Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
ATHEROSCLEROSE ARTERIOSCLEROSE
Professor LAJOS SZOLLÁR INSTITUT für PATHOPHYSIOLOGIE Fakultät für Medizin SEMMELWEIS Universität 2006

2
Definition Arteriosklerose – Verdickung und Verhärtung der Intima und Media Atherosklerose – intimale Anhäufung von Lipiden Fettablagerung, Zellproliferation, reaktíve Entzündung, Bindegewebswucherung, Nekrose, Verkalkung

3
Definition 2. Die Arteriosklerose stellt einen polyätiologischen Krankheitsprozeß dar: Primäre Alterungsprozesse der Arterien und sekundäre, die Gefäßwand tangierende, metabolische Anomalien überlagern sich in ihren Auswirkungen. Die Atherosklerose ist eine variable Kombination von Veränderungen der Intima, bestehend aus herdförmige Amsammlungen von Lipiden, komplexen Kohlenhydraten, Blut und Blutbestandteilen, Bindegewebe und Kalziumablagerungen. (WHO)
")
4
Entwicklung der Atherosklerose
Gesunde Arterie Frühe Läsion –Fettstreifen – unter 10 Jahres Fortgeschrittene Läsion – fibröser Plaque –ab 20 Jahres Komplizierte Läsion – ab 30 Jahres

5
The progression of atherosclerosis

7
CVD Deaths in the US, by Type
This slide displays the percentages of CVD-related deaths by CVD type in the US in CAD and stroke lead by a very wide margin, with CAD accounting for 54% of all CVD deaths, more than all other types combined. Stroke was the cause of 18% of all CVD deaths. CHF and high blood pressure (BP) resulted in 6% and 5% of all CVD deaths, respectively. Deaths due to other CVD types totaled 18%. American Heart Association. Heart Disease and Stroke Statistics – 2004 Update. Dallas, Tex: American Heart Association; 2003.
 resulted in 6% and 5% of all CVD deaths, respectively. Deaths due to other CVD types totaled 18%. American Heart Association. Heart Disease and Stroke Statistics – 2004 Update. Dallas, Tex: American Heart Association;")
8
Mortality from CVD and CHD in Mortality from CVD and CHD in
Selected Countries Selected Countries Mortality rate per 100,000 population (men aged 35 - 74 years) 1000 CVD deaths CHD deaths 500 Atherosclerosis eventually leads to cardiovascular disease (CVD), resulting in a variety of clinical manifestations including; coronary heart disease (CHD) (angina pectoris, MI, and sudden cardiac death), cerebrovascular disease (transient ischaemic attacks [TIA] and stroke) and peripheral vascular disease (PVD) (intermittent claudication and gangrene). The most significant clinical manifestation, in terms of morbidity and mortality, is CHD. This slide shows that the death rates in selected countries resulting from CVD and CHD vary greatly in different countries, with the highest rates in Eastern Europe and the lowest in Japan.1 CVD is the leading cause of death in Europe, accounting for over 4 million deaths a year.2 Nearly half (49%) of all deaths are from CVD (55% of deaths in women and 43% of deaths in men). References 1. International Cardiovascular Disease Statistics 2003; American Heart Association. 2. European Cardiovascular Disease Statistics 2000 Edition, British Heart Foundation. USA Poland Japan Romania Scotland Germany Sweden Australia Netherlands International Cardiovascular Disease Statistics 2003: AHA
 CVD deaths. CHD deaths Atherosclerosis eventually leads to cardiovascular disease (CVD), resulting in a variety of clinical manifestations including; coronary heart disease (CHD) (angina pectoris, MI, and sudden cardiac death), cerebrovascular disease (transient ischaemic attacks [TIA] and stroke) and peripheral vascular disease (PVD) (intermittent claudication and gangrene). The most significant clinical manifestation, in terms of morbidity and mortality, is CHD. This slide shows that the death rates in selected countries resulting from CVD and CHD vary greatly in different countries, with the highest rates in Eastern Europe and the lowest in Japan.1. CVD is the leading cause of death in Europe, accounting for over 4 million deaths a year.2 Nearly half (49%) of all deaths are from CVD (55% of deaths in women and 43% of deaths in men). References. 1. International Cardiovascular Disease Statistics 2003; American Heart Association. 2. European Cardiovascular Disease Statistics 2000 Edition, British Heart Foundation. USA. Poland. Japan. Romania. Scotland. Germany. Sweden. Australia. Netherlands. International Cardiovascular Disease Statistics 2003: AHA.")
9
Organmanifestationen
Koronarkrankheiten: Angina pectoris, Myokardinfarkt, plötzlicher Herztod Apoplexie, Schlaganfall Claudicatio intermitttens, Gangrän Aneurysma

10
Clinical Manifestations of Atherosclerosis
Coronary heart disease Angina pectoris, myocardial infarction, sudden cardiac death Cerebrovascular disease Transient ischaemic attacks, stroke Peripheral vascular disease Intermittent claudication, gangrene Coronary heart disease Restriction of blood flow to the myocardium may be caused by an atherosclerotic plaque narrowing the lumen of the coronary arteries. If the diameter of the coronary artery is reduced by more than 50%, ischaemia will develop and the patient will experience tightness or crushing pain in the chest (angina pectoris). However, pain does not always accompany myocardial ischaemia: this is called silent ischaemia. Coronary plaque rupture and erosion have been shown to result in thrombus formation within coronary arteries. If blood flow is completely obstructed, either due to a thrombus or by a large atherosclerotic plaque, death to part of the myocardium may ensue, resulting in an MI. Depending on the magnitude or site of the damage to the myocardium the pumping action of the heart may be impaired and/or the heart rate and rhythm may become disturbed. These can result in congestive heart failure or, if very severe, sudden cardiac death.1 Cerebrovascular disease Narrowing of the carotid, vertebral and cerebral arteries supplying blood to the brain can cause a brief interruption in the blood supply to the brain resulting in a transient ischaemic attack. This may cause temporary impairment of vision, speech, sensation or movement and may be followed by a stroke. A stroke may also be caused by formation of a thrombus or embolus, arterial rupture or haemorrhage of the cerebral arteries stopping the oxygen supply to parts of the brain. Sudden loss of consciousness often occurs with subsequent paralysis of parts of the body. It can lead to permanent damage and disability and sudden death.1 Peripheral vascular disease When the lumen of arteries such as the femoral and iliac arteries supplying blood to the legs has been significantly narrowed, by 60% or more, the symptoms of intermittent claudication become evident. These include an aching or cramping pain, most often in the legs when walking, which occurs when insufficient oxygen is reaching the muscles in the legs. In advanced cases of peripheral vascular disease, blood supply to the legs may become completely blocked, possibly by thrombus formation, and painful leg and foot ulcers may develop. If left untreated gangrene may eventually ensue, requiring amputation of the affected limb.1 Reference 1. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000,
. However, pain does not always accompany myocardial ischaemia: this is called silent ischaemia. Coronary plaque rupture and erosion have been shown to result in thrombus formation within coronary arteries. If blood flow is completely obstructed, either due to a thrombus or by a large atherosclerotic plaque, death to part of the myocardium may ensue, resulting in an MI. Depending on the magnitude or site of the damage to the myocardium the pumping action of the heart may be impaired and/or the heart rate and rhythm may become disturbed. These can result in congestive heart failure or, if very severe, sudden cardiac death.1. Cerebrovascular disease Narrowing of the carotid, vertebral and cerebral arteries supplying blood to the brain can cause a brief interruption in the blood supply to the brain resulting in a transient ischaemic attack. This may cause temporary impairment of vision, speech, sensation or movement and may be followed by a stroke. A stroke may also be caused by formation of a thrombus or embolus, arterial rupture or haemorrhage of the cerebral arteries stopping the oxygen supply to parts of the brain. Sudden loss of consciousness often occurs with subsequent paralysis of parts of the body. It can lead to permanent damage and disability and sudden death.1. Peripheral vascular disease When the lumen of arteries such as the femoral and iliac arteries supplying blood to the legs has been significantly narrowed, by 60% or more, the symptoms of intermittent claudication become evident. These include an aching or cramping pain, most often in the legs when walking, which occurs when insufficient oxygen is reaching the muscles in the legs. In advanced cases of peripheral vascular disease, blood supply to the legs may become completely blocked, possibly by thrombus formation, and painful leg and foot ulcers may develop. If left untreated gangrene may eventually ensue, requiring amputation of the affected limb.1. Reference. 1. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000,")
11
Coronary artery disease
Coronary artery disease. Coronary arteriogram showing critical stenosis of left anterior descending coronary artery.

12
Cerebrovascular disease
Cerebrovascular disease. Carotid angiogram showing atherosclerotic narowing of internal carotid artery.

13
Peripheral vascular disease
Peripheral vascular disease. Arteriogram of iliofemoral (left) and femoral (right) arteries showing irregular narrowing due to atherosclerotic disease
 and femoral (right) arteries showing irregular narrowing due to atherosclerotic disease.")
14
Histological section of artery showing atherosclerotic narrowing of lumen

15
The Anatomy of Atherosclerotic Plaque
Intima Lipid core Fibrous cap Lumen Media – T lymphocyte – Macrophage foam cell (tissue factor+) – “Activated” intimal SMC (HLA-DR+) – Normal medial SMC Libby P. Lancet. 1996;348:S4-S7.
 – Activated intimal SMC (HLA-DR+) – Normal medial SMC. Libby P. Lancet. 1996;348:S4-S7.")
16
Macrophages in atheroma

17
Historical Model of Atherogenesis
healthy subclinical symptomatic Threshold Decades Years-Months Months-Days Plaque Intima Media Lumen Stable angina Stable plaques with narrowing Simple diagnostic (ECG, angiography) Rare MI Easy to treat Antischkow N. Beitr Path Anat Allg Path 1913;56: Originally it was thought that atherogenesis was a relatively simple process and revolved around the formation of atheromatous plaques within the intimal wall leading to eventual blockage of the artery. The gradual increase in size of the plaque was thought to encroach into the lumen of the artery, eventually causing a reduction in lumen size. The resulting reduction in blood flow was then thought to cause stable angina pectoris and rarely, myocardial infarction.1 Reference 1. Antischkow N. Beitr Path Anat Allg Path 1913;56:
 Rare MI. Easy to treat. Antischkow N. Beitr Path Anat Allg Path 1913;56: Originally it was thought that atherogenesis was a relatively simple process and revolved around the formation of atheromatous plaques within the intimal wall leading to eventual blockage of the artery. The gradual increase in size of the plaque was thought to encroach into the lumen of the artery, eventually causing a reduction in lumen size. The resulting reduction in blood flow was then thought to cause stable angina pectoris and rarely, myocardial infarction.1. Reference. 1. Antischkow N. Beitr Path Anat Allg Path 1913;56:")
24
New Paradigm healthy subclinical symptomatic Threshold Decades
Years-Months Months-Days Intima Media Plaque Thrombus Lumen Unstable angina Unstable plaque no narrowing Difficult to diagnose (IVUS, MRI) Frequent MI with sudden death Easy to prevent More recently, atherogenesis has been revealed as a complex process and is preceded and accompanied by inflammation. The endothelium responds to damage by inducing a protective response, eventually leading to the formation the atherosclerotic plaque. Over time, the plaque may grow or reduce in size, and may or may not encroach into the lumen of the artery. The clinical outcome often depends on the stability of the plaque.1 The less stable the plaque the more susceptible it is to erosion or rupture. Both erosion and rupture can lead to thrombus formation on the site of the plaque and vessel occlusion, culminating in unstable angina or myocardial infarction.1 Treatment with statins, in addition to dietary and lifestyle changes, may result in regression of atherosclerotic plaques. Reference 1. Ross R. Nature 1993:362:
 Frequent MI with sudden death. Easy to prevent. More recently, atherogenesis has been revealed as a complex process and is preceded and accompanied by inflammation. The endothelium responds to damage by inducing a protective response, eventually leading to the formation the atherosclerotic plaque. Over time, the plaque may grow or reduce in size, and may or may not encroach into the lumen of the artery. The clinical outcome often depends on the stability of the plaque.1 The less stable the plaque the more susceptible it is to erosion or rupture. Both erosion and rupture can lead to thrombus formation on the site of the plaque and vessel occlusion, culminating in unstable angina or myocardial infarction.1 Treatment with statins, in addition to dietary and lifestyle changes, may result in regression of atherosclerotic plaques. Reference. 1. Ross R. Nature 1993:362:")
25
Nonobstructive atheromatous plaque in a coronary artery

26
Unstable and stable plaques

27
IS THE PLAQUE INFLAMED? stable plaque Ustable plaque
Angiography is not capable of differentiating between a stable lesion with little inflammation and a dense fibrous cap and a potentially unstable lesion with numerous inflammatory cells (in red) and a thin fibrous cap. Also, angiography often misses atherosclerotic lesions in remodelled vessels. KW: plaque, inflammation, unstable, angiography
 and a thin fibrous cap. Also, angiography often misses atherosclerotic lesions in remodelled vessels. KW: plaque, inflammation, unstable, angiography.")
28
The Vulnerable Atherosclerotic Plaque
Vulnerable plaques are characterised by a thin fibrous caps, a core rich in lipid and macrophages, and less evidence of smooth muscle proliferation. In contrast, the stable plaque has a relatively thick fibrous cap protecting the lipid core from the contact with blood. Vulnerable plaques are prone to rupture and ulceration, followed by rapid development of thrombi. The size of the plaque does not appear to predict whether a plaque is prone to rupture, indeed clinical data suggest that stable plaques more often show luminal narrowing detectable by angiography than do vulnerable plaques. Rupture usually occurs at sites of thinning (particularly at the shoulder area of the plaque) and is associated with regions where there are relatively few smooth muscle cells but abundant macrophages and T cells. Rupture is associated with greater influx and activation of macrophages, accompanied by release of matrix metalloproteinases that are involved with the breakdown of collagen.1 Reference 1. Libby P. Circulation 1995;91: Libby P. Circulation 1995;91:
 and is associated with regions where there are relatively few smooth muscle cells but abundant macrophages and T cells. Rupture is associated with greater influx and activation of macrophages, accompanied by release of matrix metalloproteinases that are involved with the breakdown of collagen.1. Reference. 1. Libby P. Circulation 1995;91: Libby P. Circulation 1995;91:")
29
Atherosclerosis: A Progressive Process
Normal Fatty Streak Fibrous Plaque Occlusive Atherosclerotic Plaque Plaque Rupture/ Fissure & Thrombosis MI Stroke Critical Leg Ischemia Clinically Silent Coronary Death Increasing Age Effort Angina Claudication Unstable Angina

30
Vulnerable plaque: from plaque to thrombus

31
Total occlusion: plaque + thrombosis

32
The Matrix Skeleton of Unstable Coronary Artery Plaque
Fissures in the fibrous cap Davies MJ. Circulation. 1996;94:

33
AN INFLAMMATORY DISEASE. Almost by definition…from the very beginning
ATHEROSCLEROSIS IS: AN INFLAMMATORY DISEASE. Almost by definition…from the very beginning it is associated with recruitment of monocytes and T-lymphocytes into the sites of developing lesions A LIPID DISORDER DUE TO DYSLIPIDEMIA. Established beyond a reasonable doubt by animal model studies, epidemiologic studies and, ultimately by clinical trials, notably with the statins. KW: inflammation, dyslipidemia

34
Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide
Lipidhypothese Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide Tierexperimentelle Evidenzen Epidemiologische Untersuchungen Geographische Differenzen Migration Interventionen Cholesterin und Ernährung

35
Sudan-stained LDLR -/-
mouse aorta and corresponding autoradiograph of antibodies to epitopes of ox-LDL. Shaw et al., Art Scler Thromb Vasc Biol 21:1333, 2001

36
Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide
Lipidhypothese Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide Tierexperimentelle Evidenzen Epidemiologische Untersuchungen Geographische Differenzen Migration Interventionen Cholesterin und Ernährung

38
The Framingham Study: Relationship Between Cholesterol and CHD Risk
150 125 100 CHD incidence per 1000 75 50 25 Cardiovascular disease is associated with increased levels of total cholesterol.1 Other risk factors include an increase in total to HDL-C ratio, hypertension, cigarette smoking, excess weight, elevated blood sugar levels, lack of exercise, stress, and electrocardiographic abnormalities. Intervention trials have shown that identifying and lowering these risk factors may help to reduce the subsequent rate of coronary heart disease, stroke, and other cardiovascular disease. Reference 1. Castelli WP. Am J Med. 1984;76:4-12. <204 (<5.3) ( ) ( ) ( ) >295 (>7.6) Serum total cholesterol, mg/dL (mmol/L) Castelli WP. Am J Med. 1984;76:4-12
 ( ) ( ) ( ) >295. (>7.6) Serum total cholesterol, mg/dL (mmol/L) Castelli WP. Am J Med. 1984;76:4-12.")
40
Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide
Lipidhypothese Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide Tierexperimentelle Evidenzen Epidemiologische Untersuchungen Geographische Differenzen Migration Interventionen Cholesterin und Ernährung

42
Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide
Lipidhypothese Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide Tierexperimentelle Evidenzen Epidemiologische Untersuchungen Geographische Differenzen Migration Interventionen Cholesterin und Ernährung

44
Cholesterol: A Modifiable Risk Factor
In the USA, 51% (105 million) have elevated total cholesterol (>200 mg/dL, 5.2 mmol/L)1 In EUROASPIRE II, 58% of patients with established CHD had elevated total cholesterol (5 mmol/L, 190 mg/dL)2 10% reduction in total cholesterol results in: 15% reduction in CHD mortality (p<0.001) 11% reduction in total mortality (p<0.001)3 LDL-C is the primary target to prevent CHD It has been estimated that in the USA approximately 105 million people have elevated total cholesterol levels of >200 mg/dL (5.2 mmol/L) and 37 million levels of >240 mg/dL (6.2 mmol/L).1 In EUROASPIRE II, 58% (n=5556) of patients with established CHD were found to have elevated cholesterol levels (5 mmol/L, 190 mg/dL).2 Early trials have shown that a reduction in total cholesterol results in a reduction in the incidence of CHD events. In addition, a meta-analysis of 38 trials3 has shown that for every 10% reduction in total cholesterol, CHD mortality is reduced by 15%, and total mortality by 11% (both p<0.001). Similar reductions were seen with all lipid-modifying treatments studied. Thus, total cholesterol is a modifiable risk factor for CHD and total mortality.4 Low-density lipoprotein (LDL) cholesterol has been recognised as a prime target for lipid intervention to prevent CHD. Under NCEP ATP III LDL-C guidelines it has been estimated that approximately 36 million patients would be suitable for drug therapy.5 The intensity of intervention depends not only on raised cholesterol or LDL-C but also on the presence of a number of other risk factors for CHD. References 1. American Heart Association. Heart and Stroke Statistical Update; 2004. 2. EUROASPIRE II Study Group. Eur Heart J 2001;22: 3. Gould AL et al. Circulation 1998;97:946–952. 4. National Cholesterol Education Program. Circulation 1994;98(3):1333–1445. 5. Fedder DO, Koro CE, L’Italien GJ. Circulation 2002;105: 1. American Heart Association. Heart and Stroke Statistical Update; 2002; 2. EUROASPIRE II Study Group. Eur Heart J 2001;22: ; 3. Gould AL et al. Circulation 1998;97:946–952.
 have elevated total cholesterol (>200 mg/dL, 5.2 mmol/L)1. In EUROASPIRE II, 58% of patients with established CHD had elevated total cholesterol (5 mmol/L, 190 mg/dL)2. 10% reduction in total cholesterol results in: 15% reduction in CHD mortality (p<0.001) 11% reduction in total mortality (p<0.001)3. LDL-C is the primary target to prevent CHD. It has been estimated that in the USA approximately 105 million people have elevated total cholesterol levels of >200 mg/dL (5.2 mmol/L) and 37 million levels of >240 mg/dL (6.2 mmol/L).1 In EUROASPIRE II, 58% (n=5556) of patients with established CHD were found to have elevated cholesterol levels (5 mmol/L, 190 mg/dL).2. Early trials have shown that a reduction in total cholesterol results in a reduction in the incidence of CHD events. In addition, a meta-analysis of 38 trials3 has shown that for every 10% reduction in total cholesterol, CHD mortality is reduced by 15%, and total mortality by 11% (both p<0.001). Similar reductions were seen with all lipid-modifying treatments studied. Thus, total cholesterol is a modifiable risk factor for CHD and total mortality.4. Low-density lipoprotein (LDL) cholesterol has been recognised as a prime target for lipid intervention to prevent CHD. Under NCEP ATP III LDL-C guidelines it has been estimated that approximately 36 million patients would be suitable for drug therapy.5 The intensity of intervention depends not only on raised cholesterol or LDL-C but also on the presence of a number of other risk factors for CHD. References. 1. American Heart Association. Heart and Stroke Statistical Update; EUROASPIRE II Study Group. Eur Heart J 2001;22: Gould AL et al. Circulation 1998;97:946– National Cholesterol Education Program. Circulation 1994;98(3):1333– Fedder DO, Koro CE, L’Italien GJ. Circulation 2002;105: American Heart Association. Heart and Stroke Statistical Update; 2002; 2. EUROASPIRE II Study Group. Eur Heart J 2001;22: ; 3. Gould AL et al. Circulation 1998;97:946–952.")
45
Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide
Lipidhypothese Cholesterin Ablagerungen an den Arterien Cholesterin und Blutlipide Tierexperimentelle Evidenzen Epidemiologische Untersuchungen Geographische Differenzen Migration Interventionen Cholesterin und Ernährung

47
OEK Népegészségügyi Gyorsjelentés, 2002
WHO 2000 OEK Népegészségügyi Gyorsjelentés, 2002

48
Deaths due to CHD shows a significant correlation with average daily cholesterol intake

49
Correlation between the proportion of saturated fatty acid in the diet and MI as well as deaths due to CHD

50
Decline of age-related mortality for cardiovascular and noncardiovascular diseases in the USA from 1968 to 1978

51
Lipid (infiltration) hypothese
 hypothese")
52
Lipid (infiltration) hypothese
Die Anhäufung oder Zufuhr hoher Mengen von Cholesterin und Fetten führt zu Ablagerungen von Lipiden an den Arterien. Extra- und intrazelluläreLipide reichern sich in den Arterienwänden an. Monozyten die sich zu Makrophagen umwandeln nehmen die Lipide auf und werden damit zu sogenannten „schaumzellen”.

53
Lipid (infiltration) hypothese 2.
Zusätzlich wandern aus der Media Muskelzellen in den subendothelialen Raum ein: Sie nehmen ebenfalls Lipide auf. Es kommt zur Intimaproliferation und es resultiert das Atherom.

54
Infiltration of LDL

55
Role of LDL in Atherogenesis

56
„Modified” LDL and atherosclerosis

57
LDL uptake at the „normal” LDL-receptors

58
Macrophages cannot be converted to foam cells by native LDL because uptake is too slow and because, like other cells, the macrophage down regulates its LDL receptors when in the presence of native LDL. Acetylated LDLand certain other chemically conjugated forms of LDL ARE able to generate foam cells but these forms have not been found in vivo. Oxidized LDL, oxidized by incubation with cells or by catalytic concentrations of copper ion, can generate foam cells by interacting with so-called scavenger receptors, including CD36 and SR-A. KW: inflammation, dyslipidemia, macriìophage, modified LDL, CD36, SR-A

59
„Scavenger” receptor LDL-s

60
A model depicting how lipoproteins may contribute to atherosclerosis

61
Wirkungsmechanismen des Risikofaktors „Hyperlipidämie”
Erhöhte Konzentration von LDL können das Endothel schädigen. LDL und hauptsätzlich „modifizierte” LDL können die Proliferation der glatten Muskelzellen in der Media stimulieren. LDL, IDL, VLDL dringen in die Intima durch normales und vor allem durch beschädigtes Endothel ein in den Konzentrationen im Plasma proportionalen Mengen. „Modifizierte” (oxidisierte) LDL-Partikeln werden von proliferierten Muskelzellen bzw. aus dem Blut eingewanderten Monozyten (Makrophagen) via „scavenger” Rezeptoren aufgenommen und abgebaut.
 LDL-Partikeln werden von proliferierten Muskelzellen bzw. aus dem Blut eingewanderten Monozyten (Makrophagen) via „scavenger Rezeptoren aufgenommen und abgebaut.")
62
Wirkungsmechanismen des Risikofaktors „Hyperlipidämie” 2.
Aus abgebauten Lipoproteinen stammendes Cholesterin wirs als Cholesterinester intra- und extrazellulär angereichert. Gleichzeitig werden die glatte Muskelzellen zur vermehrten Bildung von Kollagen, Elastin und Proteoglykanen angeregt und leiten so die Gefäßsklerose ein. Der von Thrombozyten abgegebene Wachstumfaktor erhöht die Ausbildung von LDL-Rezeptoren an den glatten Muskelzellen und dadurch die Aufnahme von LDL. HDL erhöht deb Abtrabsport vin Cholestrein aus der Intima und wirkt der Atherombildung entgegen.

63
„Response to injury”- Modell
Arterielle Hypertonie Veränderte Hämodynamik Lokale Gefäßwandschädigungen Immunologische, chemische oder bakterielle Schädigungen Schwere Hypoxie

64
„Response to injury”- Modell 2.
Die endotheliale Zerstörung oder Fehlfunktion führt zu Adhäsion von Leukozyten und Migration in die Intima. Zusätzlich kommt es vermutlich durch Freisetzung von Kollagen zur Plättenaggregation an den verletzten Arterienwänden. (Thromboxan A2, ADP) Wachstumfaktoren (PDGF) regen die Proliferation glatter Muskelzellen der Media an. Zusätzlich zur Proliferation der Zellen werden Kollagen,Elastin und Proteoglykane synthetisiert. Dies trägt zur Bildung des arteriosklerotischen Plaques bei. Die lumeneinengenden Plaques können ulzerieren, subintimale Einblutungen und weitere Thrombosierungen führen bis zum kompletten Gefäßverschluß.
 Wachstumfaktoren (PDGF) regen die Proliferation glatter Muskelzellen der Media an. Zusätzlich zur Proliferation der Zellen werden Kollagen,Elastin und Proteoglykane synthetisiert. Dies trägt zur Bildung des arteriosklerotischen Plaques bei. Die lumeneinengenden Plaques können ulzerieren, subintimale Einblutungen und weitere Thrombosierungen führen bis zum kompletten Gefäßverschluß.")
65
AN INFLAMMATORY DISEASE. Almost by definition…from the very beginning
ATHEROSCLEROSIS IS: AN INFLAMMATORY DISEASE. Almost by definition…from the very beginning it is associated with recruitment of monocytes and T-lymphocytes into the sites of developing lesions A LIPID DISORDER DUE TO DYSLIPIDEMIA. Established beyond a reasonable doubt by animal model studies, epidemiologic studies and, ultimately by clinical trials, notably with the statins. KW: inflammation, dyslipidemia

66
Atherosclerosis: An Inflammatory Disorder
The earliest atherosclerotic lesion, the fatty streak, is macrophage- and T- lymphocyte rich The endothelium is an active organ that produces as well as responds to inflammatory mediators Cytokines have an impact upon the cellular make-up in plaque lesions Investigation of the inflammatory component of atherosclerosis has increased substantially and has identified potential novel markers for risk assessment, such as C-reactive protein, as well as potential novel targets for intervention, such as LFA-1 inhibition. KW: inflammation, CRP. LFA-1

68
Pathogenesis of Atherosclerotic Plaques
Endothelial damage Protective response results in production of cellular adhesion molecules Monocytes and T lymphocytes attach to ‘sticky’ surface of endothelial cells Migrate through arterial wall to subendothelial space The primary event in atherosclerosis is thought to be damage caused to the endothelium of arterial walls, resulting in endothelial dysfunction. This damage may be caused by a variety of factors; haemodynamic forces (shear stress caused by e.g. hypertension), a number of vasoactive substances, mediators (cytokines) from blood cells, cigarette smoke, atherogenic diet, elevated glucose levels and oxidised LDL-C.1 Initially, damage causes the endothelial cells to express cellular adhesion molecules such as cytokines (interleukin-1, IL-1; tumour necrosis factor alpha, TNF-alpha), chemokines (monocyte chemoattractant factor 1, MCP-1; IL-8) and growth factors (platelet-derived growth factor, PDGF; basic fibroblast growth factor, bFGF).1 This ‘sticky’ surface encourages inflammatory cells such as monocytes and T lymphocytes to attach to the endothelial surface. Once attached they migrate through the intact endothelium into the subendothelial space. Many of the monocytes differentiate into macrophages and take up oxidised LDL, which is more atherogenic than native LDL; these macrophages then become foam cells.1 Oxidised LDL promotes death of endothelial cells and an inflammatory response resulting in impairment of normal function of the endothelium. In addition, it modifies the response to angiotensin II, resulting in vasodilatory impairment, and induces a prothrombic state by affecting platelets and coagulation factors. Thus, the endothelium responds to damage by inducing a protective response which will eventually lead to the formation of fibrofatty and fibrous lesions, the atherosclerotic plaque, preceded and accompanied by inflammation.2 This schematic linear diagram represents part of a network of complex processes that include various disease (and protecting) mechanisms that occur simultaneously. References 1. Koenig W. Eur Heart J Supplements 1999:1:T19–26. 2. Ross R. Nature 1993;362:801–809. Macrophages take up oxidised LDL-C Lipid-rich foam cells Fatty streak and plaque
, a number of vasoactive substances, mediators (cytokines) from blood cells, cigarette smoke, atherogenic diet, elevated glucose levels and oxidised LDL-C.1. Initially, damage causes the endothelial cells to express cellular adhesion molecules such as cytokines (interleukin-1, IL-1; tumour necrosis factor alpha, TNF-alpha), chemokines (monocyte chemoattractant factor 1, MCP-1; IL-8) and growth factors (platelet-derived growth factor, PDGF; basic fibroblast growth factor, bFGF).1 This ‘sticky’ surface encourages inflammatory cells such as monocytes and T lymphocytes to attach to the endothelial surface. Once attached they migrate through the intact endothelium into the subendothelial space. Many of the monocytes differentiate into macrophages and take up oxidised LDL, which is more atherogenic than native LDL; these macrophages then become foam cells.1. Oxidised LDL promotes death of endothelial cells and an inflammatory response resulting in impairment of normal function of the endothelium. In addition, it modifies the response to angiotensin II, resulting in vasodilatory impairment, and induces a prothrombic state by affecting platelets and coagulation factors. Thus, the endothelium responds to damage by inducing a protective response which will eventually lead to the formation of fibrofatty and fibrous lesions, the atherosclerotic plaque, preceded and accompanied by inflammation.2. This schematic linear diagram represents part of a network of complex processes that include various disease (and protecting) mechanisms that occur simultaneously. References. 1. Koenig W. Eur Heart J Supplements 1999:1:T19– Ross R. Nature 1993;362:801–809. Macrophages take up oxidised LDL-C. Lipid-rich foam cells. Fatty streak and plaque.")
69
Role of cytokines in atherothrombosis

70
The ‘Activated’ Endothelium
cytokines (eg. IL-1, TNF-) chemokines (eg.MCP-1, IL-8) growth factors (eg. PDGF, FGF) CELLULAR ADHESION MOLECULES Endothelial injury, or exposure to atherogenic stimuli, triggers endothelial cell inflammatory responses leading to recruitment of leukocytes and release of cellular adhesion molecules; cytokines, including tumour necrosis factor- (TNF-), interleukin-1 (IL-1) and interferon gamma (IFN- ), chemokines, including monocyte chemoattractant factor 1 (MCP-1) and interleukin-8 (IL-8), and growth factors, including platelet derived growth factor (PDGF) and fibroblast growth factor (FGF).1 The cytokines, in addition to amplifying the immune response, alter endothelial cell function towards a prothrombotic state, characterised by increased production of platelet activator inhibitor-1 (PAI-1), tissue factor expression (TFE) and activation of the extrinsic coagulation pathway), and release of PDGF. Reference 1. Koenig W. Eur Heart J Suppl 1999;1(Suppl T);T19-26. attracts monocytes and T lymphocytes which adhere to endothelial cells induces cell proliferation and a prothrombic state Koenig W. Eur Heart J Suppl 1999;1(Suppl T);T19-26.
 chemokines (eg.MCP-1, IL-8) growth factors (eg. PDGF, FGF) CELLULAR ADHESION MOLECULES. Endothelial injury, or exposure to atherogenic stimuli, triggers endothelial cell inflammatory responses leading to recruitment of leukocytes and release of cellular adhesion molecules; cytokines, including tumour necrosis factor- (TNF-), interleukin-1 (IL-1) and interferon gamma (IFN- ), chemokines, including monocyte chemoattractant factor 1 (MCP-1) and interleukin-8 (IL-8), and growth factors, including platelet derived growth factor (PDGF) and fibroblast growth factor (FGF).1. The cytokines, in addition to amplifying the immune response, alter endothelial cell function towards a prothrombotic state, characterised by increased production of platelet activator inhibitor-1 (PAI-1), tissue factor expression (TFE) and activation of the extrinsic coagulation pathway), and release of PDGF. Reference. 1. Koenig W. Eur Heart J Suppl 1999;1(Suppl T);T attracts monocytes and T lymphocytes. which adhere to endothelial cells. induces cell proliferation and a prothrombic state. Koenig W. Eur Heart J Suppl 1999;1(Suppl T);T")
71
The ‘Activated’ Endothelium

72
Endothelial wall and leukocytes in: Athero-sclerosis –Macrophage/www
Endothelial wall and leukocytes in: Athero-sclerosis –Macrophage/

74
NOT EITHER/OR… BUT BOTH: ATHEROGENESIS IN PERSPECTIVE:
HYPERCHOLESTEROLEMIA, AND INFLAMMATION AS PARTNERS IN CRIME. (Steinberg, Nature Med ,2002) KW: inflammation, dyslipidemia
 KW: inflammation, dyslipidemia.")
75
Atherosclerosis is an inflammatory disease
Immune activity in plaque T cells, Mø, Antibodies Local immune activation Cytokines, costimulatory factors Systemic response Antibodies, T cells Circulating CRP, IL-6 Genetic associations Immunostimulatory genes OX40L, MHCIITA Immunopathogenicity Major effects of immune factors in model systems There is today strong evidence for atherosclerosis being an inflammatory disease. The first data was obtained through analysis of human lesions and demonstrated infiltrating T cells, macrophages and antibody deposits. It was also shown that cytokines are produced locally in the plaque; together with costimulatory factors, they may promote inflammation. More recent studies have demonstrated associations to myocardial infarction and stroke for systemic inflammatory responses and immune genes. Finally, gene-targeted mouse models have permitted a dissection of disease pathways. KW: inflammation

77
Risikofaktoren der Arteriosklerose
Beeinflußbar Rauchen Dyslipidaemia Hoch LDL-C Niedrige HDL-C Erhöhte TG Arterielle Hypertonie Diabetes mellitus Adiposität Dietary factors Thrombogene Faktoren Bewegungsmangel Infektionen Alkoholzufuhr Nicht beeinflußbar Genetik (Familien) Alter Geschlecht Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 Alter. Geschlecht. Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1. Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
78
Serum cholesterol level
Levels of Risk Associated with Smoking, Hypertension and Hypercholesterolaemia Hypertension (SBP 195 mmHg) x3 x4.5 x9 x16 x1.6 x4 x6 Smoking Multiple risk factors for CVD are usually present in an individual; rarely do they occur in isolation. When risk factors co-exist the effect is often exponential; their combined effect is greater than the sum of their individual effects.1 Multiple risk factors are also associated with the metabolic syndrome which is characterized by dyslipidaemia, hypertension, insulin resistance, visceral distribution of body fat, and a prothrombotic state.2 References 1. Poulter N. In Cardiovascular Disease: Risk Factors and Intervention. Eds: Poulter N, Sever P, Thom S. Radcliffe Medical Press, Oxford, 1993. 2. Deedwania PC. Am J Med 1998;105(1A);1S-3S. Serum cholesterol level (8.5 mmol/L, 330 mg/dL) Poulter N et al., 1993
 x3. x4.5. x9. x16. x1.6. x4. x6. Smoking. Multiple risk factors for CVD are usually present in an individual; rarely do they occur in isolation. When risk factors co-exist the effect is often exponential; their combined effect is greater than the sum of their individual effects.1. Multiple risk factors are also associated with the metabolic syndrome which is characterized by dyslipidaemia, hypertension, insulin resistance, visceral distribution of body fat, and a prothrombotic state.2. References. 1. Poulter N. In Cardiovascular Disease: Risk Factors and Intervention. Eds: Poulter N, Sever P, Thom S. Radcliffe Medical Press, Oxford, Deedwania PC. Am J Med 1998;105(1A);1S-3S. Serum cholesterol level. (8.5 mmol/L, 330 mg/dL) Poulter N et al.,")
79
Relative Risk of CHD (16-Year)
Framingham Offspring Study Risk Factors Low HDL-C High total cholesterol High BMI High SBP High TG High glucose 6- Relative Risk of CHD (16-Year) 5- 4- 3- Men Women 2- 1- KW: Framingham, CHD, men, women, gender, risk factor 1 2 3 4 1 2 3 4 Number of Risk Factors Wilson 2004
 Men. Women KW: Framingham, CHD, men, women, gender, risk factor Number of Risk Factors. Wilson")
80
PROCAM: Combination of Risk Factors Increases Risk of MI
None The Prospective Cardiovascular Münster Study (PROCAM) showed that rates of myocardial infarction (MI) over a 4-year follow-up period in a group of middle-aged men were increased nearly three times in people with diabetes compared with no diabetes. When diabetes mellitus and hypertension occurred together, the incidence of MI was eight-fold greater than in subjects without any risk factors. If dyslipidaemia was also present, a further two-fold increase in risk was observed. These data confirm both the independent risk associated with diabetes mellitus and the synergistic interaction that diabetes has with other common risk factors for coronary heart disease.1 Reference 1. Assmann G, Schulte H. Am Heart J 1988;116: Hypertens + diabetes Hypertension only Diabetes only Dyslipidaemia Dyslipidaemia + hypertens +/- diabetes Prevalence (%): Assmann G, Schulte H. Am Heart J 1988;116:
 showed that rates of myocardial infarction (MI) over a 4-year follow-up period in a group of middle-aged men were increased nearly three times in people with diabetes compared with no diabetes. When diabetes mellitus and hypertension occurred together, the incidence of MI was eight-fold greater than in subjects without any risk factors. If dyslipidaemia was also present, a further two-fold increase in risk was observed. These data confirm both the independent risk associated with diabetes mellitus and the synergistic interaction that diabetes has with other common risk factors for coronary heart disease.1. Reference. 1. Assmann G, Schulte H. Am Heart J 1988;116: Hypertens + diabetes. Hypertension only. Diabetes only. Dyslipidaemia. Dyslipidaemia + hypertens +/- diabetes. Prevalence (%): Assmann G, Schulte H. Am Heart J 1988;116:")
82
„Classical” risk factors of atherosclerosis

83
Risk Factors for Cardiovascular Disease
Modifiable Smoking Dyslipidaemia Raised LDL-C Low HDL-C Raised triglycerides Raised blood pressure Diabetes mellitus Obesity Dietary factors Thrombogenic factors Lack of exercise Excess alcohol consumption Non-modifiable Personal history of CVD Family history of CVD Age Gender Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
84
Risikofaktoren der Arteriosklerose
Beeinflußbar Rauchen Dyslipidaemia Hoch LDL-C Niedrige HDL-C Erhöhte TG Arterielle Hypertonie Diabetes mellitus Adiposität Dietary factors Thrombogene Faktoren Bewegungsmangel Infektionen Alkoholzufuhr Nicht beeinflußbar Genetik (Familien) Alter Geschlecht Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 Alter. Geschlecht. Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1. Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
85
Cigarette smoking and initial MI in men and women

87
Risk Factors for Cardiovascular Disease
Modifiable Smoking Dyslipidaemia Raised LDL-C Low HDL-C Raised triglycerides Raised blood pressure Diabetes mellitus Obesity Dietary factors Thrombogenic factors Lack of exercise Excess alcohol consumption Non-modifiable Personal history of CVD Family history of CVD Age Gender Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
88
Risikofaktoren der Arteriosklerose
Beeinflußbar Rauchen Dyslipidaemia Hoch LDL-C Niedrige HDL-C Erhöhte TG Arterielle Hypertonie Diabetes mellitus Adiposität Dietary factors Thrombogene Faktoren Bewegungsmangel Infektionen Alkoholzufuhr Nicht beeinflußbar Genetik (Familien) Alter Geschlecht Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 Alter. Geschlecht. Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1. Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
89
Increased risk of recurrent MI, CHD and all-cause mortality according to total cholesterol

92
Cardiovascular Disease
and HDL-C Levels 160 140 Men Women 120 Rate per 1000 100 80 60 40 KW: CHD, risk factor, HDL, men, women, gender 20 <34 35-54 >55 <34 35-54 >55 HDL Cholesterol, mg/dL Kannel WB. Am J Cardiol. 1983;52:9B-12B.

93
Hypertriglyceridemia—An Independent Risk Factor for CHD: PROCAM Study
150 132 93 100 81 Events/ 1,000 in 8 yr 44 50 KW: hypertriglyceridemia, CHD, risk factor, PROCAM, TG <200 (157/3,593) (84/903) (14/106) 800 (3/37) TG (mg/dL) Assmann G et al. Am J Cardiol. 1992;70:
 (84/903) (14/106) 800 (3/37) TG (mg/dL) Assmann G et al. Am J Cardiol. 1992;70:")
94
Triglyceride and CHD Risk PROCAM Study
250 TG < 200 mg/dL TG 200 mg/dL 245 200 150 per 1,000 (in 6 years) Incidence 100 116 50 KW: TG, CVD, risk, PROCAM 31 24 5.0 > 5.0 LDL-C/HDL-C ratio Assmann G, Schulte H. Am J Cardiol 1992;70:733–737.
 Incidence KW: TG, CVD, risk, PROCAM 5.0. > 5.0. LDL-C/HDL-C ratio. Assmann G, Schulte H. Am J Cardiol 1992;70:733–737.")
95
Relationship Between Changes in LDL-C and HDL-C Levels and CHD Risk
1% decrease in LDL-C reduces CHD risk by 1% 1% increase in HDL-C reduces CHD risk by 1% KW: risk, LDL, HDL

96
Impact of Lipid Levels on CAD Risk
LDL-C is the primary target for cholesterol management. An abundance of experimental and epidemiologic evidence demonstrates that elevated LDL-C levels increase the likelihood of CAD. Robust evidence from clinical trials also shows that reducing LDL-C levels reduces CAD risk. In the Framingham Study and subsequent studies, low levels of HDL-C have also been recognized as a significant risk factor for CAD. HDL-C levels <40 mg/dL are associated with increased risk for CAD. For persons with observed HDL-C levels <40mg/dL coupled with a TC ?200mg/dL, a follow-up lipoprotein profile is recommended. It has been estimated that a 10% population-wide decrease in TC levels could reduce the incidence of CAD by 30%. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106: American Heart Association. Heart Disease and Stroke Statistics – 2004 Update. Dallas, Tex: American Heart Association; 2003.
 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106: American Heart Association. Heart Disease and Stroke Statistics – 2004 Update. Dallas, Tex: American Heart Association;")
97
Risikofaktoren der Arteriosklerose
Beeinflußbar Rauchen Dyslipidaemia Hoch LDL-C Niedrige HDL-C Erhöhte TG Arterielle Hypertonie Diabetes mellitus Adiposität Dietary factors Thrombogene Faktoren Bewegungsmangel Infektionen Alkoholzufuhr Nicht beeinflußbar Genetik (Familien) Alter Geschlecht Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 Alter. Geschlecht. Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1. Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
98
Blood Pressure and CVD: Framingham Heart Study
Men Women Relative Risk of CHD (12-Year) 5- 4- 3- 2- 1- KW: Framingham, CHD, BP, men, women, gender <120 120 -129 130 -139 120 -129 130 -139 <120 Systolic Blood Pressure (mmHg)
 KW: Framingham, CHD, BP, men, women, gender. < <120. Systolic Blood Pressure (mmHg)")
99
Risikofaktoren der Arteriosklerose
Beeinflußbar Rauchen Dyslipidaemia Hoch LDL-C Niedrige HDL-C Erhöhte TG Arterielle Hypertonie Diabetes mellitus Adiposität Dietary factors Thrombogene Faktoren Bewegungsmangel Infektionen Alkoholzufuhr Nicht beeinflußbar Genetik (Familien) Alter Geschlecht Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 Alter. Geschlecht. Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1. Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
102
Combination Risk for CAD: Metabolic Syndrome
The National Cholesterol Educational Program Adult Treatment Panel III (NCEP ATP III) has described metabolic syndrome as a constellation of lipid and nonlipid risk factors that put patients at markedly increased risk for CVD. These abnormalities include abdominal obesity, atherogenic dyslipidemia, increased BP, insulin resistance, proinflammatory state, and prothrombotic state. NCEP ATP III has recognized metabolic syndrome as a secondary target of risk-reduction therapy. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:
 has described metabolic syndrome as a constellation of lipid and nonlipid risk factors that put patients at markedly increased risk for CVD. These abnormalities include abdominal obesity, atherogenic dyslipidemia, increased BP, insulin resistance, proinflammatory state, and prothrombotic state. NCEP ATP III has recognized metabolic syndrome as a secondary target of risk-reduction therapy. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:")
103
Factors altering the course of cardiovascular disease

104
Proinflammatory State
Adipose Tissue Liver Cytokines Unstable Plaques CRP KW: inflammation, cytokine, adipocyte, liver, CRP Apo B Diabetes HDL Prothrombotic State

105
CRP and CHD risk

106
CRP and CHD risk

107
Reassignment of risk strata
Lp(a) >40 mg/dL CRP > 5 mg/L ESR > 10 mm/h fibrinogen > 3.85 g/L apo B > 1.2 g/L genotyping: APOE, F5 carotid doppler: IMT Additional biochemical and genetic factors that could result in re-assignment of a patient to a different risk stratum that that which would be predicted by the traditional risk factors, such as the Framingham risk factors. KW: risk factor
 >40 mg/dL. CRP > 5 mg/L. ESR > 10 mm/h. fibrinogen > 3.85 g/L. apo B > 1.2 g/L. genotyping: APOE, F5. carotid doppler: IMT. Additional biochemical and genetic factors that could result in re-assignment of a patient to a different risk stratum that that which would be predicted by the traditional risk factors, such as the Framingham risk factors. KW: risk factor.")
108
Risikofaktoren der Arteriosklerose
Beeinflußbar Rauchen Dyslipidaemia Hoch LDL-C Niedrige HDL-C Erhöhte TG Arterielle Hypertonie Diabetes mellitus Adiposität Dietary factors Thrombogene Faktoren Bewegungsmangel Infektionen Alkoholzufuhr Nicht beeinflußbar Genetik (Familien) Alter Geschlecht Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 Alter. Geschlecht. Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1. Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
109
26 -Year Incidence of CHD in Men
Obesity and CHD: 26 -Year Incidence of CHD in Men <50 years 50+ years 600 500 440 366 400 350 333 300 255 177 Incidence/1,000 200 100 KW: metabolic syndrome, MS, CHD, risk factor, obesity, men, BMI, Framingham <25 25-<30 30+ BMI Level Framingham Heart Study Adapted from Hubert HB et al. Circulation 1983;67: Metropolitan Relative Weight of 110 is a BMI of approximately 25.

111
Risikofaktoren der Arteriosklerose
Beeinflußbar Rauchen Dyslipidaemia Hoch LDL-C Niedrige HDL-C Erhöhte TG Arterielle Hypertonie Diabetes mellitus Adiposität Dietary factors Thrombogene Faktoren Bewegungsmangel Infektionen Alkoholzufuhr Nicht beeinflußbar Genetik (Familien) Alter Geschlecht Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.
 Alter. Geschlecht. Some of the risk factors that predispose an individual to the development or progression of CVD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CVD. Of these, three are considered to be of prime importance:1. Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CVD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CVD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-C. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
112
Physical Inactivity, Fitness, and CVD
2.50 2.25 1.89 2.00 CVD Mortality RR 1.50 1.00 1.00 1.00 0.50 KW: metabolic syndrome, MS, CHD, risk factor, mortality, life style, inactivity 0.00 Healthy Metabolic Syndrome Metabolic Syndrome Fit Metabolic Syndrome Unfit Katzmarzyk (Blair) Arch Interen Med. 2004;164:1029-7
 Arch Interen Med. 2004;164:")
114
Continuum of Patients at Risk for a CHD Event
Post MI/Angina Other Atherosclerotic Manifestations Subclinical Atherosclerosis Multiple Risk Factors Low Risk Secondary Prevention Primary Prevention

115
Principles of Prevention of Cardiovascular Disease
Fundamental Principles Identify risk factors Determine risk category Adjust intensity of treatment . Risk Categories High Risk Intermediate Risk Lower to Moderate Risk KW: guidelines, risk factor

116
Fundamental Principles
Identify major cardiovascular risk factors Determine patient’s cardiovascular risk category Adjust intensity of treatment of risk factors to patient’s risk category KW: guidelines

117
Major Cardiovascular Risk Factors
LDL cholesterol HDL cholesterol Triglycerides Blood pressure Diabetes mellitus Smoking History of CHD or stroke Age: men > 45 years; women > 55 years KW: guidelines, risk factor, LDL, HDL, TG, diabetes, age, gender, blood pressure

118
10-Year Risk Assessment Calculate 10-year risk with risk algorithm
Framingham: PROCAM: Some countries require 10-year risk > 30% to define high risk Some authorities include diabetes in 10-year risk assessment KW: guidelines, risk factor, Framingham, PROCAM, risk algorithm

119
High-Risk Category Established CVD (CAD, PAD, aortic or carotid disease) Diabetes mellitus, particularly in combination with microalbuminuria Multiple risk factors (10-year risk for CHD > 20%) KW: guidelines, risk factor, diabetes
 KW: guidelines, risk factor, diabetes.")
120
Intermediate Risk Category
> 2 risk factors and 10-year risk 10-20% Metabolic syndrome--3 or 5 following: Abdominal obesity (geographic region specific) Fasting TG > 150 mg/dl (1.7 mmol/L) HDL < 40 mg/dl (1.0 mmol/L) men < 50 mg/dl (1.3 mmol/L) women BP > 130/85 mmHg Glucose > 110 mg/dl (6.0 mmol/L) KW: guidelines, risk factor, metabolic syndrome, obesity, HDL, blood pressure, glucose, TG
 Fasting TG > 150 mg/dl (1.7 mmol/L) HDL < 40 mg/dl (1.0 mmol/L) men. < 50 mg/dl (1.3 mmol/L) women. BP > 130/85 mmHg. Glucose > 110 mg/dl (6.0 mmol/L) KW: guidelines, risk factor, metabolic syndrome, obesity, HDL, blood pressure, glucose, TG.")
121
Lower to Moderate Risk Category
Lower risk: 0-1 risk factor Moderate risk: > 2 risk factors 10-year risk: < 10% KW: guidelines, risk factor

122
National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) Clinical Guidelines 2001 The Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults presents the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) recommendations for CAD* risk assessment and treatment. In this presentation, we review these guidelines and recent recommended modifications based on clinical trials, as well as specific risk factors and categories contributing to the assessment of global risk for CAD. *NCEP ATP III defines CAD as symptomatic ischemic heart disease, including myocardial infarction, stable or unstable angina, demonstrated myocardial ischemia by noninvasive testing, and history of coronary artery procedures.
 recommendations for CAD* risk assessment and treatment. In this presentation, we review these guidelines and recent recommended modifications based on clinical trials, as well as specific risk factors and categories contributing to the assessment of global risk for CAD. *NCEP ATP III defines CAD as symptomatic ischemic heart disease, including myocardial infarction, stable or unstable angina, demonstrated myocardial ischemia by noninvasive testing, and history of coronary artery procedures.")
123
NCEP ATP III Guidelines:Global Risk Assessment – 2001
Individual risk factors other than LDL-C that affect CAD risk status in primary prevention - Cigarette smoking - Hypertension (blood pressure >=140/90 mm Hg) - Low high-density lipoprotein cholesterol (HDL-C) (<40 mg/dL)* - Family history of premature CAD –- In males: first-degree relative <55 years –- In females: first-degree relative <65 years - Age (men >=45 years; women >=55 years) *HDL-C >=60 mg/dL counts as a “negative” risk factor; this level of HDL-C removes 1 risk factor from the total. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:
 - Low high-density lipoprotein cholesterol (HDL-C) (<40 mg/dL)* - Family history of premature CAD. –- In males: first-degree relative <55 years. –- In females: first-degree relative <65 years. - Age (men >=45 years; women >=55 years) *HDL-C >=60 mg/dL counts as a negative risk factor; this level of HDL-C removes 1 risk factor from the total. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:")
124
A. Risikoabschätzung zur Auswahl von Patienten für die klinische Behandlung

125
A. Risikoabschätzung zur Auswahl von Patienten für die klinische Behandlung
Eine Mikroalbuminurie ist definiert als Albuminausscheidungsrate im Urin von μg/min in zwei von drei über einen Zeitraum von 6 Monaten gewonnenen Urinproben. Dies entspricht in etwa der Ausscheidung von 30-300mg Albumin über 24 Stunden. Eine andere, wenn auch weniger genaue Nachweismethode der Mikroalbuminurie ist die Bestimmung des Albumins oder des Verhältnisses aus Albumin- und Kreatinin- Ausscheidung im Spontanurin (idealerweise zweiter Morgenurin), wobei eine Albuminausscheidung von mg/L oder von mg/g Kreatinin eine Mikroalbuminurie anzeigt.
, wobei eine Albuminausscheidung von mg/L oder von mg/g Kreatinin eine Mikroalbuminurie anzeigt.")
126
A. Risikoabschätzung zur Auswahl von Patienten für die klinische Behandlung

128
PROCAM Score für einzelne Risikofaktoren
Die Abbildung gibt an, welche Punktzahl jedem einzelnen Risikofaktor zugeordnet wird. Alle angegebenen Parameter müssen bekannt sein! Um die Gesamtzahl zu ermitteln, addieren Sie einfach die Punktzahlen für die einzelnen Risikofaktoren. Dasmit der jeweiligen Gesamtpunktzahl verbundene Risiko können Sie in der folgendenAbbildung ablesen.

130
PROCAM Score Alter (Jahre) 35-39 0 40-44 6 45-49 11 50-54 16 55-59 21
Systolischer Blutdruck (mm Hg) < >= LDL-Cholesterin (mg/dl) < > Triglyzeride (mg/dl) < > HDL-Cholesterin (mg/dl) <35 11 > Raucher Nein Ja Positive Familien- anamnese Nein Ja Diabetiker Nein 0 Ja 6 Assmann, Cullen, Schulte; Circulation, 105: ; 2002
 < >= LDL-Cholesterin (mg/dl) < > Triglyzeride (mg/dl) < > HDL-Cholesterin (mg/dl) < >54 0. Raucher. Nein 0. Ja 8. Positive Familien- anamnese. Nein 0. Ja 4. Diabetiker. Nein 0. Ja 6. Assmann, Cullen, Schulte; Circulation, 105: ;")
131
PROCAM Score Anzahl der Punkte 20 21 22 23 24 25 26 27 28 29 30 31
32 33 34 Herzinfarkt- risiko in 10 Jahren (%) 1.0 1.1 1.2 1.3 1.4 1.6 1.7 1.8 1.9 2.3 2.4 2.8 2.9 3.3 3.5 Anzahl der Punkte 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 Herzinfarkt- risiko in 10 Jahren (%) 4.0 4.2 4.8 5.1 5.7 6.1 7.0 7.4 8.0 8.8 10.2 10.5 10.7 12.8 13.2 Anzahl der Punkte 50 51 52 53 54 55 56 57 58 59 60 Herzinfarkt- risiko in 10 Jahren (%) 15.5 16.8 17.5 19.6 21.7 22.2 23.8 25.1 28.0 29.4 30.0 Assmann, Cullen, Schulte; Circulation, 105: ; 2002
 Anzahl. der Punkte Herzinfarkt- risiko in. 10 Jahren (%) Anzahl. der Punkte 60. Herzinfarkt- risiko in. 10 Jahren (%) Assmann, Cullen, Schulte; Circulation, 105: ;")
132
Der PROCAM Algorithmus
Herzinfarkte (%) in 10 Jahren 21.4 7.6 2.8 2.1 0.6 I II III IV V Quintile des PROCAM Score Unabhängige Parameter: Alter, systolischer Blutdruck, LDL-Cholesterin, HDL-Cholesterin, Triglyzeride, Diabetes mellitus, Rauchen, familiäre Belastung, 325 tödliche und nicht-tödliche Herzinfarkte bei 4818 Männern im Alter von Jahren
 in 10 Jahren I. II. III. IV. V. Quintile des PROCAM Score. Unabhängige Parameter: Alter, systolischer Blutdruck, LDL-Cholesterin, HDL-Cholesterin, Triglyzeride, Diabetes mellitus, Rauchen, familiäre Belastung, 325 tödliche und nicht-tödliche Herzinfarkte bei 4818 Männern im Alter von Jahren.")
133
Beobachtete Herzinfarkte
PROCAM Score Beobachtete Herzinfarkte (per 1000) in 10 Jahren PROCAM Score geschätztes Herzinfarkt- risiko in 10 Jahren (%) < 40 Prävalenz (%) Assmann, Cullen, Schulte; Circulation, 105: ; 2002
 in 10 Jahren. PROCAM Score. geschätztes Herzinfarkt- risiko in 10 Jahren (%) < 40. Prävalenz (%) Assmann, Cullen, Schulte; Circulation, 105: ;")
135
Wenn Sie die Gesamtpunktzahl ermittelt haben, können Sie in dieser Tabelle ablesen, wie hoch das Risiko ist, innerhalb von 10 Jahren einen Herzinfarkt zu erleiden oder an einer koronaren Herzkrankheit zu versterben. Der PROCAM Score wurde aus den Daten von jährigen Männern abgeleitet. Die Anzahl der in der PROCAM Studie aufgetretenen Herzinfarkte bei Frauen erlaubt zur Zeit leider noch nicht die Ableitung eines Scores speziell für Frauen.

137
PROCAM Score Anzahl der Punkte 20 21 22 23 24 25 26 27 28 29 30 31
32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 Herzinfarkt- risiko in 10 Jahren (%) 1.0 1.1 1.2 1.3 1.4 1.6 1.7 1.8 1.9 2.3 2.4 2.8 2.9 3.3 3.5 4.0 4.2 4.8 5.1 5.7 6.1 7.0 7.4 8.0 8.8 10.2 10.5 10.7 12.8 13.2 15.5 16.8 17.5 19.6 21.7 22.2 23.8 25.1 28.0 29.4 30.0 Assmann, Cullen, Schulte; Circulation, 105: ; 2002
 Assmann, Cullen, Schulte; Circulation, 105: ;")
138
Interpretation des 10-Jahres-KHK-Risikos

141
Potenziell neue Risikofaktoren

143
Management of Major Risk Factors
Lifestyle modification Blood pressure targets LDL cholesterol targets Low HDL Diabetes mellitus KW: guidelines, risk factor, LDL, HDL, diabetes, blood pressure, life style

144
Lifestyle Modification
Smoking cessation Weight reduction Healthy diet Regular exercise KW: guidelines, risk factor, life style, obesity

145
Blood Pressure Targets
High-risk patients - BP < 130/85 mmHg Other risk categories - BP < 140/90 mmHg KW: guidelines, risk factor, blood pressure

146
LDL Cholesterol Targets
High-risk patients - < 100 mg/dl (2.6 mmol/L) Intermediate-risk patients - < 130 mg/dl (3.4 mmol/L) Lower- to moderate-risk patients - < 160 mg/dl (4.1 mmol/L) KW: guidelines, risk factor, LDL
 Intermediate-risk patients. - < 130 mg/dl (3.4 mmol/L) Lower- to moderate-risk patients. - < 160 mg/dl (4.1 mmol/L) KW: guidelines, risk factor, LDL.")
147
NCEP ATP III: LDL-C Goals (2004 proposed modifications)
Moderately High Risk ≥ 2 risk factors (10-yr risk 10-20%) Moderate Risk ≥ 2 risk factors (10-yr risk <10%) Lower Risk < 2 risk factors High Risk CHD or CHD risk equivalents (10-yr risk >20%) 190 - Target 160 mg/dL 160 - Target 130 mg/dL or optional 100 mg/dL** Target 130 mg/dL LDL-C level 130 - Target 100 mg/dL or optional 70 mg/dL* 100 - This slide provides a graphic representation of the NCEP ATP III LDL-C goals.1 The goal of therapy in patients at high risk ie. with CHD or CHD risk equivalents is to reduce LDL-C to 100 mg/dL (2.6 mmol/L) and in patients at very high risk there is now a proposed therapeutic option to reduce LDL-C to <70 mg/dL (1.8 mmol/L). This also extends to moderately high-risk persons with a baseline LDL-C of 100 to 129 mg/dL. When LDL-C lowering drug therapy is employed in high-risk or moderately high-risk patients, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. The degree of risk should indicate the severity of intervention. Less aggressive intervention may be warranted if fewer risk factors are present. The LDL-C cut-off is 160 mg/dL (4.1 mmol/L) for patients with fewer than two risk factors. Reference 1. Grundy SM, Cleeman JI, Merz NB et al. Circulation 2004;110: 70 - *Therapeutic option in very high-risk patients and in patients with high TG, non-HDL-C<100 mg/dL; ** Therapeutic option; 70 mg/dL =1.8 mmol/L; 100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L Grundy SM et al. Circulation 2004;110:
 Moderate Risk. ≥ 2 risk factors. (10-yr risk <10%) Lower Risk. < 2 risk factors. High Risk. CHD or CHD risk equivalents. (10-yr risk >20%) Target mg/dL Target mg/dL. or optional. 100 mg/dL** Target mg/dL. LDL-C level Target mg/dL. or optional. 70 mg/dL* This slide provides a graphic representation of the NCEP ATP III LDL-C goals.1 The goal of therapy in patients at high risk ie. with CHD or CHD risk equivalents is to reduce LDL-C to 100 mg/dL (2.6 mmol/L) and in patients at very high risk there is now a proposed therapeutic option to reduce LDL-C to <70 mg/dL (1.8 mmol/L). This also extends to moderately high-risk persons with a baseline LDL-C of 100 to 129 mg/dL. When LDL-C lowering drug therapy is employed in high-risk or moderately high-risk patients, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. The degree of risk should indicate the severity of intervention. Less aggressive intervention may be warranted if fewer risk factors are present. The LDL-C cut-off is 160 mg/dL (4.1 mmol/L) for patients with fewer than two risk factors. Reference. 1. Grundy SM, Cleeman JI, Merz NB et al. Circulation 2004;110: *Therapeutic option in very high-risk patients and in patients with high TG, non-HDL-C<100 mg/dL; ** Therapeutic option; 70 mg/dL =1.8 mmol/L; 100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L. Grundy SM et al. Circulation 2004;110:")
148
HDL Cholesterol Management
General goal: raise HDL Lifestyle modification first Reduce global risk KW: guidelines, risk factor, HDL

149
Diabetes Mellitus Management
Glycohemoglobin Target < 7 percent KW: guidelines, risk factor, diabetes

150
NCEP ATP III Guidelines: CAD Risk Factors
Major risk factors account for only about half of the variation in CAD risk in the US. Additional significant risk factors have been identified, although none are presently categorized as major. These “emerging” risk factors deserve further consideration. Certain of these appear to have significant predictive power in assessing future CAD risk. Emerging risk factors are classified in NCEP ATP III as lipid, nonlipid, or as subclinical atherosclerotic disease. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:
 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:")
151
NCEP ATP III Guidelines: Emerging Lipid Risk Factors for CAD
Emerging lipid risk factors include elevated triglycerides, lipoprotein remnants, lipoprotein (a) [Lp(a)], small LDL particles, HDL subspecies, apolipoproteins, and TC/HDL-C ratio. Elevated triglyceride levels are effective as markers for atherogenic remnant lipoproteins and other factors commonly associated with metabolic syndrome. Relevant studies indicate a strong association between Lp(a) levels and CAD risk. A recent meta-analysis supports the independent predictive power of Lp(a) as a risk factor. Although LDL particle sizing is not recommended for routine CAD risk assessment, studies exist to support its predictive significance. While HDL-C is a long-established risk indicator for CAD, HDL subfractions have also figured in risk prediction. Apo B and Apo A-1 are elements of LDL and HDL, respectively. Neither is currently measurable in standard assays, although non–HDL-C is seen as a useful “surrogate” marker for Apo B. Applicable studies demonstrate a strong predictive power for TC/HDL-C ratios in assessing CAD risk. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:
 [Lp(a)], small LDL particles, HDL subspecies, apolipoproteins, and TC/HDL-C ratio. Elevated triglyceride levels are effective as markers for atherogenic remnant lipoproteins and other factors commonly associated with metabolic syndrome. Relevant studies indicate a strong association between Lp(a) levels and CAD risk. A recent meta-analysis supports the independent predictive power of Lp(a) as a risk factor. Although LDL particle sizing is not recommended for routine CAD risk assessment, studies exist to support its predictive significance. While HDL-C is a long-established risk indicator for CAD, HDL subfractions have also figured in risk prediction. Apo B and Apo A-1 are elements of LDL and HDL, respectively. Neither is currently measurable in standard assays, although non–HDL-C is seen as a useful surrogate marker for Apo B. Applicable studies demonstrate a strong predictive power for TC/HDL-C ratios in assessing CAD risk. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:")
152
NCEP ATP III Guidelines: Emerging Nonlipid Risk Factors for CAD
Other emerging nonlipid risk factors include homocysteine, thrombotic factors, inflammatory markers, and impaired fasting glucose. The atherosclerotic process is known to involve chronic inflammation, and arterial inflammation is receiving heightened attention as a viable risk factor for CAD. Serum inflammatory markers, eg, C-reactive protein (CRP), appear to be reliable predictors of CAD. Some investigators suggest that patients with elevated CRP should be assigned more aggressive lipid-lowering goals. Thrombosis plays a significant role in acute coronary syndromes, including myocardial infarction, and elevations in prothrombotic factors such as fibrinogen and plasminogen activator inhibitor-1 have been associated with metabolic syndrome. Although some researchers believe impaired fasting glucose to be an independent risk factor, others believe that any predictive capability of impaired fasting glucose may result simply from its strong link with metabolic syndrome. The use of homocysteine as a risk indicator is an option for low-risk patients with a strong family history of premature CAD. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:
, appear to be reliable predictors of CAD. Some investigators suggest that patients with elevated CRP should be assigned more aggressive lipid-lowering goals. Thrombosis plays a significant role in acute coronary syndromes, including myocardial infarction, and elevations in prothrombotic factors such as fibrinogen and plasminogen activator inhibitor-1 have been associated with metabolic syndrome. Although some researchers believe impaired fasting glucose to be an independent risk factor, others believe that any predictive capability of impaired fasting glucose may result simply from its strong link with metabolic syndrome. The use of homocysteine as a risk indicator is an option for low-risk patients with a strong family history of premature CAD. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:")
153
NCEP ATP III Guidelines (2004 proposed modifications)
Initiate TLC* Drug therapy Patients with LDL-C goal if LDL-C considered if LDL-C High risk: CHD or CHD risk equivalents (10-year risk >20%) <100 mg/dL† (optional goal: <70 mg/dL†) 100 mg/dL (<100 mg/dL: drug optional) 100 mg/dL† Moderately high risk: >2 risk factors (10-year risk 10-20%) <130 mg/dL† (optional goal: <100 mg/dL†) 130 mg/dL† 130 mg/dL ( mg/dL: drug optional) Moderate risk: >2 risk factors (10-year risk <10%) <130 mg/dL† 130 mg/dL† 160 mg/dL† Based on recent clinical trial evidence, an NCEP report1 has been published recommending tighter control of cholesterol management. The trials support an LDL-C goal of <100 mg/dL in high-risk patients, and the inclusion of diabetes in the high-risk category. All patients with CHD or CHD risk equivalents are at high-risk. CHD risk equivalents include noncoronary forms of clinical atherosclerotic disease, diabetes and multiple risk factors with a 10-year risk for CHD >10%. Therapeutic lifestyle changes (TLC) remain an essential part of clinical management. In patients at high risk (CHD and CHD risk equivalents, 10-year risk >20%), the recommended LDL-C goal is <100 mg/dL, but when risk is very high, an LDL-C goal of <70 mg/dL (1.8 mmol/dL) is a proposed therapeutic option based on clinical trial evidence. The recommended point at which TLC should be initiated is an LDL-C level of 100 mg/dL (2.6 mmol/L). The guidelines recommend that drug therapy be considered in this category simultaneously with TLC in persons whose LDL-C levels are 100 mg/dL (2.6 mmol/L) In patients at moderately high risk (>2 risk factors and 10-year CHD risk of 10–20%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L), but an LDL-C goal of <100 mg/dL (2.6 mmol/L) is a therapeutic option based on clinical trial evidence. This also applies to patients with a baseline LDL-C of mg/dL. Drug therapy should be considered if LDL-C levels remain 130 mg/dL (3.4 mmol/L), after 3 months of TLC. In patients at moderate risk (>2 risk factors and 10-year CHD risk of <10%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L). In this group drug therapy should be considered at LDL-C levels 160 mg/dL (4.1 mmol/L), In individuals at lower risk (0–1 risk factor) and whose LDL-C levels are 160 mg/dL (4.1 mmol/L), TLC are recommended. Drug therapy should be considered when LDL-C levels are 190 mg/dL (5 mmol/L) despite TLC, and is optional depending on clinical judgement at LDL-C levels of 160–189 mg/dL (4.1-5 mmol/L). The goal for LDL-C in this risk category is <160 mg/dL (4.1 mmol/L). When LDL-C lowering drug therapy is employed in high-risk or moderately high-risk patients, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. Moreover, any person at high risk or moderately high risk who has life-style related risk factors (eg obesity, physical inactivity, elevated TG, low HDL-C or the metabolic syndrome) is a candidate for TLC to modify these risk factors regardless of LDL-C level. Reference 1. Grundy SM, Cleeman JI, Merz NB et al. Circulation 2004;110: Lower risk: 0-1 risk factors <160 mg/dL† 160 mg/dL† 190 mg/dL† ( mg/dL: drug optional) †70 mg/dL = 1.8 mmol/L; 100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L; 190 mg/dL = 5 mmol/L: * TLC: therapeutic lifestyle changes Grundy SM et al. Circulation 2004;110:
 <100 mg/dL† (optional goal: <70 mg/dL†) 100 mg/dL. (<100 mg/dL: drug optional) 100 mg/dL† Moderately high risk: >2 risk factors (10-year risk 10-20%) <130 mg/dL† (optional goal: <100 mg/dL†) 130 mg/dL† 130 mg/dL. ( mg/dL: drug optional) Moderate risk: >2 risk factors (10-year risk <10%) <130 mg/dL† 130 mg/dL† 160 mg/dL† Based on recent clinical trial evidence, an NCEP report1 has been published recommending tighter control of cholesterol management. The trials support an LDL-C goal of <100 mg/dL in high-risk patients, and the inclusion of diabetes in the high-risk category. All patients with CHD or CHD risk equivalents are at high-risk. CHD risk equivalents include noncoronary forms of clinical atherosclerotic disease, diabetes and multiple risk factors with a 10-year risk for CHD >10%. Therapeutic lifestyle changes (TLC) remain an essential part of clinical management. In patients at high risk (CHD and CHD risk equivalents, 10-year risk >20%), the recommended LDL-C goal is <100 mg/dL, but when risk is very high, an LDL-C goal of <70 mg/dL (1.8 mmol/dL) is a proposed therapeutic option based on clinical trial evidence. The recommended point at which TLC should be initiated is an LDL-C level of 100 mg/dL (2.6 mmol/L). The guidelines recommend that drug therapy be considered in this category simultaneously with TLC in persons whose LDL-C levels are 100 mg/dL (2.6 mmol/L) In patients at moderately high risk (>2 risk factors and 10-year CHD risk of 10–20%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L), but an LDL-C goal of <100 mg/dL (2.6 mmol/L) is a therapeutic option based on clinical trial evidence. This also applies to patients with a baseline LDL-C of mg/dL. Drug therapy should be considered if LDL-C levels remain 130 mg/dL (3.4 mmol/L), after 3 months of TLC. In patients at moderate risk (>2 risk factors and 10-year CHD risk of <10%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L). In this group drug therapy should be considered at LDL-C levels 160 mg/dL (4.1 mmol/L), In individuals at lower risk (0–1 risk factor) and whose LDL-C levels are 160 mg/dL (4.1 mmol/L), TLC are recommended. Drug therapy should be considered when LDL-C levels are 190 mg/dL (5 mmol/L) despite TLC, and is optional depending on clinical judgement at LDL-C levels of 160–189 mg/dL (4.1-5 mmol/L). The goal for LDL-C in this risk category is <160 mg/dL (4.1 mmol/L). When LDL-C lowering drug therapy is employed in high-risk or moderately high-risk patients, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. Moreover, any person at high risk or moderately high risk who has life-style related risk factors (eg obesity, physical inactivity, elevated TG, low HDL-C or the metabolic syndrome) is a candidate for TLC to modify these risk factors regardless of LDL-C level. Reference. 1. Grundy SM, Cleeman JI, Merz NB et al. Circulation 2004;110: Lower risk: 0-1 risk factors. <160 mg/dL† 160 mg/dL† 190 mg/dL† ( mg/dL: drug optional) †70 mg/dL = 1.8 mmol/L; 100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L; 190 mg/dL = 5 mmol/L: * TLC: therapeutic lifestyle changes. Grundy SM et al. Circulation 2004;110:")
154
2003 European Guidelines: Guide to lipid management in asymptomatic subjects
Estimate total CVD risk of fatal CVD event in 10 years using SCORE chart Total CVD risk <5% TC 5 mmol/L (190 mg/dL) Total CVD risk 5% Measure fasting lipids, give lifestyle advice, with repeat lipids after 3 months Lifestyle advice Aim: TC<5 mmol/L (190 mg/dL) LDL-C <3.0 mmol/L (115 mg/dL) Follow-up at 5-year intervals TC <5 mmol/L (190 mg/dL) and LDL-C <3.0 mmol/L (115 mg/dL) Maintain lifestyle advice with annual follow-up. If total risk remains 5%, consider drugs to lower TC to <4.5 mmol/L (175 mg/dL) and LDL-C to <2.5 mmol/L (100 mg/dL) TC 5 mmol/L (190 mg/dL) or LDL-C 3 mmol/L (115 mg/dL) Maintain lifestyle advice and start drug therapy The prevention of CHD in patients with established CHD or other atherosclerotic disease, and in asymptomatic healthy prevention actions should be guided in accordance with the total CVD risk level. Most recently, the Third Joint Task Force of European and other Societies on Cardiovascular Disease Prevention in Clinical Practice1 has provided guidelines using a simplified risk analysis chart, the SCORE (Systemic Coronary Risk Evaluation) system, which includes factors such as age, gender, smoking, total cholesterol or the cholesterol/HDL ratio and systolic blood pressure. There are now two charts, a low-risk chart used in Belgium, France, Greece, Italy, Luxembourg, Spain, Switzerland and Portugal and a high-risk chart used in all other European countries. The SCORE system provides a risk assessment for the probability of a fatal CVD event over 10 years. With respect to blood lipids, recommended treatment goals include a total cholesterol consistently below 5.0 mmol/L (190 mg/dL) and an LDL-C below 3.0 mmol/L (115 mg/dL). For patients with clinically established CVD and patients with diabetes the treatment goals should be lower: total cholesterol <4.5 mmol/L (175 mg/dL) and LDL-C <2.5 mmol/L (100 mg/dL). If lifestyle changes fail to reach these targets, drug therapy should be initiated. Concentrations of HDL-C and triglycerides are not used as goals of therapy. However, an HDL-C <1.0 mmol/L (40 mg/dL) in men and <1.2 mmol/L (46 mg/dL) in women, and fasting triglycerides >1.7 mmol/L (150 mg/dL) are markers of increased coronary risk. Reference 1. De Backer G, Ambrosioni E, Borch-Johnsen K et al. Eur Heart J 2003;24: De Backer G et al. Eur Heart J 2003;24:1601–1610.
 Total CVD risk 5% Measure fasting lipids, give lifestyle. advice, with repeat lipids after. 3 months. Lifestyle advice. Aim: TC<5 mmol/L (190 mg/dL) LDL-C <3.0 mmol/L (115 mg/dL) Follow-up at 5-year intervals. TC <5 mmol/L (190 mg/dL) and LDL-C <3.0 mmol/L (115 mg/dL) Maintain lifestyle advice with annual. follow-up. If total risk remains 5%, consider drugs to lower TC to <4.5 mmol/L. (175 mg/dL) and LDL-C to. <2.5 mmol/L (100 mg/dL) TC 5 mmol/L (190 mg/dL) or. LDL-C 3 mmol/L (115 mg/dL) Maintain lifestyle. advice and start drug. therapy. The prevention of CHD in patients with established CHD or other atherosclerotic disease, and in asymptomatic healthy prevention actions should be guided in accordance with the total CVD risk level. Most recently, the Third Joint Task Force of European and other Societies on Cardiovascular Disease Prevention in Clinical Practice1 has provided guidelines using a simplified risk analysis chart, the SCORE (Systemic Coronary Risk Evaluation) system, which includes factors such as age, gender, smoking, total cholesterol or the cholesterol/HDL ratio and systolic blood pressure. There are now two charts, a low-risk chart used in Belgium, France, Greece, Italy, Luxembourg, Spain, Switzerland and Portugal and a high-risk chart used in all other European countries. The SCORE system provides a risk assessment for the probability of a fatal CVD event over 10 years. With respect to blood lipids, recommended treatment goals include a total cholesterol consistently below 5.0 mmol/L (190 mg/dL) and an LDL-C below 3.0 mmol/L (115 mg/dL). For patients with clinically established CVD and patients with diabetes the treatment goals should be lower: total cholesterol <4.5 mmol/L (175 mg/dL) and LDL-C <2.5 mmol/L (100 mg/dL). If lifestyle changes fail to reach these targets, drug therapy should be initiated. Concentrations of HDL-C and triglycerides are not used as goals of therapy. However, an HDL-C <1.0 mmol/L (40 mg/dL) in men and <1.2 mmol/L (46 mg/dL) in women, and fasting triglycerides >1.7 mmol/L (150 mg/dL) are markers of increased coronary risk. Reference. 1. De Backer G, Ambrosioni E, Borch-Johnsen K et al. Eur Heart J 2003;24: De Backer G et al. Eur Heart J 2003;24:1601–1610.")
155
SCORE: Systematic Coronary Risk Evaluation
De Backer et al. European Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur Heart J 2003 The determination of traditional cardiovascular risk factors like age, gender, elevated total cholesterol, blood pressure, smoking, diabetes mellitus and physical inactivity represent a useful first step in determining who could be at risk for a coronary event. In the era of “Global Risk Assessment” this should be done using one of the available scores, e.g. Framingham score, PROCAM score or the SCORE score of the European Society of Cardiology, derived from multivariable statistical models. KW: SCORE, risk, CVD, risk factor, BP, cholesterol, diabetes

Ähnliche Präsentationen
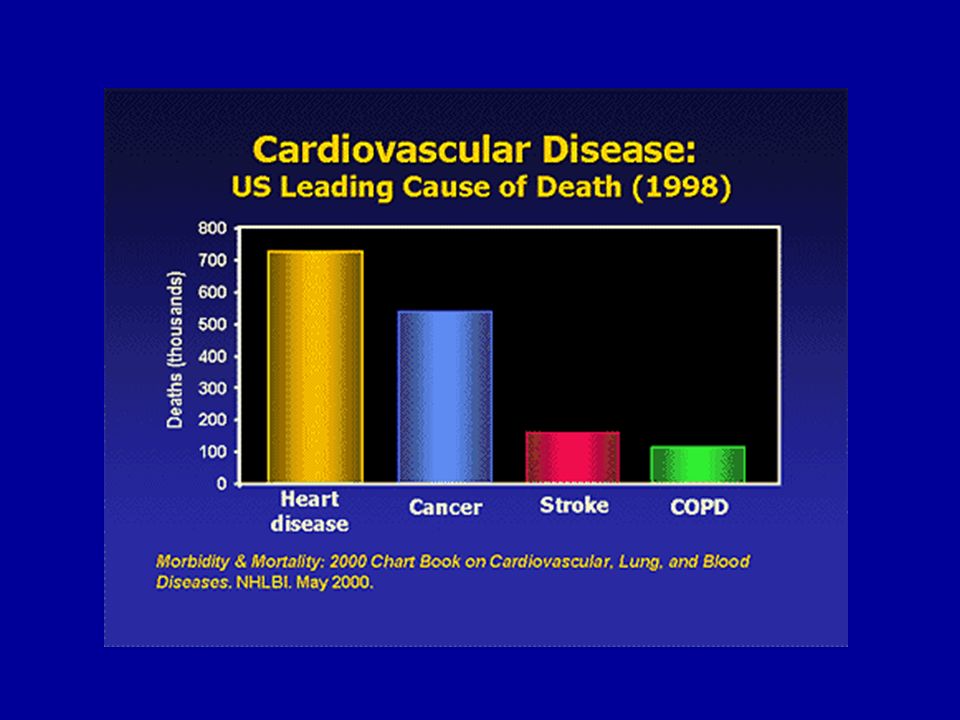

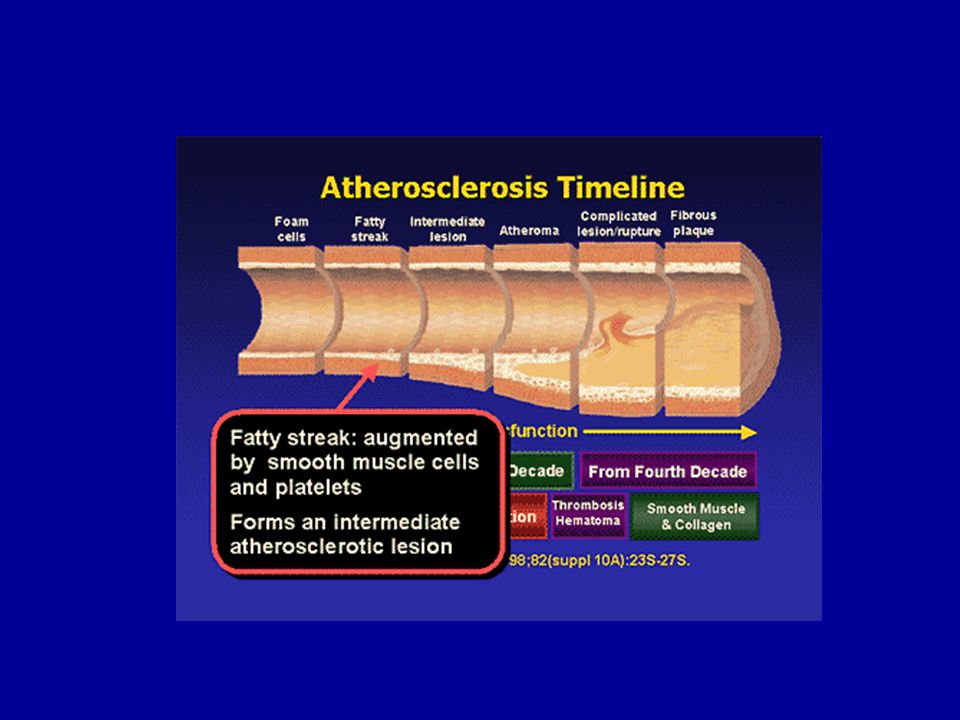
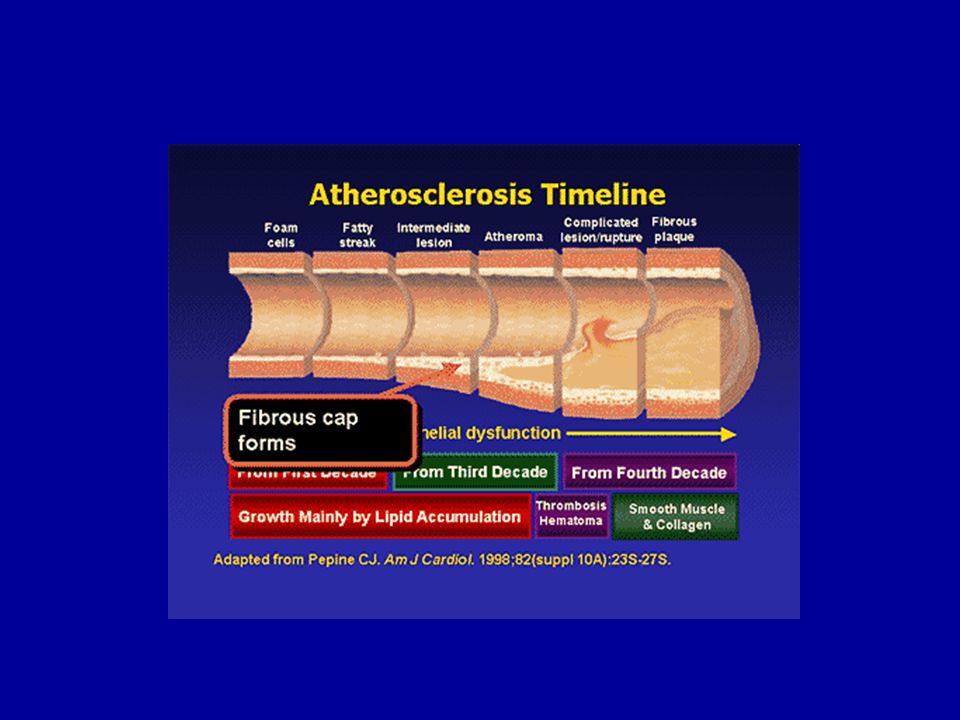
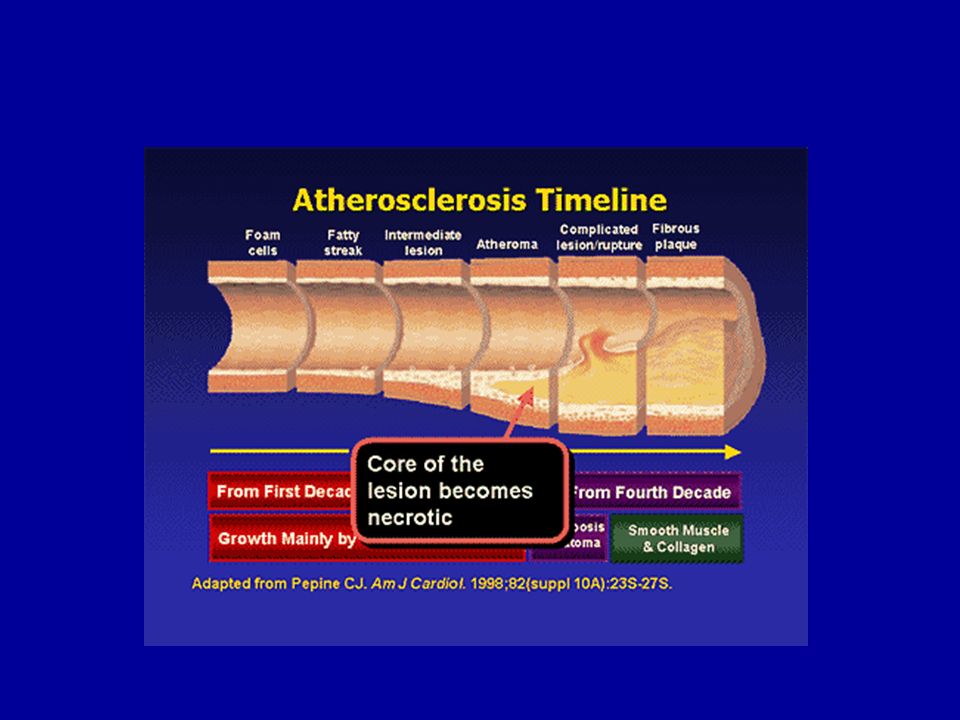
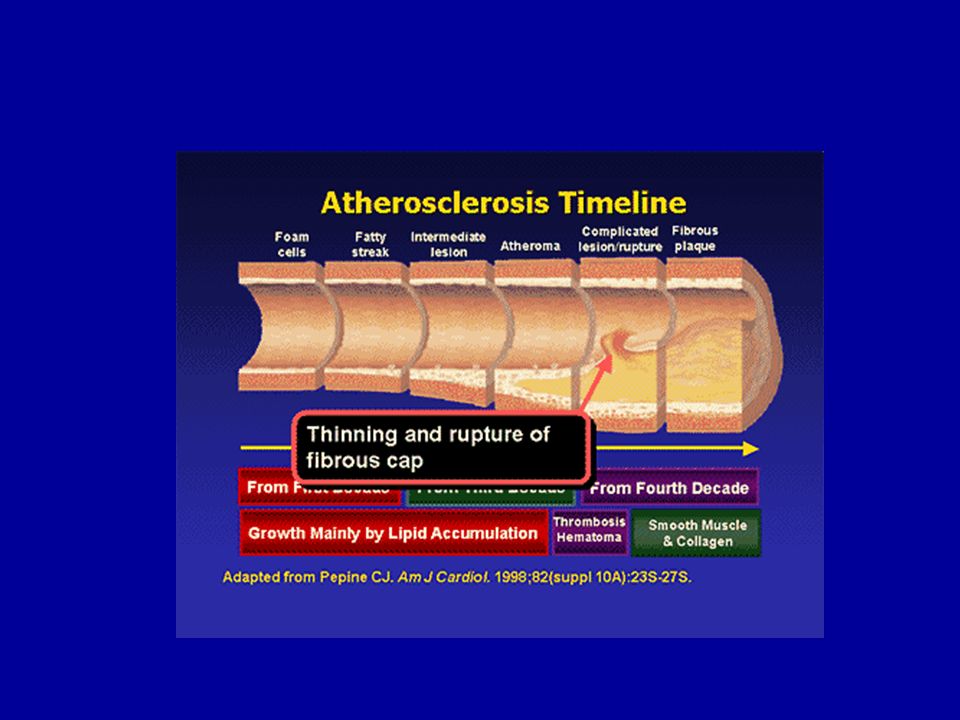

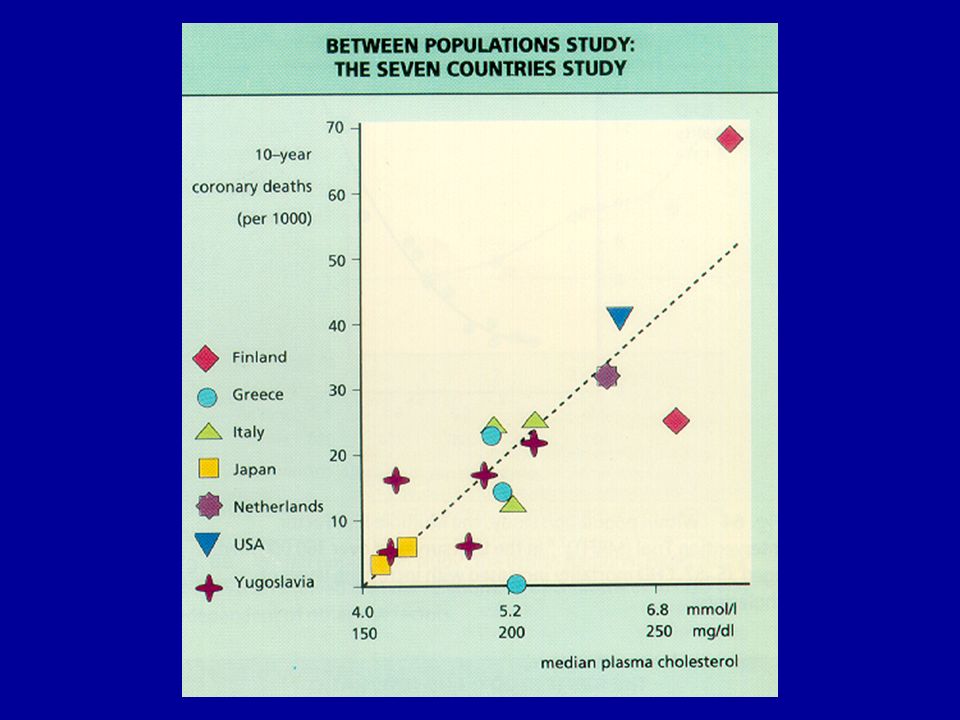
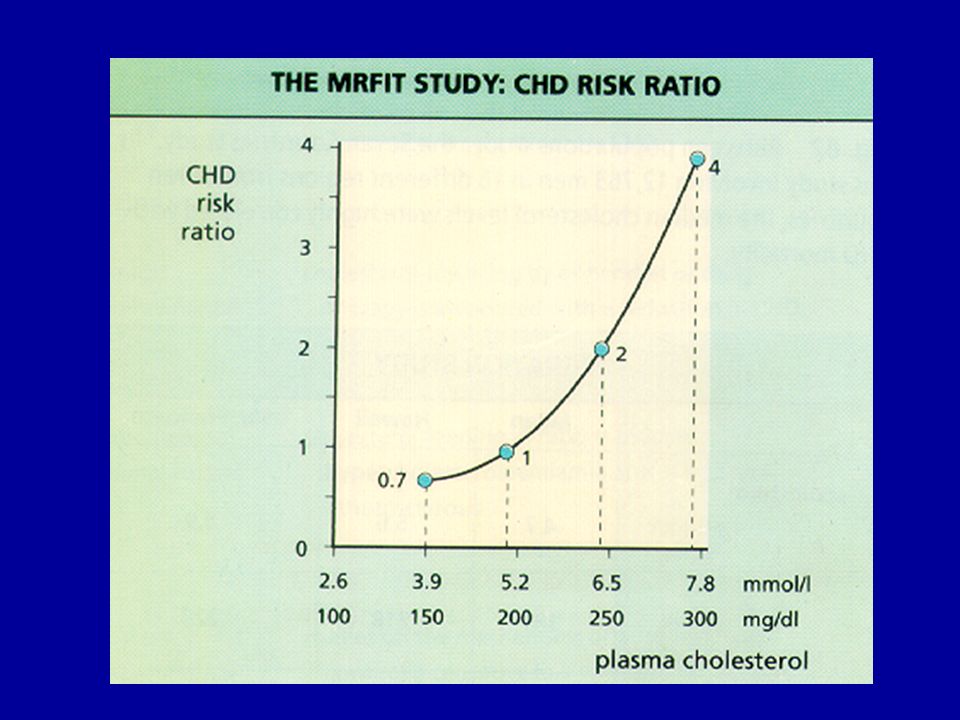
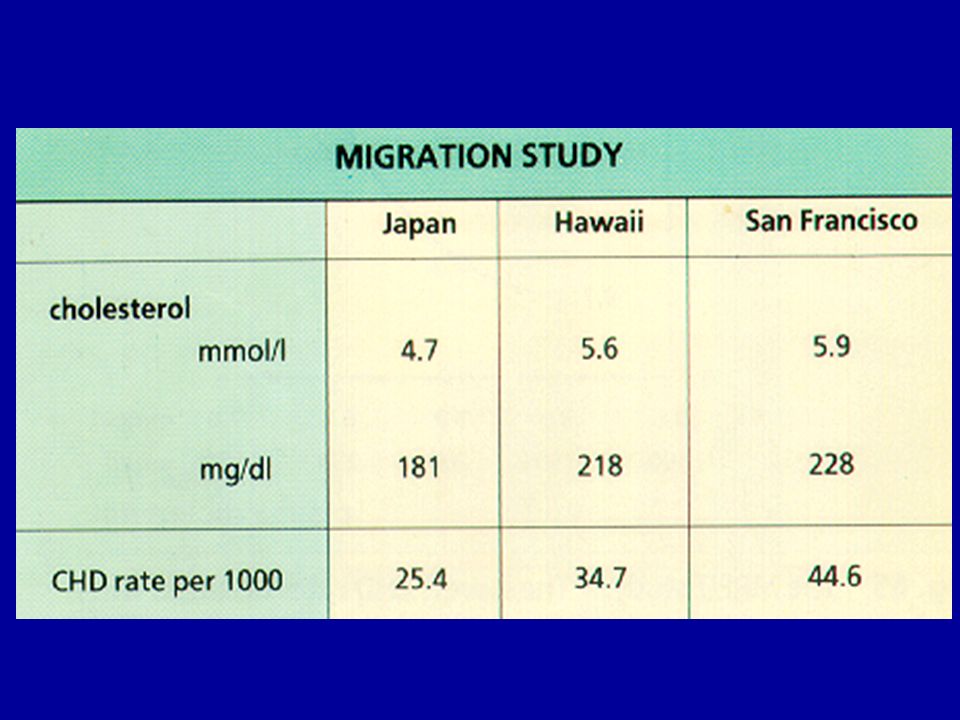
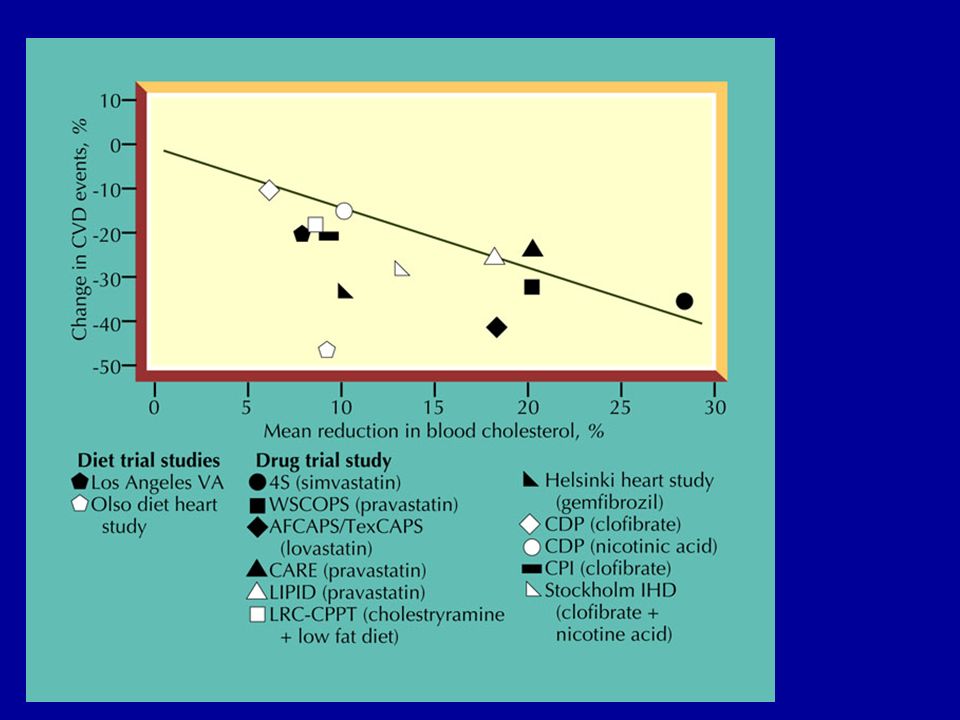
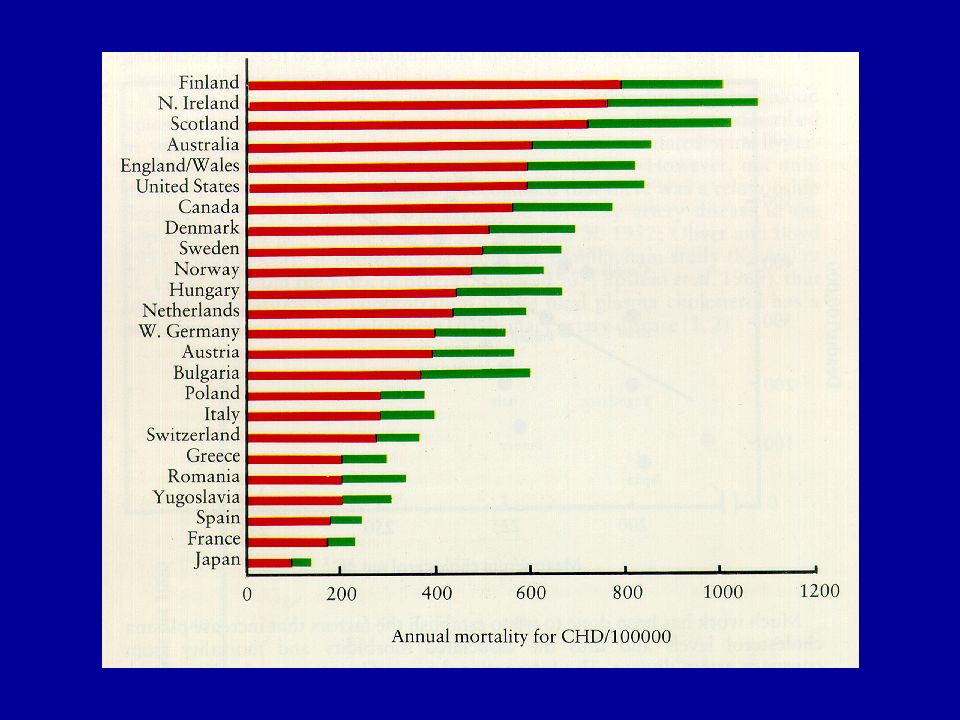

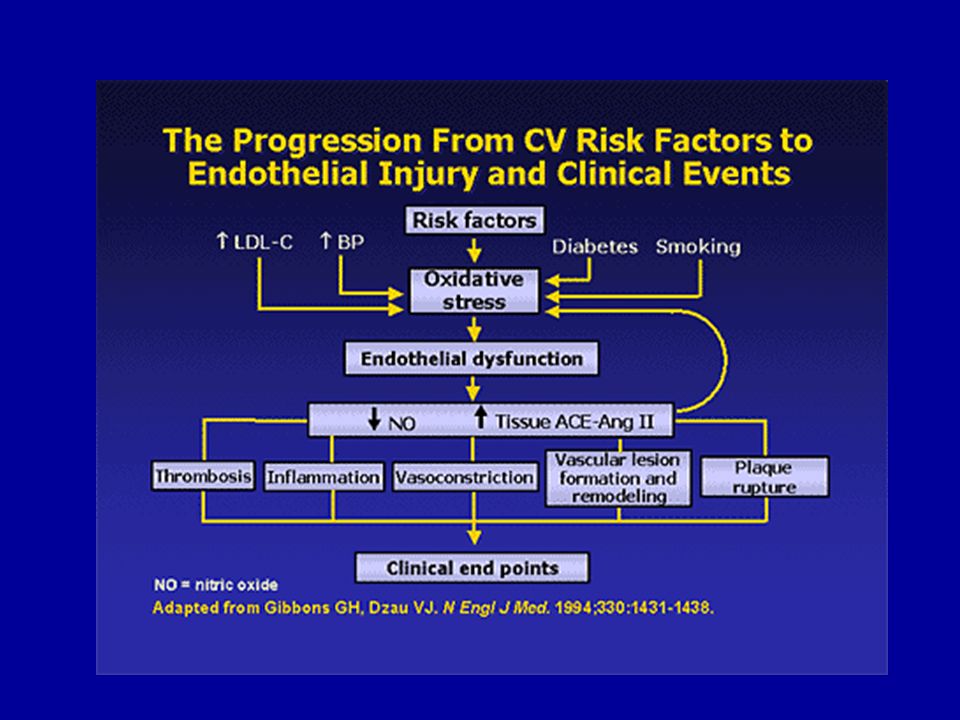

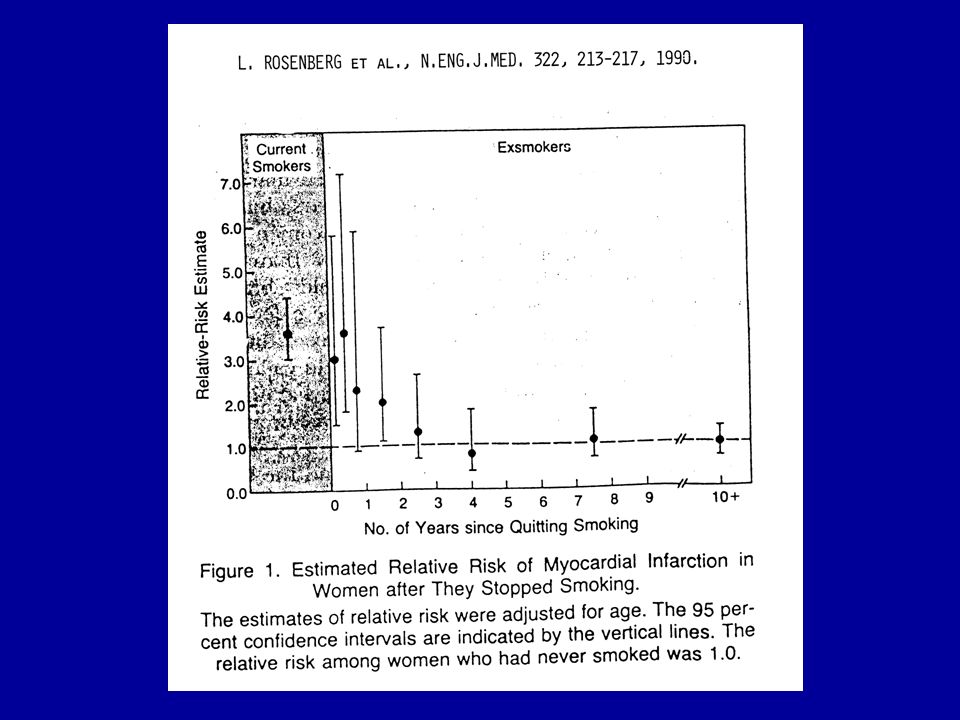
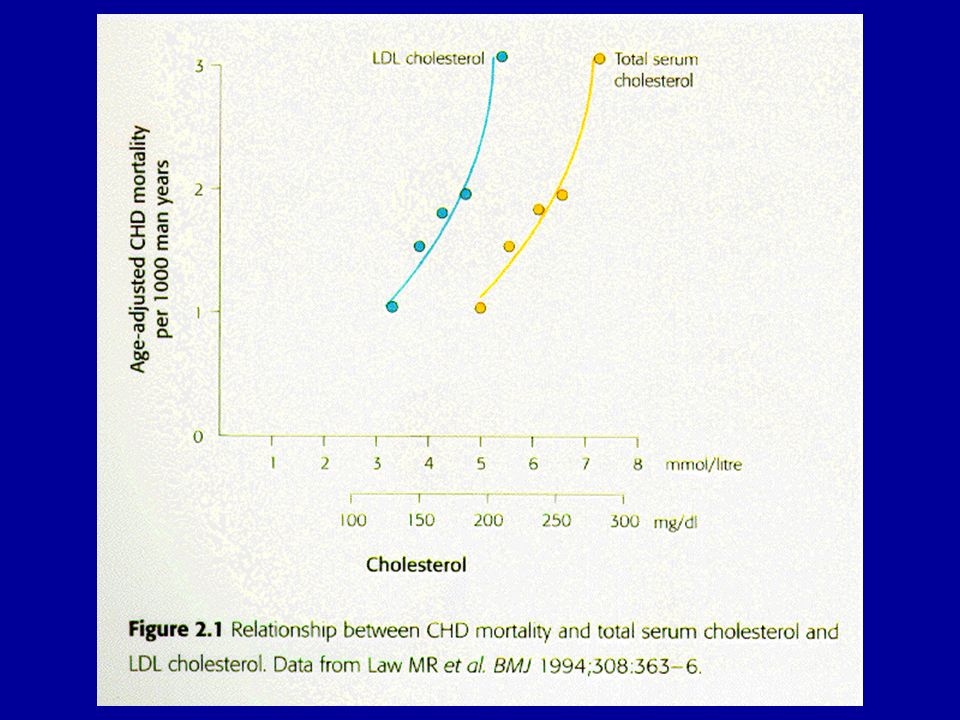
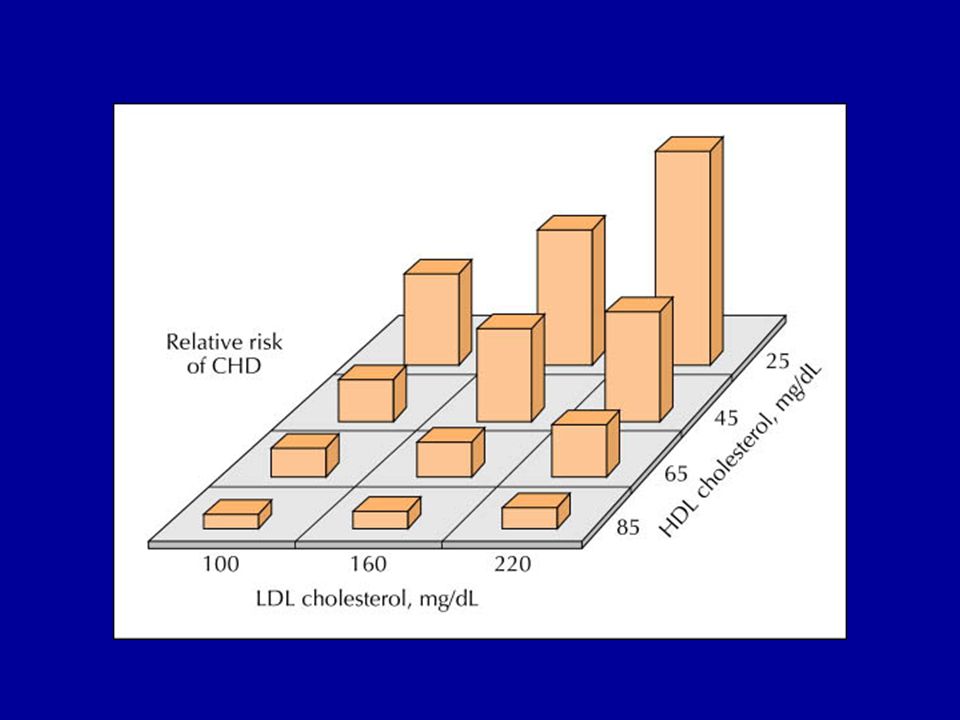
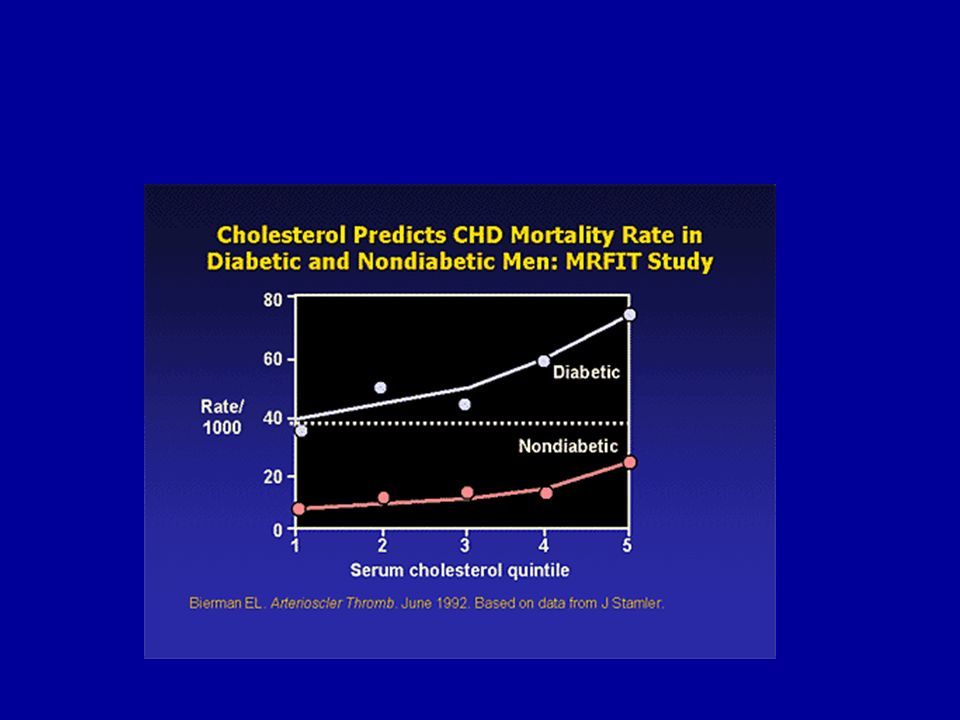
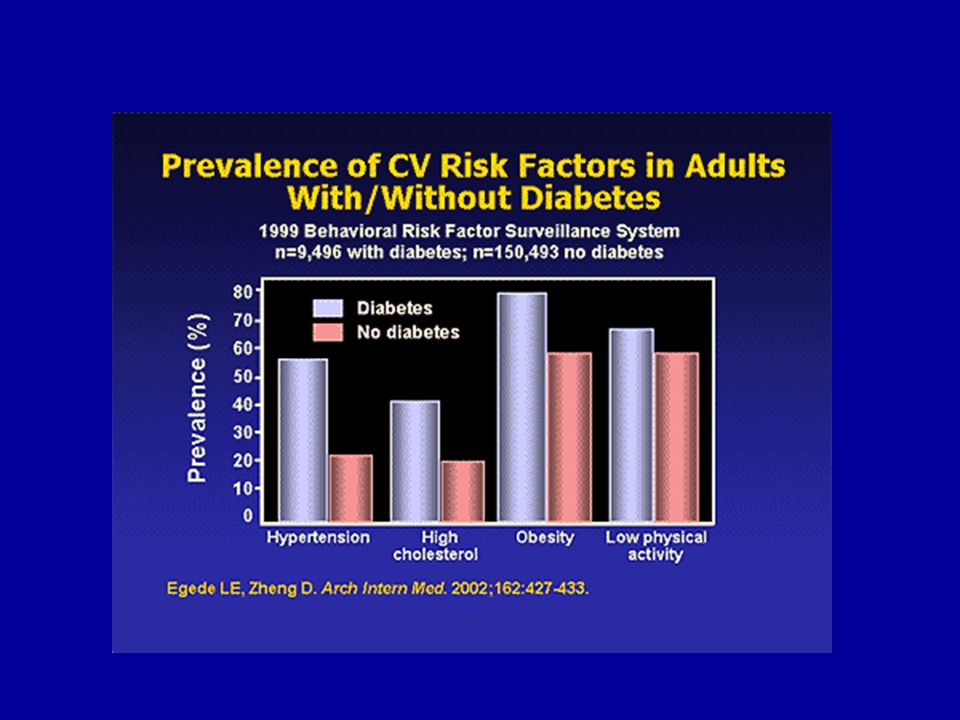
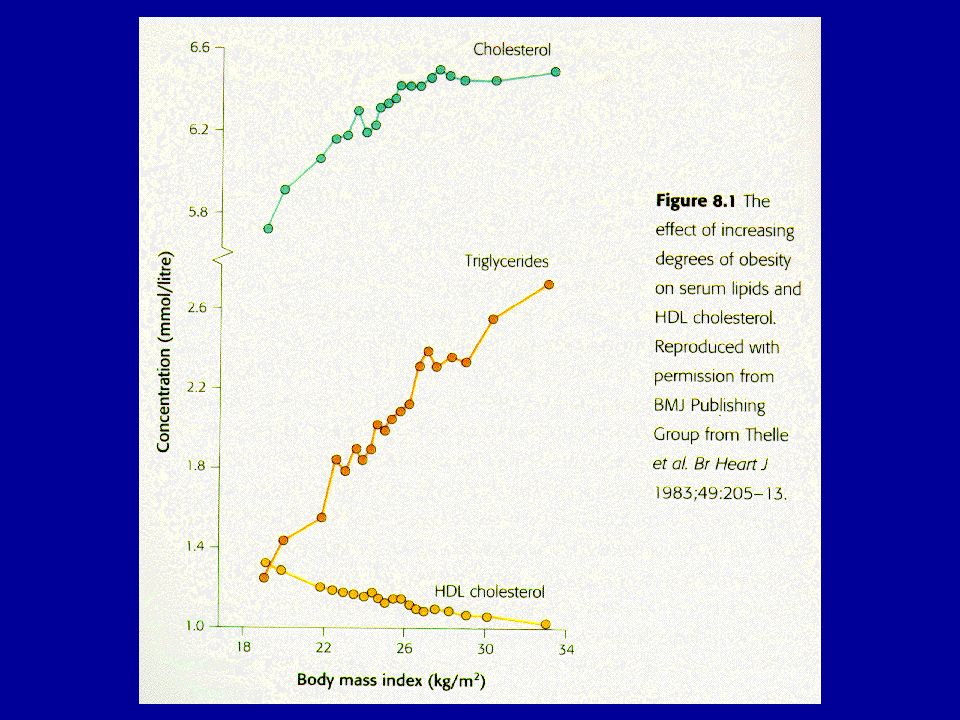

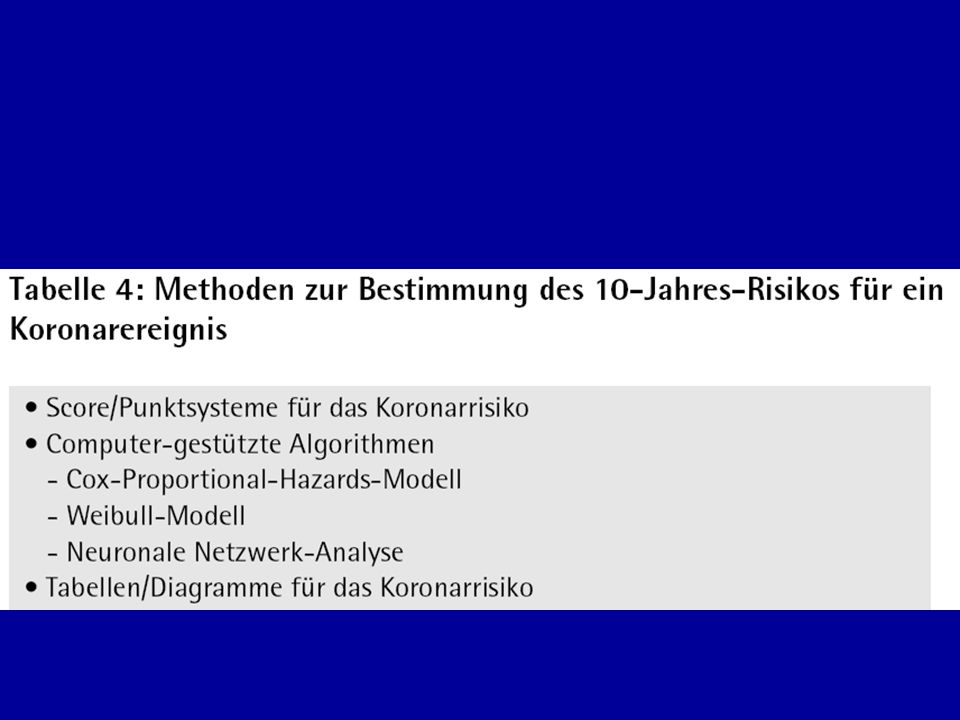
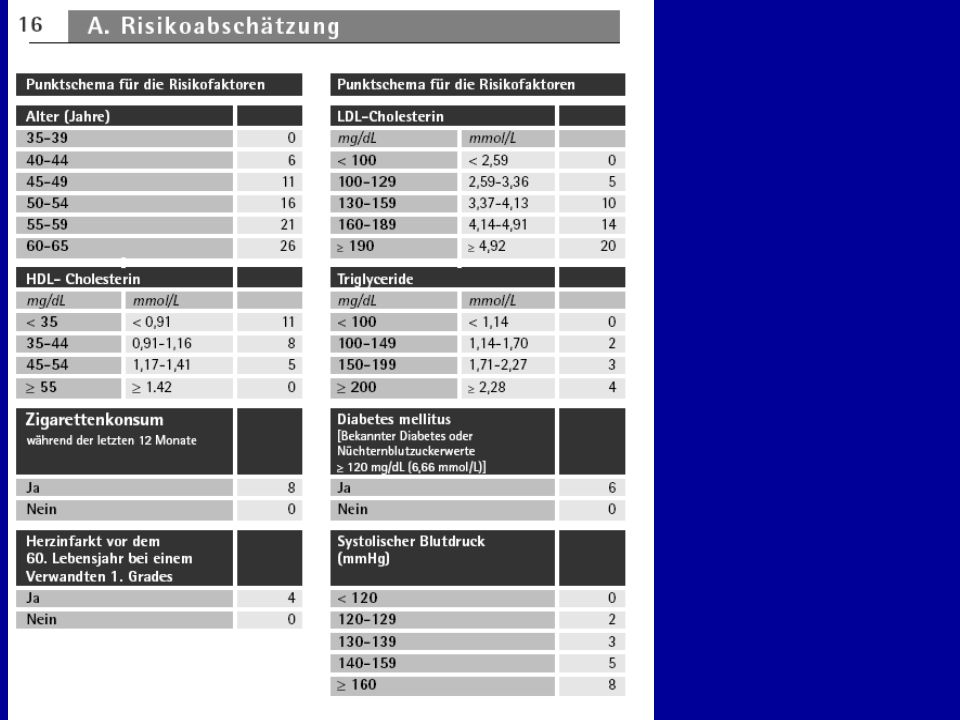
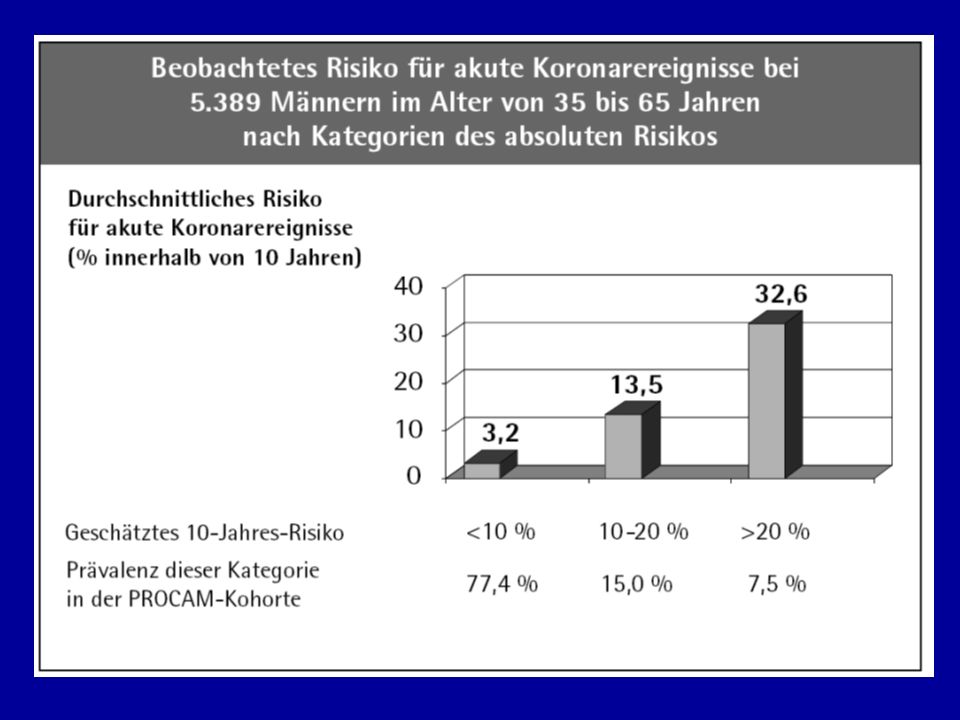
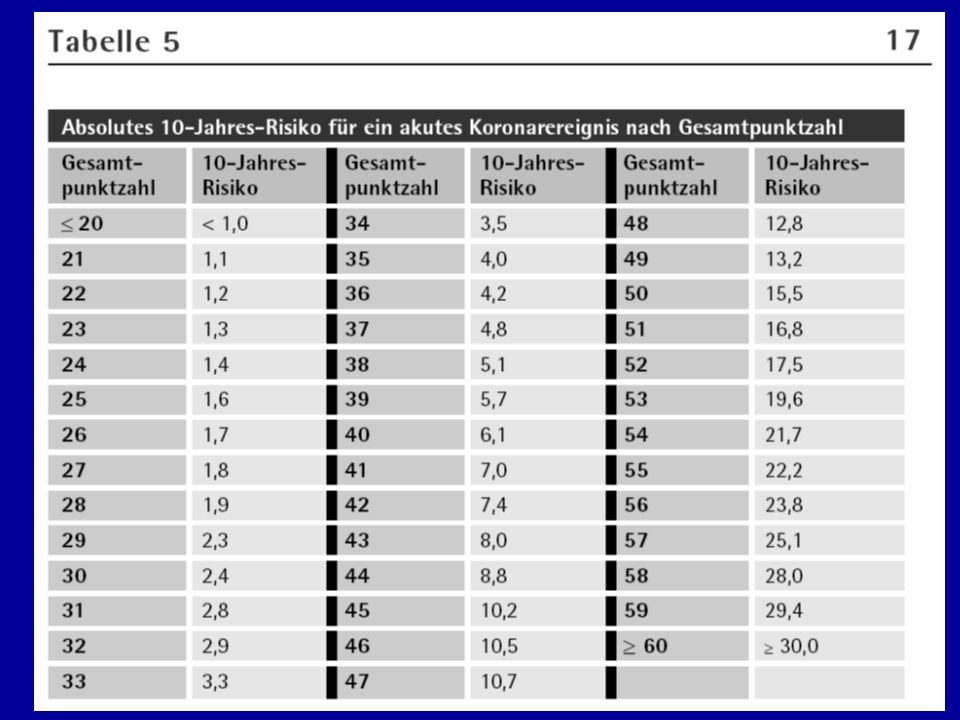

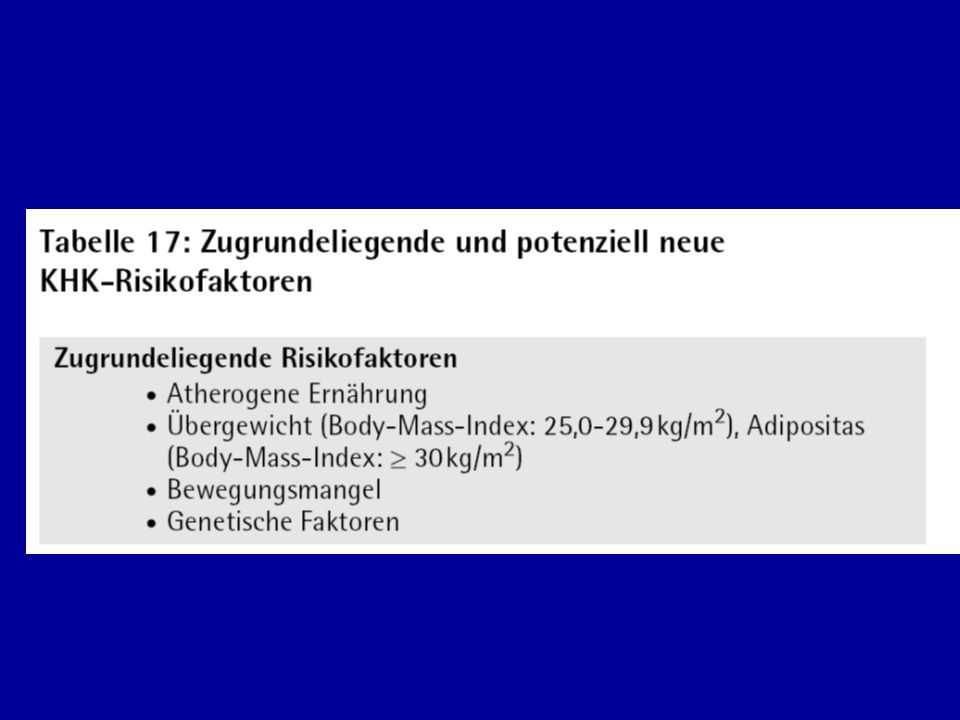












>")

>")
>")




>")
