For heavens.>")


>")



