Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Pap – HPV Impfung? Prophylaxe
Heinz Koelbl Universitätsklinik und Poliklinik für Geburtshilfe und Frauenkrankheiten Johannes-Gutenberg-Universität Mainz European Training Center

2
HPV induzierte Karzinome
Zervixkarzinom Vulvakarzinom: ca. 70% HPV induziert, v.a. junge Frauen Analkarzinom: ca % HPV positiv Peniskarzinome < 3% Larynxca.

3
Vulvakarzinom Inzidenz: ca. 1.5 – 2 pro 100,000 Frauen pro Jahr in Deutschland (Cervix Ca: 12 pro ) ca 400-fache Zunahme der in situ Fälle seit 1973 Ca. 20%-ige Zunahme der invasiven Karzinome seit 1973 Ca. 560 Todesfälle pro Jahr Ca neue Fälle in USA in 2006 erwartet , 880 Todesfälle > 75% HPV-induziert, v.a. junge Frauen auf dem Boden einer VIN III

4
HPV und Zervixkarzinom
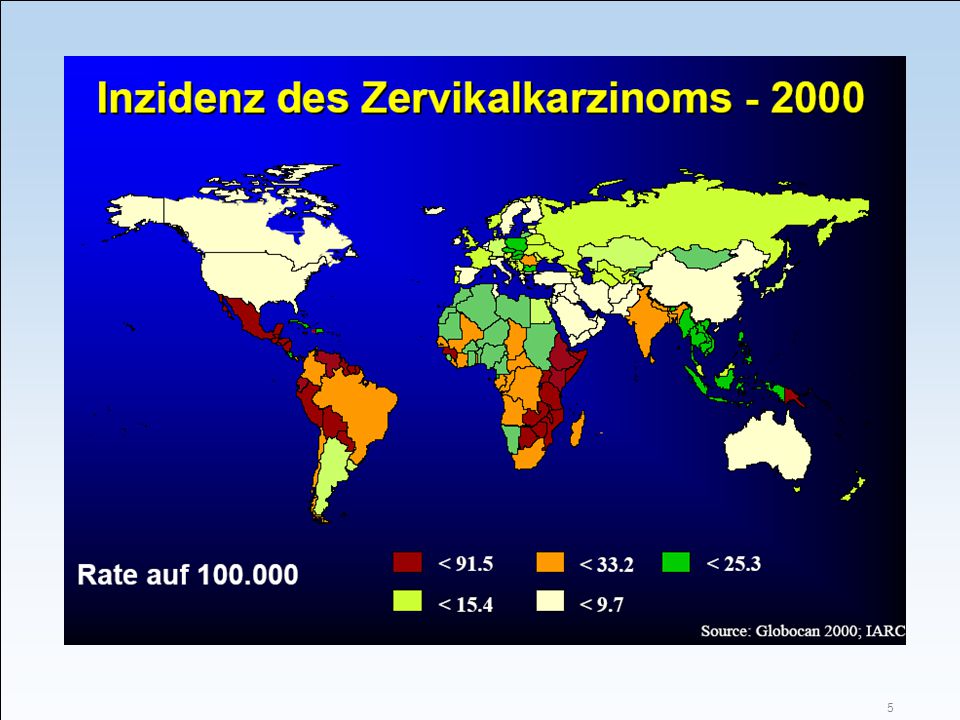
Zervixkarzinom - zweithäufigste Krebserkrankung bei Frauen neue Fälle weltweit Todesfälle pro Jahr in Deutschland ca Neuerkrankungen und Todesfälle pro Jahr Inzidenz: / Frauen Afrika > Lateinamerika > Asien > Europa > USA 80% der Fälle treten in Entwicklungsländern auf Gründe: keine oder mangelhafte Vorsorgeuntersuchung für viele auch einfach nur nicht bezahlbar Weltweit stirbt alle 2 Minuten eine Frau am Zervixkarzinom!

6
Krebsvorsorge des Zervixkarzinoms
1878 Ruge und Veit (Berlin) erste histolog. Cervix-Ca-Dg. 1908 Schauenstein (Graz) 1925 Hinselmann 1. Kolposkop 1928 Papanicolaou erste zytologische Methodik 1943 Papanicolaou und Traut Monographie 1947 Igel (Berlin) Einführung der Zytologie in D 1953 Runge (Heidelberg) Durchbruch der gynäkol. Zytologie 1971 Einführung Screening bei Zervix- Ca George N. Papanicolaou ( )
 erste histolog. Cervix-Ca-Dg Schauenstein (Graz) 1925 Hinselmann 1. Kolposkop Papanicolaou. erste zytologische Methodik Papanicolaou und Traut. Monographie Igel (Berlin) Einführung der Zytologie in D Runge (Heidelberg) Durchbruch der gynäkol. Zytologie Einführung Screening bei Zervix- Ca. George N. Papanicolaou ( )")
7
Nach §25 Abs. 2 SGB V haben alle Frauen ab dem 20. LJ
Nach §25 Abs. 2 SGB V haben alle Frauen ab dem 20. LJ. einmal jährlich Anspruch auf ein Zervixkarzinom-Screening Inzidenzrate von 40,5 / (1971) auf 11,2 / (1996) Mortalität sank in den letzten 15 Jahren um 40 %
 auf 11,2 / (1996) Mortalität sank in den letzten 15 Jahren um 40 %")
8
Teilnahmeraten an Krebsfrüherkennungs- Untersuchungen: Frauen
Quellen: Altenhofen, L. Hochrechnung zur Akzeptanz von Gesundheitsuntersuchungen und Krebsfrüherkennungsuntersuchungen bei gesetzlich Versicherten. Berlin, Zentralinstitut für die kassenärztliche Versorgung in der Bundesrepublik Deutschland; (alle Jahre bis auf 1998, 1999) Quaas J, Schneider V. Was würde ein primäres HPV-Screening in Deutschland kosten? Frauenart 45; 2004: (Jahre 1998, 1999) Verfahrenswechsel bei der Berechnungsgrundlage in 2000! Quellen: Altenhofen 2005, Quaas 2004
 Quaas J, Schneider V. Was würde ein primäres HPV-Screening in Deutschland kosten Frauenart 45; 2004: (Jahre 1998, 1999) Verfahrenswechsel bei der Berechnungsgrundlage in 2000! Quellen: Altenhofen 2005, Quaas")
9
ThinPrep® Pap Test ThinPrep® Pap Test von der FDA Mai 1996 zugelassen

10
Geschichte der Entdeckung der Humanen Papillomviren
1976 zur Hausen postuliert, dass Papillomviren an der Pathogenese des Zervixkarzinoms beteiligt sein können 1980 Isolierung von HPV 6 & 11 aus Condylomata accuminata 1982 Klonierung von HPV 16 und 18 aus Biopsien von Zervixkarzinomen 1985 Aufklärung der Genomstruktur der HPVs in den Tumorzellen und der Expression der E6 & E7 Gene 1986 Immortalisierung menschlicher Zellen durch HPV E6 & E7 Gene 1988 Hemmung der Aktivität der Gene E6 & E7 führt zum Verlust der neoplastischen Wachstumseigenschaften Ab 1990 Aufklärung der biochemischen Funktionen der E6 & E7 Gene

11
HPV und Zervixkarzinom
Ca % aller Frauen infizieren sich mit einem HP-Virus. 1-3% der HPV-Infektionen entwickeln sich zu einem invasiven Tumor. Voraussetzung ist eine persistierende HPV- Infektion. 99,7% aller Zervixkarzinome sind mit einer HPV- Infektion assoziiert. In über 70% wird HPV 16 oder HPV 18 gefunden: HPV 16 in 56% HPV 18 in 19%

12
HPV = Auslöser des Zervixkazinoms
„ Eine kausale Rolle der Infektion mit dem HP-Virus beim Zervixkarzinom ist ohne Zweifel dokumentiert.“ „Der Zusammenhang in fast allen Fällen von Zervixkarzinomen weltweit ist offensichtlich.“ Bosch FX et al., The causal relation between human papillomavirus and cervical cancer. J Clin Pathol 2002; 55: 244–65.

13
HPV-Typen: Risikotypen
15 Hoch-Risikotypen verursachen Gebärmutterhalskrebs Hoch-Risikotypen: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73 und 82 Niedrig-Risikotypen verursachen gutartige Genitalwarzen Niedrig-Risikotypen: 6, 11, 42, 43, 44 , 54 , , 70 , 72 und 81 Munoz N. et al., Against which human papillomavirus types shall we vaccinate and screen? The international perspective Int J Cancer 2004; 111: 278–85.

14
Übertragung HPV lebt in 400 nm Haut, nirgends sonst im Körper
Jeder ist infiziert (z.B. Hand- und Fußwarzen der Kindheit) Übertragung nur durch Hautkontakt von Mensch zu Mensch Menschen leben zusammen und brauchen „Hautkontakt“ zum Überleben HPV Infektion nur auf der Körperoberfläche – Keine Virämie , deshalb auch keine direkte AK-Induktion. D. Harper: HPV Today 7 (2005)
 Übertragung nur durch Hautkontakt von Mensch zu Mensch. Menschen leben zusammen und brauchen „Hautkontakt zum Überleben. HPV Infektion nur auf der Körperoberfläche – Keine Virämie , deshalb auch keine direkte AK-Induktion. D. Harper: HPV Today 7 (2005)")
15
Übertragung sexuell übertragen (inkl. Petting) Fragliche Übertragung:
Handtuch, Toilettensitz, Schwimmbad, u.a. Pädophiler Kontakt? Verminderung der Übertragbarkeit: Kondome? Beschneidung? Beschnittene (Muslime, Juden) übertragen offensichtlich weniger HPV beim Sexualverkehr , daher in diesen Regionen geringeres Vorkommen von CxCa. Übertragung durch Gegenstände ist eher nicht anzunehmen.
 übertragen offensichtlich weniger HPV beim Sexualverkehr , daher in diesen Regionen geringeres Vorkommen von CxCa. Übertragung durch Gegenstände ist eher nicht anzunehmen.")
16
Übertragungswege für HPV
Kontakt mit genitalen Schleimhäuten: Häufigster durch Geschlechtsverkehr übertragene Virus weltweit1,2 Perinatal3 Andere4 Schmierinfektion Digital Schutz vor HPV: Kein GV Monogamie Kondome (Winer, NEJM, 2006) Zircumzision (?) PapillomaViruses are most commonly transmitted through contact – either genital-genital, oral- genital, genital-anal or skin-to-skin.1 Furthermore, as there is a 10% cumulative incidence of PapillomaVirus infection in virgins, Winer et al established that non-penetrative sexual contact may be a plausible route of transmission.2 However, the use of condoms offers limited protection against the PapillomaVirus infection.3 Microabrasions occur on the epithelial surface allowing virions from the infected partner to gain access to the basal cell layer of the non-infected partners.4 During delivery, mothers with anogenital warts can transmit warts to their baby. Perinatal transmission of human PapillomaVirus from women with evidence of PapillomaVirus infection is approximately 2.8%.5 However, the risk of the child developing complications as a result of this exposure is estimated to be one to several hundred exposures.6 An uncommon consequence is neonatal laryngeal papillomatosis, usually caused by human PapillomaVirus type 6 or 11. There is also evidence of vertical (intrauterine) transmission of PapillomaViruses.4 Digital transmission of non-genital skin warts infrequently causes genital warts.2 PapillomaVirus DNA has been detected on bed control panels, light switches and colposcope handles in genitourinary medicine departments. The most likely route of contamination is directly from the physician’s gloved hands.7 PapillomaVirus DNA has also been detected in patient toilets (toilet flush handles, toilet seat and wash basin taps). The most likely route of contamination is directly from the patient.7 Although PapillomaViruses have been detected in a variety of hospital locations, it is not known if infections can be transmitted via these routes.7 Giles S. Transmission of HPV. CMAJ. 2003;168:1391 Winer RL, Lee S-K, Hughes JP et al. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students. Am J Epidemiol. 2003;157:218–226. Manhart LE and Koutsky LA. Do condoms prevent genital HPV infection, external genital warts or cervical neoplasia? Sex Transm Dis. 2002;29:725–735. Handsfield HH. Clinical presentation and natural course of anogenital warts. Am J Med ;102:16–20. Watts DH, Koutsky LA, Holmes KK et al. Low risk of perinatal transmission of human papillomavirus: results from a prospective cohort study. Am J Obstet Gynecol. 1999;180:774–775. Kawana K, Yasugi T, Yoshikawa H et al. Evidence for the presence of neutralising antibodies against human papillomavirus type 6 in infants born to mothers with condyloma acuminata. Am J Perinatol. 2003;20:11–15. Strauss S, Sastry P, Sonnex C et al. Contamination of environmental surfaces by genital papillomaviruses. Sex Transm Infect. 2002;78:135–138. 1. Winer et al. AJE. 2003;157:218– Giles CMAJ. 2003;168: Handsfield. Am J Med. 1997;102:16– Strauss et al Sex Trans Infect. 2002;78:135–138.
 Zircumzision ( ) PapillomaViruses are most commonly transmitted through contact – either genital-genital, oral- genital, genital-anal or skin-to-skin.1. Furthermore, as there is a 10% cumulative incidence of PapillomaVirus infection in virgins, Winer et al established that non-penetrative sexual contact may be a plausible route of transmission.2. However, the use of condoms offers limited protection against the PapillomaVirus infection.3. Microabrasions occur on the epithelial surface allowing virions from the infected partner to gain access to the basal cell layer of the non-infected partners.4. During delivery, mothers with anogenital warts can transmit warts to their baby. Perinatal transmission of human PapillomaVirus from women with evidence of PapillomaVirus infection is approximately 2.8%.5 However, the risk of the child developing complications as a result of this exposure is estimated to be one to several hundred exposures.6 An uncommon consequence is neonatal laryngeal papillomatosis, usually caused by human PapillomaVirus type 6 or 11. There is also evidence of vertical (intrauterine) transmission of PapillomaViruses.4. Digital transmission of non-genital skin warts infrequently causes genital warts.2. PapillomaVirus DNA has been detected on bed control panels, light switches and colposcope handles in genitourinary medicine departments. The most likely route of contamination is directly from the physician’s gloved hands.7. PapillomaVirus DNA has also been detected in patient toilets (toilet flush handles, toilet seat and wash basin taps). The most likely route of contamination is directly from the patient.7. Although PapillomaViruses have been detected in a variety of hospital locations, it is not known if infections can be transmitted via these routes.7. Giles S. Transmission of HPV. CMAJ. 2003;168:1391. Winer RL, Lee S-K, Hughes JP et al. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students. Am J Epidemiol. 2003;157:218–226. Manhart LE and Koutsky LA. Do condoms prevent genital HPV infection, external genital warts or cervical neoplasia Sex Transm Dis. 2002;29:725–735. Handsfield HH. Clinical presentation and natural course of anogenital warts. Am J Med. 1997;102:16–20. Watts DH, Koutsky LA, Holmes KK et al. Low risk of perinatal transmission of human papillomavirus: results from a prospective cohort study. Am J Obstet Gynecol. 1999;180:774–775. Kawana K, Yasugi T, Yoshikawa H et al. Evidence for the presence of neutralising antibodies against human papillomavirus type 6 in infants born to mothers with condyloma acuminata. Am J Perinatol. 2003;20:11–15. Strauss S, Sastry P, Sonnex C et al. Contamination of environmental surfaces by genital papillomaviruses. Sex Transm Infect. 2002;78:135– Winer et al. AJE. 2003;157:218– Giles CMAJ. 2003;168: Handsfield. Am J Med. 1997;102:16– Strauss et al Sex Trans Infect. 2002;78:135–138.")
17
Charakteristika der HPV Infektion des weiblichen Genitale
Lokale Infektion, keine systemische Ausbreitung Eintritt des Virus über Mikroläsionen Keine lokale entzündliche Reaktion Keine Zellyse Virusreplikation in Zellkernen Keine Übertragung von Zelle zu Zelle Persistenz in episomaler Form Latente Infektionen und lebenslange Virus-Persistenz Reinfektionen möglich

18
Natürlicher Verlauf HPV Infektion
Prävalenz stark abhängig vom Alter: % der Frauen im Alter zwischen 20 und 24 sind HPV positiv - bei Frauen über 35 liegt Prävalenz nur bei 4-10 % Bei 80% der Frauen heilt die symptomlose Infektion innerhalb von Mo aus Reinfektionen und Reaktivierung sind möglich

19
Von der HPV Infektion zur Karzinogenese
Voraussetzung für Karzinogenese: - Persistierende HPV Infektion - Integration der HPV DNA ins Wirtsgenom - Expression der Onkoproteine E6 und E7 LCR E7 E6 E1 L1 L2 E2 E4 E5 Disruption and integration point + – Integrated HPV DNA Host DNA Episomal HPV DNA Benign lesions In benign PapillomaVirus-associated skin lesions, the PapillomaVirus exists as a plasmid episome in the cell cytoplasm. It replicates separately, extrachromosomally.1 Lesions due to oncogenic PapillomaVirus In malignant PapillomaVirus-associated skin lesions, PapillomaVirus DNA integrates into the host cell’s chromosome through a break in the viral genome around the E1/E2 region.1 As a result of this break, the function of the E1 and E2 genes is lost. E2 is, therefore, no longer able to regulate expression of E6 and E7, resulting in cellular transformation.1 The E6 protein associates with the tumour suppressor protein, p53, and promotes proteolytic destruction of the protein. This leads to malignant transformation and loss of regulated cell growth.1 The E7 protein associates with the retinoblastoma protein (pRB), which inactivates the cell cycle restriction function of this protein.1 Viral load The average viral load may also be used to predict the frequency and extent of lesions in the cervix. Polymerase chain reaction quantification of PapillomaVirus viral load in a longitudinal study of 2,081 Brazilian women showed that the higher the number for viral copies per cell, the higher the risk of developing squamous intraepithelial lesions (SILs).2 Women with no lesions had, on average, 2.6 viral copies per cell.2 Women who had developed 3 or more SILs in the 6 years of follow up had, on average, 15.1 viral copies per cell.2 Syränen and Syränen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–51. Schlecht NF, Trevisan A, Duarte-Franco E et al. Viral load as a predictor of the risk of cervical intraepithelial neoplasia. Int J Cancer. 2003;103:519–524. Immortalisierung der Zellen, Genetische Instabilität, Aneuploidie Where E = Early; HPV = human PapillomaVirus; L = Late; LCR = Long Control Region; dotted yellow arrow = regulation. Adapted from 1. Phelps and Alexander. Ann Intern Med. 1995;123:368– Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46.
, which inactivates the cell cycle restriction function of this protein.1. Viral load. The average viral load may also be used to predict the frequency and extent of lesions in the cervix. Polymerase chain reaction quantification of PapillomaVirus viral load in a longitudinal study of 2,081 Brazilian women showed that the higher the number for viral copies per cell, the higher the risk of developing squamous intraepithelial lesions (SILs).2. Women with no lesions had, on average, 2.6 viral copies per cell.2. Women who had developed 3 or more SILs in the 6 years of follow up had, on average, 15.1 viral copies per cell.2. Syränen and Syränen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–51. Schlecht NF, Trevisan A, Duarte-Franco E et al. Viral load as a predictor of the risk of cervical intraepithelial neoplasia. Int J Cancer. 2003;103:519–524. Immortalisierung der Zellen, Genetische Instabilität, Aneuploidie. Where E = Early; HPV = human PapillomaVirus; L = Late; LCR = Long Control Region; dotted yellow arrow = regulation. Adapted from 1. Phelps and Alexander. Ann Intern Med. 1995;123:368– Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46.")
20
HPV Integration und Krebsrisiko: Funktion von E6
HPV wird in den Zellen gebildet Effekt E6 Genexpression wird von E2 kontrolliert Verlust der Kontrolle der E6 Expression Aktivität von p53 blockiert Verhinderung der Apoptose Zunahme der chromosomalen Instabilität Episomal E6 p53 AP E6 is a major transforming protein, capable of immortalising certain cell types.1 When the PapillomaVirus genome is episomal, the expression of the E6 genome and levels of the E6 protein, are controlled by the E2 protein.1 In malignant tumours, the PapillomaVirus genome is integrated into the host DNA.1 Integration regularly occurs within the viral E1–E2 region, thereby disrupting expression of the E2 gene. Expression of the E6 gene is no longer controlled.1 As a result of high levels of expression of E6, the protein forms complexes with other cellular proteins.1 E6 complexes with p53, a tumour suppressor protein, and AP (Associated Protein), resulting in the degradation of p53.1 The net result is a resistance to controlled cell death (apoptosis) and an increase in chromosome instability.2 Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46. Zur Hausen H. Papillomaviruses and cancer. From basic studies to clinical application. Nat Rev Cancer. 2002;2:342–350. Integration Wechselwirkung von E6 mit p53 und AP Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46.
, resulting in the degradation of p53.1. The net result is a resistance to controlled cell death (apoptosis) and an increase in chromosome instability.2. Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46. Zur Hausen H. Papillomaviruses and cancer. From basic studies to clinical application. Nat Rev Cancer. 2002;2:342–350. Integration. Wechselwirkung von E6 mit p53 und AP. Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46.")
21
HPV Integration und Krebsrisiko: Funktion von E7
HPV wird in den Zellen gebildet Effekt E7 Genexpression kontrolliert durch E2 Verlust der Kontrolle der E7 Expression Vervielfältigung des Chromosomensatzes Zelluläre Immortalisierung Tumorigenese Episomal E7 pRB E7 is a major transforming protein, capable of inducing cellular immortalisation and tumourigenesis.1 When the PapillomaVirus genome is episomal, the expression of E7 is tightly controlled by the E2 protein.1 Once the PapillomaVirus genome has integrated into the host DNA, function of the E2 gene is lost, and expression of the E7 gene is no longer controlled.1 With lack of control of expression, the levels of the E7 protein increase. The E7 protein complexes with other cellular proteins, such as the retinoblastoma protein (pRB).2 Association of E7 with pRB results in the dissociation of the pRB/E2F complex.1 Free E2F acts as a transcriptional activator, stimulating transcription of E2F-response genes. This propels the cell through the cell cycle.1 E7 also interacts with proteins p107 and p130, which would normally inhibit expression of pRB.1 Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46. Zur Hausen H. Papillomaviruses and cancer. From basic studies to clinical application. Nat Rev Cancer. 2002;2:342–350. + Integration E2F Freies Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46.
.2. Association of E7 with pRB results in the dissociation of the pRB/E2F complex.1. Free E2F acts as a transcriptional activator, stimulating transcription of E2F-response genes. This propels the cell through the cell cycle.1. E7 also interacts with proteins p107 and p130, which would normally inhibit expression of pRB.1. Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46. Zur Hausen H. Papillomaviruses and cancer. From basic studies to clinical application. Nat Rev Cancer. 2002;2:342– Integration. E2F. Freies. Syrjänen and Syrjänen. Papillomavirus infections in human pathology. Wiley & Sons, Chichester; p.11–46.")
22
Zeitlicher Ablauf der Karzinogenese
Innerhalb 1 Jahres Bis zu 5 Jahren > 10 Jahre Notwendiger Faktor KREBS NORMAL Schwere Dysplasie, Ca in situ Leichte/ mittlere Dysplasie HPV Infektion Sexualverhalten Hygiene Kondombenutzung Zircumzision Früher Sexualkontakt Multiple Partner Immunität Genetik Virale Faktoren Rauchen Geburtenzahl Pille? Ernährung? HIV Infektionen Kofaktoren

23
Prävalenz HPV-induzierter Erkrankungen
Geschätzte Anzahl von Erkrankungen/Jahr in Europa ~2,000 vulvar-vaginal cancers 33,400 invasive cervical cancer 15,000 women die each year (40 women/day or ~2/hour) ~30,000 pre-cancerous vulvar-vaginal lesions 163,000 severe pre-cancerous cervical lesions (CIN2/3) ~450 per day Low grade vulvar-vaginal lesions 554,000 low grade cervical lesions (CIN1) ~1,500 per day Cervix Vulva > 250,000 Genital warts Asymptomatische Infektion ~ 30 Mio/y
 ~30,000 pre-cancerous vulvar-vaginal lesions. 163,000 severe pre-cancerous cervical lesions (CIN2/3) ~450 per day. Low grade vulvar-vaginal lesions. 554,000 low grade cervical lesions. (CIN1) ~1,500 per day. Cervix. Vulva. > 250,000 Genital warts. Asymptomatische Infektion. ~ 30 Mio/y.")
24
Zusammenfassung: Ergebnisse der Grainge -Studie
Die Infektionsrate mit den onkogenen HPV-Typen 16 und 18 war in allen Altersgruppen vergleichbar. Die hohe Infektionsrate bei Frauen > 50 unterstützt die Notwendigkeit der Fortführung von Screeningprogrammen einer HPV- Impfung auch für ältere Frauen Grainge MJ et al. Emerg Infect Dis 2005;11:1680–5.

25
HPV Impfstoffe Merck (SPMSD) Impfstoff GSK Impfstoff
Dosis und Impfschema 0,5 ml; intramuskulär 0, 2, 6 Monate 0, 1, 6 Monate Impfstoff HPV- 6/ 11/ 16/ 18; VLP HPV-16 and HPV-18; VLP Herstellung Hefe Hi 5 (Baculovirus) Antigengehalt 20 µg HPV 6 40 µg HPV 11 40 µg HPV 16 20 µg HPV 18 20 µg HPV 16 Adjuvans 225 µg Al+++ AS04 (500µg Al µg MPL)
 Antigengehalt. 20 µg HPV µg HPV µg HPV µg HPV µg HPV 16. Adjuvans. 225 µg Al+++ AS04 (500µg Al µg MPL)")
26
Adjuvans Substanz, die in Verbindung mit einem Immunogen verabreicht, die Immunantwort auf dieses Immunogen verstärkt.

27
Phase II : Verbesserte Immunantwort mit dem Adjuvans AS04
700 * HPV 16/18 L1 Impfstoff mit AS04 600 HPV 16/18 L1 Impfstoff mit Aluminium Neutralisierende Antikörper, die über 4 Jahre in hoher Konzentration nachweisbar sind! 500 Anti-V5 (HPV-16) GMC (EU/ml) 400 * 300 * * 200 * 100 800 * 700 600 500 Anti-J4 (HPV-18) GMC (EU/ml) 400 * 300 * 200 * * 100 Month 3 Impfstoffdosen appliziert nach dem Impfschema 0,1,6 Monate * Statistically significant Giannini SL et al. AACR,Oct 30-Nov 2, 2005, Baltimore, USA.
 GMC (EU/ml) 400. * 300. * * 200. * * Anti-J4. (HPV-18) GMC (EU/ml) 400. * 300. * 200. * * Month. 3 Impfstoffdosen appliziert nach dem Impfschema 0,1,6 Monate. * Statistically significant. Giannini SL et al. AACR,Oct 30-Nov 2, 2005, Baltimore, USA.")
28
Antikörpertiter beim Vierfachimpfstoff
Koutsky & Harper, Vaccine 2006, Erweiterung: Olsen et al. Vaccine 2007.

29
Antikörpertiter beim Zweifachimpfstoff

30
HPV-001/-007-Studien: Hohe und lang anhaltende HPV-16 Antikörperkonzentrationen (bis zu 5,5 Jahren)
log (ELU/ml) 10000 100% Vakzine Anti-HPV-16 IgG 100% 1000 99.7% 99% 99% 100% 100% 99% 100% 98% > 11 fach höher 100 Natürliche Infektion 10 In the follow up study, up to 5,5 years, we observe the further “plateauing” of the serum antibody levels. At 63 to 64 months, the antibody levels in the vaccinated group were still at least 11 times higher than after natural infection. 6% 1 HPV-001 HPV-007 Monate Follow up Adapted from Presentation Gall S, AACR, Los Angeles, April 14-18, 2007.
 % Vakzine. Anti-HPV-16 IgG. 100% % 99% 99% 100% 100% 99% 100% 98% > 11 fach höher Natürliche. Infektion. 10. In the follow up study, up to 5,5 years, we observe the further plateauing of the serum antibody levels. At 63 to 64 months, the antibody levels in the vaccinated group were still at least 11 times higher than after natural infection. 6% HPV-001. HPV-007. Monate Follow up. Adapted from Presentation Gall S, AACR, Los Angeles, April 14-18,")
31
Sicherheit und Verträglichkeit
3.5 19 4.0 22 Serious Adverse Events insgesamt 0.0 Serious Adverse Events (SAEs), impfstoffbezogen 87.6 482 94.0 518 Lokalreaktionen ( Tage nach Impfung) 85.8 472 86.0 474 Allgemeinsymptome ( Tage nach Impfung) % n N=550 N=551 Plazebo Vakzine Probanden (ITT-Kohorte) Art der Symptome
, impfstoffbezogen Lokalreaktionen ( Tage nach Impfung) Allgemeinsymptome ( Tage nach Impfung) % n. N=550. N=551. Plazebo. Vakzine. Probanden (ITT-Kohorte) Art der Symptome.")
32
Immunogenität bei 15- bis 55-jährigen
10000 GMC (EU/ml) 15-25 26-35 36-45 46-55 1000 100 100% 100% 100% 100% 100% 100% 100% 100% 10 Vergleich der 3 Altersgruppen 26-35, 36-45, mit Gruppe jährigen. In höheren Altersgruppen ebenfalls 100%ige Serokonversion. 1 HPV 16 HPV 18 T. Schwarz; 42nd ASCO Annual Meeting, June 2-6, 2006, Atlanta.
 % 100% 100% 100% 100% 100% 100% 100% 10. Vergleich der 3 Altersgruppen 26-35, 36-45, mit Gruppe jährigen. In höheren Altersgruppen ebenfalls 100%ige Serokonversion. 1. HPV 16. HPV 18. T. Schwarz; 42nd ASCO Annual Meeting, June 2-6, 2006, Atlanta.")
33
Hinweise auf Kreuzprotektion
ITT-Kohorte; Nachbeobachtung bis zu 53 Monaten HPV 31 – antigenetisch mit HPV 16 verwandt HPV 45 – antigenetisch mit HPV 18 verwandt Kreuzprotektion gegenüber der Neuinfektion HPV 45: 1 Fall in der Impfgruppe, 17 Fälle in der Placebogruppe (94,2%) HPV 31: 14 Fälle in der Impfgruppe, 30 Fälle in der Placebogruppe (54,5%) Schutzwirkung gegen 4 der 7 häufigsten onkogenen HPV-Typen zu vermuten ! Harper D M et al. Lancet 2006; 367:
 HPV 31: 14 Fälle in der Impfgruppe, 30 Fälle in der. Placebogruppe (54,5%) Schutzwirkung gegen 4 der 7 häufigsten onkogenen HPV-Typen zu vermuten ! Harper D M et al. Lancet 2006; 367:")
34
HPV Impfstoffe Präventive Impfstoffe:
Serotypen Hersteller/Firma Entwicklungs-stand Tetravalenter L1 VLP (Gardasil) 6, 11,16, 18 Sanofi Pasteur MSD (Merck & Co.) Zugelassen in Europa, USA, Mexiko, Brasilien,Austral/Neuseeland Bivalenter L1 VLP (Cervarix) 16, 18 GSK/MedImmune Phase III Therapeutische Impfstoffe in der Entwicklung (z.T. Phase II Ergebnisse) Weitest fortgeschrittener Impfstoff Serotypen Hersteller/Firma Phase HspE7 1. Generation 16 StressGen II/III HspE7 2. Generation 16? Roche II ZYC101a Zycos MVA-HPV-IL2 (E6,E7) Transgene TA-HPV & TA-CIN 16/18 Xenova (deprioritized) The above list of vaccines under development is tentative. Preventative and therapeutic vaccines are in development for PapillomaVirus diseases. The preventative vaccines are the most advanced in the development process.
 6, 11,16, 18. Sanofi Pasteur MSD (Merck & Co.) Zugelassen in Europa, USA, Mexiko, Brasilien,Austral/Neuseeland. Bivalenter L1 VLP (Cervarix) 16, 18. GSK/MedImmune. Phase III. Therapeutische Impfstoffe in der Entwicklung (z.T. Phase II Ergebnisse) Weitest fortgeschrittener Impfstoff. Serotypen. Hersteller/Firma. Phase. HspE7 1. Generation. 16. StressGen. II/III. HspE7 2. Generation. 16 Roche. II. ZYC101a. Zycos. MVA-HPV-IL2 (E6,E7) Transgene. TA-HPV & TA-CIN. 16/18. Xenova (deprioritized) The above list of vaccines under development is tentative. Preventative and therapeutic vaccines are in development for PapillomaVirus diseases. The preventative vaccines are the most advanced in the development process.")
35
STIKO Auf Grund der positiven Ergebnisse aus klinischen Studien wurde die Impfung gegen HPV bereits als Regelimpfung in generelle Impfprogramme aufgenommen!!!

36
Impfkalender modifiziert nach der STIKO1 2007
Impfung gegen Vollendetes Lebensjahr² 9-17 ab 18 ≥60 Tetanus Diphtherie Pertussis Polio Auffrisch-Impfung (3) Masern, Mumps und Röteln Ggf. 1x MMR Windpocken Impfung (4,6) Hepatitis B Grundimmunisierung (7) 12-17 HPV Grundimmuni- sierung (10) Influenza Regelimpfung (8) Pneumokokken Regelimpfung (9) Grundimmunisierung HPV: Jahre 1 Modifiziert nach den Impfempfehlungen der Ständigen Impfkommission (STIKO) Stand Juli 2007, Quelle: Epi. Bull. 30/07, Robert Koch-Institut 2 Gleichbedeutend mit dem Beginn des folgenden Lebensjahrs 3 alle 10 Jahre eine Auffrischimpfung 4 versäumte Impfungen sollten möglichst bald nachgeholt werden 6 Ungeimpfte ohne durchgemachte Windpockenerkrankung, 1 Impfung bis zum 13 LJ, ab vollendeten 13. LJ 2 Impfungen 7 Grundimmunisierung für bisher nicht geimpfte Kinder und Jugendliche 8 Jährlich zu Beginn der Grippesaison 9 Auffrischung nach 6 Jahren (Erw.) 10 Epi Bull 30/2007
 Masern, Mumps und Röteln. Ggf. 1x MMR. Windpocken. Impfung. (4,6) Hepatitis B. Grundimmunisierung (7) HPV. Grundimmuni- sierung (10) Influenza. Regelimpfung (8) Pneumokokken. Regelimpfung (9) Grundimmunisierung HPV: Jahre. 1 Modifiziert nach den Impfempfehlungen der Ständigen Impfkommission (STIKO) Stand Juli 2007, Quelle: Epi. Bull. 30/07, Robert Koch-Institut. 2 Gleichbedeutend mit dem Beginn des folgenden Lebensjahrs. 3 alle 10 Jahre eine Auffrischimpfung. 4 versäumte Impfungen sollten möglichst bald nachgeholt werden. 6 Ungeimpfte ohne durchgemachte Windpockenerkrankung, 1 Impfung bis zum 13 LJ, ab vollendeten 13. LJ 2 Impfungen. 7 Grundimmunisierung für bisher nicht geimpfte Kinder und Jugendliche. 8 Jährlich zu Beginn der Grippesaison. 9 Auffrischung nach 6 Jahren (Erw.) 10 Epi Bull 30/2007.")
37
Empfehlungen der Ständigen Impfkommission vom 23. 03
Empfehlungen der Ständigen Impfkommission vom zur Impfung gegen HPV-16/18 Generelle Impfung für alle Mädchen im Alter von 12 bis 17 Jahren gegen HPV (Typ 16 und 18) Gefordert wird ein mit allen Arztgruppen abgestimmtes Impfprogramm, das die Gabe von 3 Dosen vor Beginn der sexuellen Aktivität sichert Frauen (>17 Jahre) können nach individueller Prüfung von Nutzen und Risiko der Impfung auf der Basis der Impfstoffzulassung geimpft werden Keine Änderung des Früherkennungsprogramms
 Gefordert wird ein mit allen Arztgruppen abgestimmtes Impfprogramm, das die Gabe von 3 Dosen vor Beginn der sexuellen Aktivität sichert. Frauen (>17 Jahre) können nach individueller Prüfung von Nutzen und Risiko der Impfung auf der Basis der Impfstoffzulassung geimpft werden. Keine Änderung des Früherkennungsprogramms.")
38
STIKO-Zielgruppe > 12-jährige Mädchen
Kinder- und Jugendärzte sehen die Mädchen oftmals nicht mehr Gynäkologen sehen die Mädchen noch nicht Mädchen-Sprechstunde Hausärzte sehen die Mädchen auch nicht, da sie selten krank sind??? Teilnahmerate an der J1: 35% Mit 17 Jahren besuchen 87% einen Frauenarzt bzw. -ärztin

39
Zusammenfassung wichtiger Erkenntnisse aus laufenden Studien
Langanhaltende Immunantwort (HPV-16 und HPV-18) bei Mädchen und Frauen im Alter von Jahren mit 100%iger Seropositivität bei HPV-16 und HPV-18 Transsudation von impfinduzierten, neutralisierenden Antikörpern in das zervikovaginale Sekret Höhere klinische Wirksamkeit als durch die eingesetzten Impfantigene zu erwarten (Kreuzprotektion: HPV-31, HPV-45) Sicherheitsprofil nach 5,5 Jahren unauffällig (keine Zunahme von AE, SAE oder NOCD) Keine Teratogenität bei akzidenzieller Impfung in der Schwangerschaft
 bei Mädchen und Frauen im Alter von Jahren mit 100%iger Seropositivität bei HPV-16 und HPV-18. Transsudation von impfinduzierten, neutralisierenden Antikörpern in das zervikovaginale Sekret. Höhere klinische Wirksamkeit als durch die eingesetzten Impfantigene zu erwarten (Kreuzprotektion: HPV-31, HPV-45) Sicherheitsprofil nach 5,5 Jahren unauffällig (keine Zunahme von AE, SAE oder NOCD) Keine Teratogenität bei akzidenzieller Impfung in der Schwangerschaft.")
40
Welche Fragen können wir inzwischen sicher beantworten?
HPV 6/11 bei Erstscreening bei 11,6% (Future) HPV 16/18 bei Erstscreening 21% (Future) Keine Antikörperbestimmung im Blut vor Impfung sinnvoll, da derzeit kein Test für die bereite Anwendung evaluiert ist und Impfeffekt nicht vom Serostatus sondern von Vorhandensein einer Infektion abhängig 8579 Frauen, die bei abgeschlossener Vakzinierung HPV-negativ waren – Effektivität der Impfung in Bezug HPV 16/18 CIN 2/3 99% (=1 Frau mit HPV 52 Persistenz) Bivalente Vakzine teilweise Kreuzprotektion gegen HPV 31 und 45 Bei HPV 16/18 vulvärer/vaginaler Dysplasie Schutz 100% Impfschutz bei Infektion während der Vakzinierung 98% HPV Vakzinierung kein therapeutischer Effekt (Hildesheim et al. JAMA 2007) Effektivität durch HPV16/18 Impfung in der Praevention aller HPV- assoziierten zerviaklen Dysplasien = 18% Krebsfrüherkennung weiterhin unerlässlich!!!!!!!!!
 HPV 16/18 bei Erstscreening 21% (Future) Keine Antikörperbestimmung im Blut vor Impfung sinnvoll, da derzeit kein Test für die bereite Anwendung evaluiert ist und Impfeffekt nicht vom Serostatus sondern von Vorhandensein einer Infektion abhängig Frauen, die bei abgeschlossener Vakzinierung HPV-negativ waren – Effektivität der Impfung in Bezug HPV 16/18 CIN 2/3 99% (=1 Frau mit HPV 52 Persistenz) Bivalente Vakzine teilweise Kreuzprotektion gegen HPV 31 und 45. Bei HPV 16/18 vulvärer/vaginaler Dysplasie Schutz 100% Impfschutz bei Infektion während der Vakzinierung 98% HPV Vakzinierung kein therapeutischer Effekt (Hildesheim et al. JAMA 2007) Effektivität durch HPV16/18 Impfung in der Praevention aller HPV- assoziierten zerviaklen Dysplasien = 18% Krebsfrüherkennung weiterhin unerlässlich!!!!!!!!!")
41
Welche Fragen können wir inzwischen sicher beantworten?
HPV-Impfstoffe sind immunogen und induzieren eine genotypen- spezifische Immunantwort. Die genotypen-spezifische Immunantwort korreliert mit Wirksamkeit bzw. Protektion vor HPV-Infektionen sowie HPV- assoziierten cervicovaginalen und vulvären Läsionen bei Mädchen/Frauen. Die Impfung bei Mädchen/Frauen mit bereits erfolgter Infektion (HPV-DNA-positiv, HPV-16/18-Antikörper-positiv) hat keine negativen Auswirkungen. Im Cervikovaginalsekret lassen sich vakzine-induzierte, neutralisierende Antikörper nachweisen. Das Sicherheitsprofil (Kurz- sowie Langzeit) beider Impfstoffe ist hervorragend.
 hat keine negativen Auswirkungen. Im Cervikovaginalsekret lassen sich vakzine-induzierte, neutralisierende Antikörper nachweisen. Das Sicherheitsprofil (Kurz- sowie Langzeit) beider Impfstoffe ist hervorragend.")
42
Fazit Es stehen zwei wirksame Impfprophylaxen zur Prävention von HPV-assoziierten zervikalen Läsionen sowie des Zervixkarzinoms zur Verfügung. Durch Implementierung eines Impfprogramms bei jungen Mädchen wird sich die Inzidenz dieser HPV- assoziierten Erkrankungen signifikant senken lassen.

43
Zusammenfassung: Junge Mädchen vor Sexualkontakt ( Jahre) stellen primäre Zielgruppe dar Eine Immunität von 10 Jahren wird angenommen Zeitpunkt einer erforderlichen Auffrischung ist bisher noch nicht klar Keine therapeutische Wirkung! Stellenwert der zytologischen Vorsorge!

44
ESGO Statement on HPV vaccination
There is no indication that vaccination will have any effect on existing Pap test abnormalities or after treatment of already established dysplasia.

45
ESGO Statement on HPV vaccination
Finally and most importantly, the ESGO perceives the greatest opportunity and benefit for the vaccine being in areas of the world where cervical screening has not been available or feasible. The society urges national and international agencies and the companies who have developed the vaccines to give priority to their introduction in the areas of the world where they are most badly needed and have the potential to prevent suffering and save millions of lives.

Ähnliche Präsentationen






 Ein Wirksamkeitsvergleich von zeitlich begrenzter.>")


 soll anhand der Geschichte von Edward Jenners Impfmethode erläutert werden: Eine der großen Seuchen.>")









