Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Multimodale Diagnostik und Therapie des hepatozellulären Karzinoms : HCC
Prof. Dr. med. M. P. Manns Klinik für Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover

2
HCC: Multimodal und Interdisziplinär
Klinik für Gastroenterologie, Hepatologie und Endokrinologie Klinik für Allgemein-, Viszeral- und Transplantationschirurgie Klinik für Haematologie, Haemostaseologie, int. Onkologie und Stammzelltransplantation Institut für diagnostische Radiologie Klinik für Strahlentherapie

3
DFG-KliFo 119: „Molekular Basis and Therapeutic Concepts in HCC“
Chair: M.P. Manns; Director: S. Kubicka Institut für Pathologie Prof. Dr. H. Kreipe Dr. P. Flemming PD Dr. U.Lehmann Institut für Zell- und Molekularpathologie Prof. Dr. B.Schlegelberger PD Dr. L. Wilkens Institut für Molekularbiologie Prof. Dr. A. Gossler Dr. N. Malek GBF Braunschweig PD Dr. J. Bruder Klinik für Gastroenterologie, Hepatologie u. Endokrinologie Prof. Dr. M. Manns Prof. Dr. S. Kubicka Prof. Dr. C. Strassburg Prof. Dr. L. Rudolph(Ulm) PD. Dr. N. Malek Prof. Dr. T. Greten Dr. A. Vogel Abt. Hämatologie/Onkologie (assoziiert) Prof. Dr. A. Ganser Dr. V. Grünwald
 PD. Dr. N. Malek Prof. Dr. T. Greten. Dr. A. Vogel. Abt. Hämatologie/Onkologie. (assoziiert) Prof. Dr. A. Ganser. Dr. V. Grünwald.")
4
Maligne Lebertumore Metastasen Lebereigene Karzinome
Hepatozelluläres Karzinom Cholangiokarzinom

5
Weltweite Inzidenz des HCC im Jahr 2000
Inzidenz weltweit. Hohe Inzidenz in Asien und Afrika, aber andere Pathogenese. Alters angepasste Inzidenz / Männer

6
80s' 90s' 2,3 USA 7,0 7,5 France 10,2 4,8 Italy 10,9 19,0 Japan 40,0
Death rate per 100,000 H. El Serag et al. NEJM 1999 Kiyosawa K, Jpn J Inf Dis 2002

7
Zunahme des HCC in Deutschland
Daten aus dem Tumorregister des Saaralnds Prof. Dr. med. M. P. Manns Klinik für Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover

8
Häufigste Krebssterbefälle in Niedersachsen (2001)
Leber Mund und Rachen Leukämie Ösophagus Harnblase Niere Pankreas Magen Prostata Darm Lunge Daten von Niedersächsischen Krebsregister. CCC und HCC sind hier nicht getrennt aufgeführt. 5 10 15 20 25 30 Epidemiologisches Krebsregister Niedersachsen, Dezember 2004

9
Zunahme der HCC Sterblichkeit
Daten stammen vom italienischen Krebsregister und zeigen die Abnahme der Zirrhose bedingten Sterblichkeit und gleichzeitige Zunahme des HCC. Prof. Dr. med. M. P. Manns Abteilung Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover

10
% aller ersten Komplikationen
Häufigkeiten der Hauptkomplikationen bei initial kompensierter HCV-Zirrhose HCC 16 Aszites 7 Ikterus 3 Blutende Varizen 2,5 Enzephalopathie 0,4 5 10 15 20 % aller ersten Komplikationen Benvegnù et al, 2000 Prof. Dr. med. M. P. Manns Abteilung Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover

11
Wandel der Komplikationen der Leberzirrhose
, 90er ,

12
Wandel der Komplikationen der Leberzirrhose
, 80er , 2006 Aufgrund der Verbesserung in der Therapie des Aszites TIPSS und der Varizen (Sklerosierung und TIPSS) stellen diese nicht mehr das Hauptproblem der Zirrhose dar, sondern zunehmend das HCC.
 stellen diese nicht mehr das Hauptproblem der Zirrhose dar, sondern zunehmend das HCC.")
13
Risikofaktoren für die Entstehung eines HCC
chronische HBV + HCV Infektion Alkohol Aflatoxine Hämochromatose Übergewicht/Diabetes (NASH) Leberzirrhose
 Leberzirrhose.")
14
HBe-Ag Serokonversion and HCC
Cumulative HCC Incidence [%] Jahre Years Yang HI, et al. N Engl J Med 2002

15
Risk of HCC across a Biological Gradient of Serum HBV Virus DNA Level
Baseline HBV DNA Level copies/mL 14 ≥ 1 Mio 12 10 Cumulative Incidence of HCC [%] 8 6 4 2 < 300 Year of Follow Up Chen et al. JAMA 2006

16
Nucleosid Treatment reduces the risk of HCC in patients with chronic HBV infection
Liaw NEJM 2004

17
HCV-Prävalenz in Deutschland (Bundes-Gesundheitssurvey 1997-1998)
Bevölkerungsstichprobe (18-79 J.) n = 6.748 Durchseuchung (anti-HCV) 0,4% Virusträger (HCV-PCR positiv) % Ausschluss von Personen aus - Krankenhäusern, Pflegeheimen etc. - Justizvollzugsanstalten iv Drogenkonsumenten unterrepräsentiert Schätzung Virusträger Palitzsch et al. 1999
 n = Durchseuchung (anti-HCV) 0,4% Virusträger (HCV-PCR positiv) 84% Ausschluss von Personen aus. - Krankenhäusern, Pflegeheimen etc. - Justizvollzugsanstalten. iv Drogenkonsumenten unterrepräsentiert. Schätzung Virusträger. Palitzsch et al")
18
Anteil der viralen Hepatitis am HCC
Anzahl der HCC Sterbefälle 1980 1994 1992 1990 1988 1986 1984 1982 1996 1998 8.000 7.000 6.000 5.000 4.000 3.000 2.000 1.000 keine Lebererkrankung andere Lebererkrankung Virale Hepatitis alkoholische Lebererkrankung Number of HCC deaths by identifiable coexistent liver disease by year (1980–1998). (Daten aus den USA) Background & Aims: The incidence of hepatocellular carcinoma (HCC) has been increasing in the United States. Although resource-intensive treatment modalities have been increasingly applied, these patients still have poor survival. We examined 2 nationally representative databases, the Multiple Cause of Death file and the Nationwide Inpatient Sample database, to examine trends in mortality and hospital service utilization related to HCC. Methods: In both databases, a priori criteria were used to identify cases of HCC. All other available diagnostic fields were examined to characterize coexistent liver disease. Age-, sex-, and race-specific mortality from HCC was calculated, and temporal changes in mortality rates were evaluated using the multivariable Poisson model. Hospital service utilization was estimated based on length of stay, total hospitalization charges, and principal procedures. Results: The age-, sex-, and race-specific mortality from HCC increased from 1.54 to 2.58 per 100,000 per year between 1980 and Male sex, African and Asian race, and increasing age were also associated with higher mortality. The estimated total charge for HCC hospitalizations nationwide increased from $241 million in 1988 to $509 million in 2000 after inflation adjustment. Commonly employed procedures in 2000 included ngiography/embolization, resection, local ablative therapy, and liver transplantation. Conclusions: In the recent past, mortality and hospital service utilization related to HCC increased substantially. Closer epidemiologic surveillance to understand causation of HCC at the population level and to help implement primary and secondary prevention is urgently arranted. Gastroenterology (2005)
. (Daten aus den USA) Background & Aims: The incidence of hepatocellular carcinoma (HCC) has been increasing in the United States. Although resource-intensive treatment modalities have been increasingly applied, these patients still have poor survival. We examined 2 nationally representative databases, the Multiple Cause of Death file and the Nationwide Inpatient Sample database, to examine trends in mortality and hospital service utilization related to HCC. Methods: In both databases, a priori criteria were used to identify cases of HCC. All other available diagnostic fields were examined to characterize coexistent liver disease. Age-, sex-, and race-specific mortality from HCC was calculated, and temporal changes in mortality rates were evaluated using the multivariable Poisson model. Hospital service utilization was estimated based on length of stay, total hospitalization charges, and principal procedures. Results: The age-, sex-, and race-specific mortality from HCC increased from 1.54 to 2.58 per 100,000 per year between 1980 and Male sex, African and Asian race, and increasing age were also associated with higher mortality. The estimated total charge for HCC hospitalizations nationwide increased from $241 million in 1988 to $509 million in 2000 after inflation adjustment. Commonly employed procedures in 2000 included ngiography/embolization, resection, local ablative therapy, and liver transplantation. Conclusions: In the recent past, mortality and hospital service utilization related to HCC increased substantially. Closer epidemiologic surveillance to understand causation of HCC at the population level and to help implement primary and secondary prevention is urgently arranted. Gastroenterology (2005)")
19
Cumulatives Risiko bei HCV induzierter Zirrhose am Beispiel von 183 Patienten mit HCV induzierter Leberzirrhose Carcinogenesis rate Background/Aims: To estimate hepatocarcinogenesis rates in patients with hepatitis C virus (HCV)-related cirrhosis, an accurate prediction table was created. Methods: A total of 183 patients between 1974 and 1990 were assessed for carcinogenesis rate and risk factors. Predicted carcinogenesis rates were validated using a cohort from the same hospital between 1991 and 2003 (nZ302) and an external cohort from Tokyo National Hospital between 1975 and 2002 (nZ205). Results: The carcinogenesis rates in the primary cohort were 28.9% at the 5th year and 54.0% at the 10th year. A proportional hazard model identified alpha-fetoprotein (R20 ng/ml, hazard ratio 2.30, 95% confidence interval 1.55–3.42), age (R55 years, 2.02, 95% CI 1.32–3.08), gender (male, 1.58, 95% CI 1.05–2.38), and platelet count (!100,000 counts/mm3, 1.54, 95% CI 1.04–2.28) as independently associated with carcinogenesis. When carcinogenesis rates were simulated in 16 conditions according to four binary variables, the 5th- and 10th-year rates varied from 9 to 64%, and 21–93%, respectively. Actual carcinogenesis rates in the internal and external validation cohorts were similar to those of the simulated curves. Conclusions: Simulated carcinogenesis rates were applicable to patients with HCV-related cirrhosis. Since, hepatocarcinogenesis rates markedly varied among patients depending on background features, we should consider stratifying them for cancer screening and cancer prevention programs. Ikeda J Hepatol 2006
-related cirrhosis, an accurate prediction table was created. Methods: A total of 183 patients between 1974 and 1990 were assessed for carcinogenesis rate and risk factors. Predicted carcinogenesis rates were validated using a cohort from the same hospital between 1991 and 2003 (nZ302) and an external cohort from Tokyo National Hospital between 1975 and 2002 (nZ205). Results: The carcinogenesis rates in the primary cohort were 28.9% at the 5th year and 54.0% at the 10th year. A proportional hazard model identified alpha-fetoprotein (R20 ng/ml, hazard ratio 2.30, 95% confidence interval 1.55–3.42), age (R55 years, 2.02, 95% CI 1.32–3.08), gender (male, 1.58, 95% CI 1.05–2.38), and platelet count (!100,000 counts/mm3, 1.54, 95% CI 1.04–2.28) as independently associated with carcinogenesis. When carcinogenesis rates were simulated in 16 conditions according to four binary variables, the 5th- and 10th-year rates varied from 9 to 64%, and 21–93%, respectively. Actual carcinogenesis rates in the internal and external validation cohorts were similar to those of the simulated curves. Conclusions: Simulated carcinogenesis rates were applicable to patients with HCV-related cirrhosis. Since, hepatocarcinogenesis rates markedly varied among patients depending on background features, we should consider stratifying them for cancer screening and cancer prevention programs. Ikeda J Hepatol")
20
Männliches Geschlecht Alter > 55 Jahre
Risikofaktoren für die Entstehung eines HCC bei chronischer HCV Infektion und Leberzirrhose AFP > 20 ng/ml Männliches Geschlecht Alter > 55 Jahre Thrombopenie < Tsd./mm3 Ikeda J Hepatol 2006

21
HCC - Ursachen (MHH 1998 - 2003, 396 Patienten)
Other 8 % HBV 21 % Eigene Daten toxic 41 % HCV 28 % HBV + HCV 3 % Greten et al Br J Can 2005

22
Incidence of HCC [rate per 100,000]
HCC-Inzidenz bei Kindern in Taiwan: Hepatitis B-Impfung verhindert Leberkrebs! 0,9 0,8 0,7 0,6 Incidence of HCC [rate per 100,000] 0,5 0,4 0,3 0,2 0,1 1981 1983 1985 1987 1989 1991 1993 Chang et al, NEJM 1997
![Incidence of HCC [rate per 100,000]](http://slideplayer.org/slide/638067/1/images/22/Incidence+of+HCC+%5Brate+per+100%2C000%5D.jpg "HCC-Inzidenz bei Kindern in Taiwan: Hepatitis B-Impfung verhindert Leberkrebs! 0,9. 0,8. 0,7. 0,6. Incidence of HCC [rate per 100,000] 0,5. 0,4. 0,3. 0,2. 0, Chang et al, NEJM")
23
Anteil gegen Hepatitis B geimpfter Kinder
bei Einschulung, (Stand: September 2004) vollständig begonnen % der Kinder mit vorliegendem Impfausweis Quelle: RKI
 vollständig. begonnen. % der Kinder mit vorliegendem Impfausweis. Quelle: RKI.")
24
Möglichkeiten der HCC Prävention
Greten, Wedemeyer, Manns Deutsches Ärzteblatt 2006

25
Risikofaktoren für die Entstehung eines HCC
chronische HBV + HCV Infektion Alkohol Aflatoxine Hämochromatose Übergewicht/Diabetes (NASH) Leberzirrhose
 Leberzirrhose.")
26
Kumulative Inzidenz für ein HCC [%]
Geschätztes HCC Risiko 30 20 HCV Kumulative Inzidenz für ein HCC [%] HBV 10 Alkohol 1 2 3 4 5 Jahre Greten, Wedemeyer, Manns Deutsches Ärzteblatt in press Prof. Dr. med. M. P. Manns Abteilung Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover
![Kumulative Inzidenz für ein HCC [%]](http://slideplayer.org/slide/638067/1/images/26/Kumulative+Inzidenz+f%C3%BCr+ein+HCC+%5B%25%5D.jpg "Geschätztes HCC Risiko HCV. Kumulative Inzidenz für ein HCC [%] HBV. 10. Alkohol Jahre. Greten, Wedemeyer, Manns Deutsches Ärzteblatt in press. Prof. Dr. med. M. P. Manns. Abteilung Gastroenterologie, Hepatologie und Endokrinologie. Medizinische Hochschule Hannover.")
27
Kumulative Inzidenz für ein HCC [%]
Geschätztes HCC Risiko 30 HCV + Alkohol 20 HCV Kumulative Inzidenz für ein HCC [%] HBV 10 Alkohol 1 2 3 4 5 Jahre Greten, Wedemeyer, Manns Deutsches Ärzteblatt in press Prof. Dr. med. M. P. Manns Abteilung Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover
![Kumulative Inzidenz für ein HCC [%]](http://slideplayer.org/slide/638067/1/images/27/Kumulative+Inzidenz+f%C3%BCr+ein+HCC+%5B%25%5D.jpg "Geschätztes HCC Risiko. 30. HCV + Alkohol. 20. HCV. Kumulative Inzidenz für ein HCC [%] HBV. 10. Alkohol Jahre. Greten, Wedemeyer, Manns Deutsches Ärzteblatt in press. Prof. Dr. med. M. P. Manns. Abteilung Gastroenterologie, Hepatologie und Endokrinologie. Medizinische Hochschule Hannover.")
28
HCC Risikofaktoren Gesamtbevölkerung Hepatozelluläres Karzinom HBV
Diabetes HCV Alkohol Hepatozelluläres Karzinom More than 18 million adults in the United States abusealcohol, a prevalence 5 times higher than that of hepatitisC. Chronic alcohol use of greater than 80 g/day for more than 10 years increases the risk for hepatocellular carcinoma(HCC) approximately 5-fold; alcohol use of less than 80 g/day is associated with a nonsignificant increased risk for HCC. The risk for HCC in decompensated alcoholinduced cirrhosis approaches 1% per year. The risk does not decrease with abstinence, and HCC can occur in a noncirrhotic liver. Alcohol use in chronic hepatitis C doubles the risk for HCC as compared with the risk in hepatitis C alone. Furthermore, there may be synergism between alcohol and hepatitis C in the development of HCC, and in these patients HCC may occur at an earlier age and the HCC may be histologically more advanced. Studies in the United States and Italy suggest that alcohol is the most common cause of HCC (accounting for 32%–45% of HCC). The mechanisms by which alcohol causes HCC are incompletely understood, but may include chromosomal loss, oxidative stress, a decreased retinoic acid level in the liver, altered DNA methylation, and genetic susceptibility. Alcohol use is increasing in many countries, suggesting that alcohol will continue to be a common cause of HCC throughout the world. USA 16 % 22 % 32 % 20 % Italien 22 % 36 % 45 % Morgan Gastroenterology 2004 Prof. Dr. med. M. P. Manns Abteilung Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover
 approximately 5-fold; alcohol use of less than 80 g/day is associated with a nonsignificant increased risk. for HCC. The risk for HCC in decompensated alcoholinduced cirrhosis approaches 1% per year. The risk does not decrease with abstinence, and HCC can occur in a noncirrhotic liver. Alcohol use in chronic hepatitis C doubles the risk for HCC as compared with the risk in hepatitis C alone. Furthermore, there may be synergism between alcohol and hepatitis C in the development of HCC, and in these patients HCC may occur at an earlier age and the HCC may be histologically more advanced. Studies in the United States and Italy suggest that alcohol is the most common cause of HCC (accounting for 32%–45% of HCC). The mechanisms by which alcohol causes HCC are incompletely understood, but may include chromosomal loss, oxidative stress, a decreased retinoic acid level in the liver, altered DNA methylation, and genetic susceptibility. Alcohol use is increasing in many countries, suggesting that alcohol will continue to be a common cause of HCC throughout the world. USA. 16 % 22 % 32 % 20 % Italien. 22 % 36 % 45 % Morgan Gastroenterology Prof. Dr. med. M. P. Manns. Abteilung Gastroenterologie, Hepatologie und Endokrinologie. Medizinische Hochschule Hannover.")
29
Risikofaktoren für die Entstehung eines HCC
chronische HBV + HCV Infektion Alkohol Aflatoxine Hämochromatose Übergewicht/Diabetes (NASH) Leberzirrhose
 Leberzirrhose.")
30
Karzinomrisko für Männer mit einem
BMI ≥ 35 kg/m2 Calle NEJM 2003

31
Diabetes und HCC Chronic non-alcoholic HCC liver diseases
Follow up (Years) Cumulative Incidence HCC Chronic non-alcoholic liver diseases No Diabetes Diabetes Background & Aims: An association between diabetes and chronic liver disease has been reported. However, the temporal relationship between these conditions remains unknown. Methods: We identified all patients with a hospital discharge diagnosis of diabetes between 1985 and 1990 using the computerized records of the Department of Veterans Affairs. We randomly assigned 3 patients without diabetes for every patient with diabetes. We excluded patients with concomitant liver disease. The remaining cohort was followed through 2000 for the occurrence of chronic nonalcoholic liver disease (CNLD) and hepatocellular carcinoma (HCC). Hazard rate ratios (HRR) were determined in Cox proportional hazard survival analysis. Results: The study cohort comprised 173,643 patients with diabetes and 650,620 patients without diabetes. Most were men (98%). Patients with diabetes were older (62 vs. 54 years) than patients without diabetes. The incidence of chronic nonalcoholic liver disease was significantly higher among patients with diabetes (incidence rate: vs per 10,000 person-years, respectively, P < ). Similar results were obtained for HCC (incidence rate: 2.39 vs per 10,000 person-years, respectively, P < ). Diabetes was associated with an HRR of 1.98 (95% CI: 1.88 to 2.09, P < ) of CNLD and an HRR of 2.16 (1.86 to 2.52, P < ) of hepatocellular carcinoma. Diabetes carried the highest risk among patients with longer than 10 years of follow-up. Conclusions: Among men with diabetes, the risk of CNLD and HCC is doubled. This increase in risk is independent of alcoholic liver disease, viral hepatitis, or demographic features. El-Serag Gastroenterology 2004 Prof. Dr. med. M. P. Manns Abteilung Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover
 Cumulative Incidence. HCC. Chronic non-alcoholic. liver diseases. No Diabetes. Diabetes. Background & Aims: An association between diabetes. and chronic liver disease has been reported. However, the temporal relationship between these conditions remains. unknown. Methods: We identified all patients. with a hospital discharge diagnosis of diabetes between and 1990 using the computerized records of the. Department of Veterans Affairs. We randomly assigned. 3 patients without diabetes for every patient with diabetes. We excluded patients with concomitant liver disease. The remaining cohort was followed through for the occurrence of chronic nonalcoholic liver disease. (CNLD) and hepatocellular carcinoma (HCC). Hazard rate. ratios (HRR) were determined in Cox proportional hazard. survival analysis. Results: The study cohort comprised. 173,643 patients with diabetes and 650,620 patients. without diabetes. Most were men (98%). Patients with. diabetes were older (62 vs. 54 years) than patients. without diabetes. The incidence of chronic nonalcoholic. liver disease was significantly higher among patients. with diabetes (incidence rate: vs per 10,000. person-years, respectively, P < ). Similar results. were obtained for HCC (incidence rate: 2.39 vs per. 10,000 person-years, respectively, P < ). Diabetes. was associated with an HRR of 1.98 (95% CI: 1.88 to. 2.09, P < ) of CNLD and an HRR of 2.16 (1.86 to. 2.52, P < ) of hepatocellular carcinoma. Diabetes. carried the highest risk among patients with longer. than 10 years of follow-up. Conclusions: Among men. with diabetes, the risk of CNLD and HCC is doubled. This. increase in risk is independent of alcoholic liver disease, viral hepatitis, or demographic features. El-Serag Gastroenterology Prof. Dr. med. M. P. Manns. Abteilung Gastroenterologie, Hepatologie und Endokrinologie. Medizinische Hochschule Hannover.")
32
Volkskrankheit NASH Steatosis: Ca. 20.000.000 Menschen in Deutschland!
Natürlicher Verlauf NAFLD – „pur fat“ Volkskrankheit NASH Steatosis: Ca Menschen in Deutschland! 10% / 10 Jahre NASH 10% / 10 Jahre Leberzirrhose 10%-20% / 10 Jahre HCC

33
Risikofaktoren Europa + US Japan Afrika + Asien HBV 22 (4-58)
20 (18-44) 60 (40-90) HCV 60 (12-72) 63 (48-94) 20 (9-56) Alkohol 45 (8-57) 2 (15-33) 0 (11-41) Nikotin 12 (0-14) 40 (9-51) 22) Kontrazeptiva 0 (10-50) - 8 Aflatoxine kaum häufig andere < 5 - Bosch Gastroenterology 2004
 60 (40-90) HCV. 60 (12-72) 63 (48-94) 20 (9-56) Alkohol. 45 (8-57) 2 (15-33) 0 (11-41) Nikotin. 12 (0-14) 40 (9-51) 22) Kontrazeptiva. 0 (10-50) - 8. Aflatoxine. kaum. häufig. andere. < 5. - Bosch Gastroenterology")
34
Risikofaktoren für ein HCC
Leberzirrhose ohne mit HBV +++ +++ HCV ++ +++ Hämochromatose +++ PBC / PSC / M. Wilson + AIH ++ BMI ≥ 35 kg/m2 + Alkohol ++ Rauchen + Aflatoxin +++ Prof. Dr. med. M. P. Manns Abteilung Gastroenterologie, Hepatologie und Endokrinologie Medizinische Hochschule Hannover

35
Influence of Coffee Drinking on Subsequent Risk of HCC:
Coffee consumption reduces the risk of HCC independently of its etiology J. Hepatol. (2005) 42: 528 Influence of Coffee Drinking on Subsequent Risk of HCC: A prospective study in Japan J. Natl. Cancer Inst. (2005) 97:293 Mehrere unabhängige Studien zeigen den protektiven Wert von Kaffee in Bezug auf das HCC. Ähnliches gilt auch für das Colon-Ca Ösophagus Ca etc. Der genaue Mechanismus ist unbekannt.
 42: 528. Influence of Coffee Drinking on Subsequent Risk of HCC: A prospective study in Japan. J. Natl. Cancer Inst. (2005) 97:293. Mehrere unabhängige Studien zeigen den protektiven Wert von Kaffee in Bezug auf das HCC. Ähnliches gilt auch für das Colon-Ca Ösophagus Ca etc. Der genaue Mechanismus ist unbekannt.")
36
Influence of Coffee Drinking on Subsequent Risk of HCC:
Coffee consumption reduces the risk of HCC independently of its etiology J. Hepatol. (2005) 42: 528 Influence of Coffee Drinking on Subsequent Risk of HCC: A prospective study in Japan J. Natl. Cancer Inst. (2005) 97:293 Oben die tatsächlichen Daten
 42: 528. Influence of Coffee Drinking on Subsequent Risk of HCC: A prospective study in Japan. J. Natl. Cancer Inst. (2005) 97:293. Oben die tatsächlichen Daten.")
37
Mass on surveillance ultrasound in a cirrhotic liver
< 1 cm Repeated US at 3-4 months intervals Stable over 18- 24 months Enlarging Return to standard surveillance protocol (6-12 monthly) Proceed according to lesion size
 Proceed. according to. lesion size.")
38
Treat as hepatocellular carcinoma
Mass on surveillance ultrasound in a cirrhotic liver < 1 cm 1 - 2 cm Repeated US at 3-4 months intervals Two dynamic imaging studies Coincidental typical vascular pattern on dynamic imaging Typical vascular pattern with one technique Atypical vascular pattern with both techniques Biopsy Stable over 18- 24 months Enlarging Diagnostic of HCC Non diagnostic Other diagnosis Return to standard surveillance protocol (6-12 monthly) Proceed according to lesion size Treat as hepatocellular carcinoma
 Proceed. according to. lesion size. Treat as hepatocellular carcinoma.")
39
Treat as hepatocellular carcinoma
Mass on surveillance ultrasound in a cirrhotic liver < 1 cm 1 - 2 cm Repeated US at 3-4 months intervals Two dynamic imaging studies Coincidental typical vascular pattern on dynamic imaging Typical vascular pattern with one technique Atypical vascular pattern with both techniques Biopsy Stable over 18- 24 months Enlarging Diagnostic of HCC Non diagnostic Other diagnosis Repeat biopsy or Imaging follow-up Return to standard surveillance protocol (6-12 monthly) Change in size/profile Proceed according to lesion size Repeat imaging and/or biopsy Positive Negative Treat as hepatocellular carcinoma
 Change in size/profile. Proceed. according to. lesion size. Repeat imaging. and/or biopsy. Positive. Negative. Treat as hepatocellular carcinoma.")
40
Treat as hepatocellular carcinoma
Mass on surveillance ultrasound in a cirrhotic liver < 1 cm 1 - 2 cm > 2 cm Repeated US at 3-4 months intervals Two dynamic imaging studies One dynamic imaging studies Typical vascular pattern on dynamic Imaging or AFP > 200 ng/ml Coincidental typical vascular pattern on dynamic imaging Typical vascular pattern with one technique Atypical vascular pattern with both techniques Atypical vascular pattern Biopsy Stable over 18- 24 months Enlarging Diagnostic of HCC Non diagnostic Other diagnosis Repeat biopsy or Imaging follow-up Return to standard surveillance protocol (6-12 monthly) Change in size/profile Proceed according to lesion size Repeat imaging and/or biopsy Positive Negative Treat as hepatocellular carcinoma
 Change in size/profile. Proceed. according to. lesion size. Repeat imaging. and/or biopsy. Positive. Negative. Treat as hepatocellular carcinoma.")
41
Staging des hepatozellulären Karzinoms
System Performance Status Hepatic Function AFP Tumor Staging Okuda Ascites, Alb., Bili No No >50% of cross-sectional area TNM No No No Number of nodes, Size, PVT Number of nodes, </>50% of liver, PVT CLIP CTP < / > 400 ng/ml No Number of nodes, size, PVT, Mets BCLC CTP No No CUPI Ascites, Bili, AP < / > 500 ng/ml Symptoms TNM JIS CTP No No TNM GRETCH Bili, AP < / > 35 ng/ml Yes PVT

42
Therapie des HCC

43
Therapiealgorithmus HCC Resektion LTx (CLT/LDLT) PEI / RF TACE new
PST 0, Child-Pugh A PST 0-2, Child-Pugh A-B PST >2, Child-Pugh C Very Early Stage Single ≤ 2 cm Early Stage Single or 3 nodules ≤ 3cm, PS 0 Intermediate Stage (B) Multinodular, PS 0 Advanced Stage Portal invasion, N1,M1, PS 1-2 Terminal Stage Single 3 nodules ≤3 cm PVP / bilirubin Increased Associated disease Portal invasion, N1,M1 Normal No Yes No Yes Resektion LTx (CLT/LDLT) PEI / RF TACE new Agents BSC Curativer Treatment RCT AASLD Guidelines 2005
 Multinodular, PS 0. Advanced Stage. Portal invasion, N1,M1, PS 1-2. Terminal. Stage. Single. 3 nodules ≤3 cm. PVP / bilirubin. Increased. Associated disease. Portal invasion, N1,M1. Normal. No. Yes. No. Yes. Resektion. LTx. (CLT/LDLT) PEI / RF. TACE. new. Agents. BSC. Curativer Treatment. RCT. AASLD Guidelines")
44
Bismuth et al., Ann Surg. 218:145-51, 1993
Liver resection versus transplantation for hepatocellular carcinoma in cirrhotic patients Bismuth et al., Ann Surg. 218:145-51, 1993 3 y OS 3 y RFS All Resection 50% 27% Transplantation 47% 46% 1-2 Nodules < 3cm Resection 18% Transplantation 83% p<0.05 p<0.001 LTX ist gerade für kleine HCCs in fortgeschrittener Leberzirrhose günstiger als die Resektion, da die „prämaligne Leberzirrhose“ durch die LTX entfernt wird

45
Liver transplantation: first series of cirrhotic patients with HCC
Authors N Tumor stage Rec 3y 5y Ringe et al. % > 5cm - 15% 15% Iwatsuki et al 35% portal invasion % multinodular 43% 39% 38% Bismuth et al. 50% symptomatic % > 3 nodules 54% 49% - Moreno et al. 25% portal invasion % T4 32% 67% 48%

46
Liver transplantation for HCC: outcomes applying restrictive selection criteria
Authors N Selection criteria Rec 5y OS Mazzaferro et al. Single < 5cm NEJM nodules < 3cm 8% 74%* Bismuth single < 3cm Sem Liv. Dis 45 3 nodules < 3cm 11 % 74% Llovet et al. Hepatology single < 5cm 4 % 75% Jonas et al single < 5cm 16 % 71 % Hepatology nodules < 3cm * 4y OS

47
HCC Tumorstadien: Indikation für eine Lebertransplantation
(Milan-Kriterien) Keine Fern- oder Lymphknotenmetastasen 3 Tumorknoten mit jeweils 3 cm Durchmesser 1 Tumorknoten 5cm Durchmesser Keine Infiltration in Gefäße
 Keine Fern- oder Lymphknotenmetastasen. 3 Tumorknoten mit jeweils 3 cm Durchmesser. 1 Tumorknoten 5cm Durchmesser. Keine Infiltration in Gefäße.")
48
Therapiealgorithmus HCC Resektion LTx (CLT/LDLT) PEI / RF TACE new
PST 0, Child-Pugh A PST 0-2, Child-Pugh A-B PST >2, Child-Pugh C Very Early Stage Single ≤ 2 cm Early Stage Single or 3 nodules ≤ 3cm, PS 0 Intermediate Stage (B) Multinodular, PS 0 Advanced Stage Portal invasion, N1,M1, PS 1-2 Terminal Stage Single 3 nodules ≤3 cm PVP / bilirubin Increased Associated disease Portal invasion, N1,M1 Normal No Yes No Yes Resektion LTx (CLT/LDLT) PEI / RF TACE new Agents BSC Curativer Treatment RCT AASLD Guidelines 2005
 Multinodular, PS 0. Advanced Stage. Portal invasion, N1,M1, PS 1-2. Terminal. Stage. Single. 3 nodules ≤3 cm. PVP / bilirubin. Increased. Associated disease. Portal invasion, N1,M1. Normal. No. Yes. No. Yes. Resektion. LTx. (CLT/LDLT) PEI / RF. TACE. new. Agents. BSC. Curativer Treatment. RCT. AASLD Guidelines")
49
Perkutane Ethanol Injektion
5. TP activity in human tissues In a study by Miwa and colleagues, the activity of the three enzymes (cytidine deaminase, carboxylesterase and TP) involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81.
 involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81.")
50
Perkutane Ethanol Installation als lokoregionales Therapieverfahren
PEI- Applikation

51
Radiofrequenzthermoablation
5. TP activity in human tissues In a study by Miwa and colleagues, the activity of the three enzymes (cytidine deaminase, carboxylesterase and TP) involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81.
 involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81.")
52
Transkutane Therapie des HCC RFA oder PEI?
HCC-Stadien in den Studien: Single HCC ≤5cm oder 3 HCC ≤3cm, keine Gefäßinvasion, 1cm Abstand vom Hilus und Gallenblase, Child A und B, Thrombozyten >50.000, Quick>50%, nicht operable, keine Vortherapie oder HCC ≤ 4cm, Tumoranzahl <3, Child A und B, keine Vortherapie, >5mm Abstand zum Hilus und DHC Rate der 2-Jahres-Lokalrezidive: PEI versus RFA 11-45% % Anzahl der Therapien bis zu kompletten Ansprechen RFA < PEI Nebenwirkungsprofil RFA < PEI Eine Studie mit besserer 5-Jahresüberlebensrate durch RFA Lin et al, Gut 2005; Shiina et al, Gastroenterology 2005; Lin et al, Gastroenterology 2005; Lencioni Radiology 2003

53
Transarterielle Chemoembolisation
Leberarterien Leber Tumor Art.hepatica T. coeliacus 5. TP activity in human tissues In a study by Miwa and colleagues, the activity of the three enzymes (cytidine deaminase, carboxylesterase and TP) involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81. Aorta Art. iliaca Katheter Embolisat / Chemotherapiegemisch
 involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81. Aorta. Art. iliaca. Katheter. Embolisat / Chemotherapiegemisch.")
54
Chemoembolisation oder Embolisation vs
Chemoembolisation oder Embolisation vs. Supportive Care des nicht-resezierbaren HCC* Studie Anzahl der Patienten Odds ratio (95% CI); Random Effects Model Lin et al., GETCH., Bruix et al., Pelletier et al., Lo et al., Llovet et al., Gesamt 503 p=0.017 Behandlungsbenefit Benefit Kontrolle Remissionsraten in den Studien ca. 30 bis 40 % *Metaanalyse von RTCs Modifiziert nach Llovet JM, et al. Lancet 2003;362:1907–17 54
; Random Effects Model. Lin et al., GETCH., Bruix et al., Pelletier et al., Lo et al., Llovet et al., Gesamt 503. p= Behandlungsbenefit Benefit Kontrolle. Remissionsraten in den Studien ca. 30 bis 40 % *Metaanalyse von RTCs. Modifiziert nach Llovet JM, et al. Lancet 2003;362:1907–")
55
Prospektive Studie zur TACE bei 8510 Patien-
ten mit nicht-resektablem HCC In Abhängigkeit vom Ausmaß der Leberzirrhose In Abhängigkeit vom Tumorstadium Overall Survival Years after Diagnosis Medianes Überleben 34 Monate 5-Jahres Überleben 26 % Takayasu et al. Gastroenterology 2006

56
TACE: Kontraindikationen
extrahepatisch metastasiertes HCC schlechte Leberfunktion (CHE < 3,0) Ejektionsfraktion < 50 % (Doxorubicin) eingeschränkte Nierenfunktion (Cisplatin) CHILD C Portalvenenthrombose Aszites, ausgeprägte port. Hypertension Gefäßinvasion des HCC Tumormasse > 50% der Leber
 Ejektionsfraktion < 50 % (Doxorubicin) eingeschränkte Nierenfunktion (Cisplatin) CHILD C. Portalvenenthrombose. Aszites, ausgeprägte port. Hypertension. Gefäßinvasion des HCC. Tumormasse > 50% der Leber.")
57
Drug eluting Beads Chemotherapiespiegel
5. TP activity in human tissues In a study by Miwa and colleagues, the activity of the three enzymes (cytidine deaminase, carboxylesterase and TP) involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81. Chemotherapiespiegel
 involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81. Chemotherapiespiegel.")
58
Überlebensanalyse von 389 Patienten mit HCC an der MHH
100 BSC TACE + PEI PEI TACE Resektion 5. TP activity in human tissues In a study by Miwa and colleagues, the activity of the three enzymes (cytidine deaminase, carboxylesterase and TP) involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274–81. 50 1 2 3 4 5 6 Greten et al Br. J Cancer 2005
 involved in the conversion of Xeloda to 5-FU was measured.1 Samples of healthy and tumour tissue were taken from each patient. TP activity was found to be significantly higher in tumour tissue than in healthy tissue from the same individual in breast, gastric, colorectal, cervical, uterine, renal, bladder, thyroid and ovarian cancers. The study also showed that carboxylesterase was found almost exclusively in the liver and showed little variation in activity between normal and tumour tissue. Analysis of cytidine deaminase revealed that this enzyme was more active in tumour tissue and the liver than in normal tissue adjacent to malignant cells. 1. Miwa M, Ura M, Nishida M et al. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998;34:1274– Greten et al Br. J Cancer")
59
Durchgeführte Therapien an 389 Patienten
OP 6 % PEI 18 % BSC 50 % TACE 13 % TACE + PEI 13 % Greten et al Br. J Cancer 2005

60
Therapiealgorithmus HCC Resektion LTx (CLT/LDLT) PEI / RF TACE new
PST 0, Child-Pugh A PST 0-2, Child-Pugh A-B PST >2, Child-Pugh C Very Early Stage Single ≤ 2 cm Early Stage Single or 3 nodules ≤ 3cm, PS 0 Intermediate Stage (B) Multinodular, PS 0 Advanced Stage Portal invasion, N1,M1, PS 1-2 Terminal Stage Single 3 nodules ≤3 cm PVP / bilirubin Increased Associated disease Portal invasion, N1,M1 Normal No Yes No Yes Resektion LTx (CLT/LDLT) PEI / RF TACE new Agents BSC Curativer Treatment RCT AASLD Guidelines 2005
 Multinodular, PS 0. Advanced Stage. Portal invasion, N1,M1, PS 1-2. Terminal. Stage. Single. 3 nodules ≤3 cm. PVP / bilirubin. Increased. Associated disease. Portal invasion, N1,M1. Normal. No. Yes. No. Yes. Resektion. LTx. (CLT/LDLT) PEI / RF. TACE. new. Agents. BSC. Curativer Treatment. RCT. AASLD Guidelines")
61
Therapiealgorithmus HCC Resektion LTx (CLT/LDLT) PEI / RF TACE new
PST 0, Child-Pugh A PST 0-2, Child-Pugh A-B PST >2, Child-Pugh C Very Early Stage Single ≤ 2 cm Early Stage Single or 3 nodules ≤ 3cm, PS 0 Intermediate Stage (B) Multinodular, PS 0 Advanced Stage Portal invasion, N1,M1, PS 1-2 Terminal Stage Single 3 nodules ≤3 cm PVP / bilirubin Increased Associated disease Portal invasion, N1,M1 Normal No Yes No Yes Resektion LTx (CLT/LDLT) PEI / RF TACE new Agents BSC Curativer Treatment RCT AASLD Guidelines 2005
 Multinodular, PS 0. Advanced Stage. Portal invasion, N1,M1, PS 1-2. Terminal. Stage. Single. 3 nodules ≤3 cm. PVP / bilirubin. Increased. Associated disease. Portal invasion, N1,M1. Normal. No. Yes. No. Yes. Resektion. LTx. (CLT/LDLT) PEI / RF. TACE. new. Agents. BSC. Curativer Treatment. RCT. AASLD Guidelines")
62
El Serag and Rudolph, Gastroenterology 2007

63
HCC - molekulare Therapie 2005-2007
Autor Protokoll N RR PFS/TTP MS Anti-EGFR O´Dwyer 06 Gefitinib 31 3,2 2,3 NA NA Ramanathan 06 Lapatinib 37 5% 2,3 NA 6,2 Philip 05 Erlotinib 38 9 % 3,2 32% 13 Grünwald 07 Cetuximab ,0 22,2% NA Louafi 07 GemOx+Cetux 37 24% 4,5 40% 9,2 Antiangiogenese Kanai 06 TSU % NA NA NA Schwatz 06 Bevacizumab 30 10% 6,5 NA NA Malka 07 Bevacizumab 24 12,5 3,5 17% NA Zhu 06 GemOx-Beva 33 20% 5,3 48% 9,6 Sun 07 CapOx+Beva 30 13,3 4,5 45% 10,6 Multikinase-I Abou-Alfa 04 Sorafenib 137 5% 5,6 37% 9,5 Llovet 07 Sorafenib 299* 2,3 5,5 NA 10,7 Zhu 07 Sunitinib 26 3,8 4,1 35% 11,6 Faiver 07 Sunitinib 37 2,7 5,2 35% 11,2 Multi-target Ansatz Thomas 07 Erlotinib+Beva 29 20,6 8,8 NA 19

65
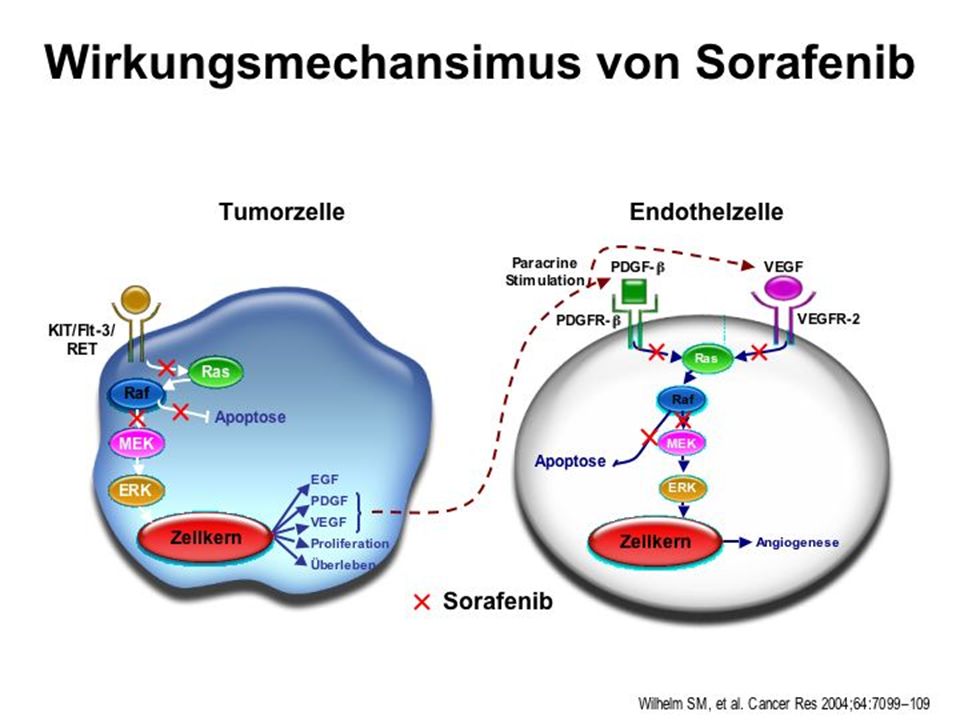
Sorafenib: B-RAF und VEGFR-Inhibitor
Tumorzelle Endothelzelle, Perizyten Sorafenib Sorafenib Sorafenib antiproliferativ antiangiogenetisch Wilhelm S et al. Clin Cancer Res. 2003;9(suppl). Abstract A78. 65 65
. Abstract A")
67
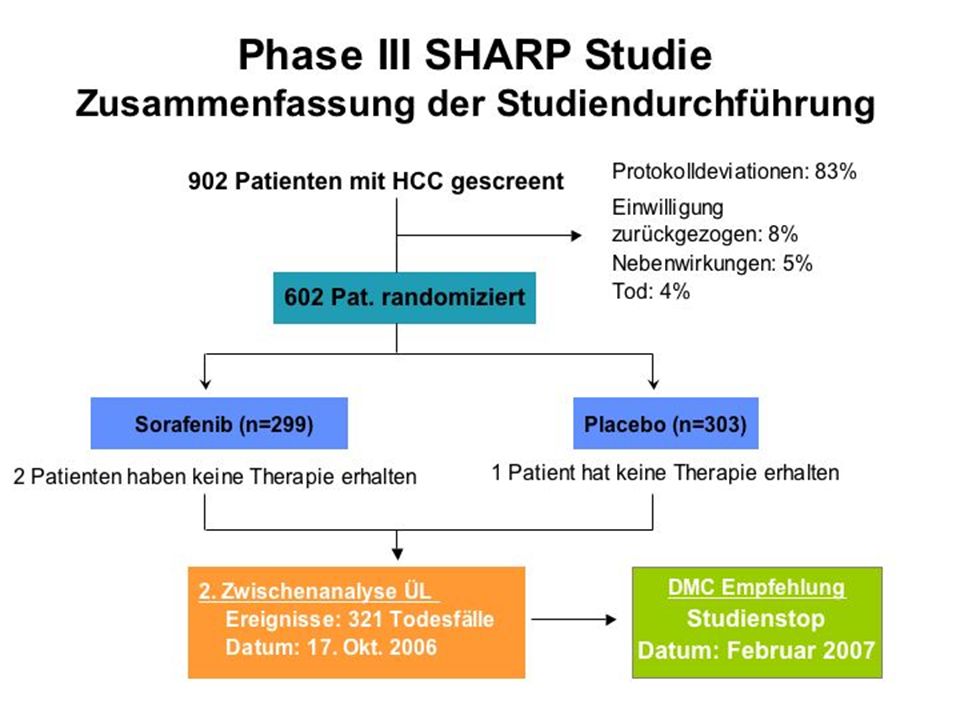
SHARP Trial n= 602 902 Pts screened R A N D O M Overall survival TTSP
• Treatment: continuous dosing of Sorafenib 400 mg po bid • Treatment is continued until radiological and symptomatic progression 902 Pts screened Protocol deviations 83% Consent withdrawn 8% Adverse invents 5% Death 4% R A N D O M Primary Endpoints: Overall survival TTSP 2nd interim Analysis OS Oct 2006 DMC: stop RCT! Feb 2007 Sorafenib (n=299) n= 602 Placebo (n=303)
 n= 602. Placebo. (n=303)")
71
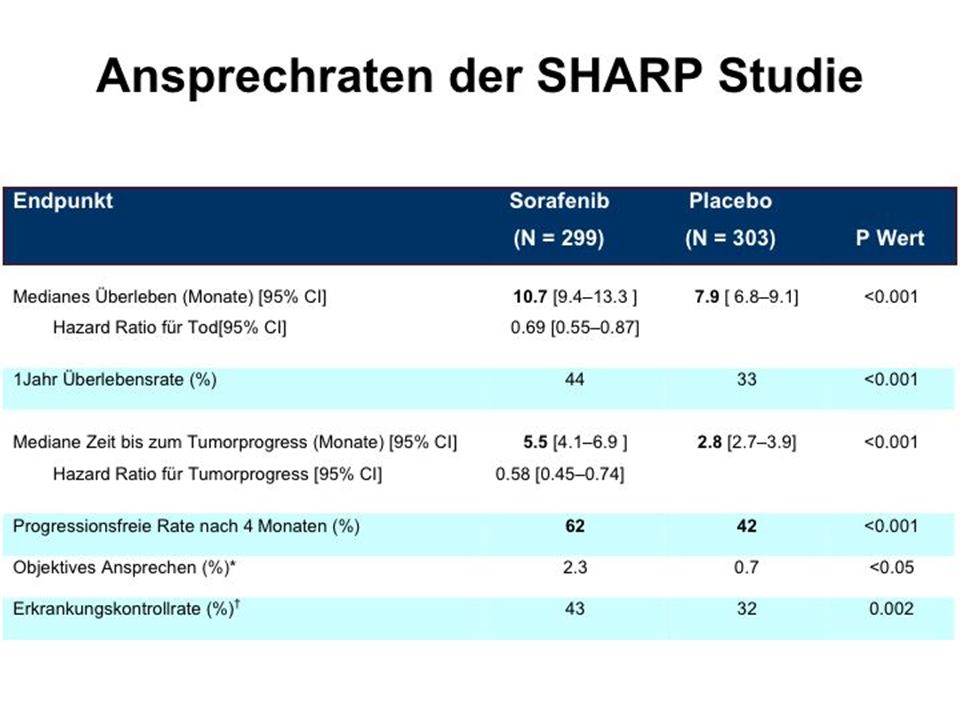
Phase III SHARP Studie: Gesamtüberleben (Intention-to-treat)
1.00 0.75 0.50 0.25 Sorafenib Median: 46,3 Wochen (10,7 Monate) (95% CI: 40,9–57,9) Placebo Median: 34,4 Wochen (7,9 Monate) (95% CI: 29,4–39,4) Überlebenswahrscheinlichkeit Hazard ratio (S/P): 0.69 (95% CI: 0.55–0.88) p= * 8 16 24 32 40 48 56 64 72 80 Wochen 274 241 205 161 108 67 38 12 Patientenanzahl Sorafenib: 276 224 179 126 78 47 25 7 2 Placebo: 299 303 *O’Brien–Fleming-Grenzwert für statistische Signifikanz war p=0.0077 Llovet JM, et al., ASCO 2007, Chicago, IL, USA 71
 (95% CI: 40,9–57,9) Placebo Median: 34,4 Wochen (7,9 Monate) (95% CI: 29,4–39,4) Überlebenswahrscheinlichkeit. Hazard ratio (S/P): 0.69 (95% CI: 0.55–0.88) p= * Wochen Patientenanzahl Sorafenib: Placebo: *O’Brien–Fleming-Grenzwert für statistische Signifikanz war p= Llovet JM, et al., ASCO 2007, Chicago, IL, USA. 71.")
74
Hand Foot Skin Reaction

76
treatment or new agents
Stadien - adaptierte Therapie des HCC PST 0, PST PST 2 Child A, Child A-B Child C Okuda Okuda Okuda 3 very early stage early stage intermediate advanced terminal Single<2cm single ≤ 5cm or >3 nodules portal invasion stage D Carcinoma in situ ≤ 3 nodules ≤3cm single >5cm N1 / M1, Performance (PST) PST PST PST 1-2 Normal portal pressure Liver function : CHE >3, Normal Bilirubin Downstaging ? (neoadjuvant) Portal invasion or N1 or M1 Yes No Associated disease No Yes No Yes Symptomatic treatment or new agents Sorafenib (Child A) Resection LTX RFA/PEI Chemoembo
 0 PST 0 PST 0 PST 1-2. Normal portal pressure. Liver function : CHE >3, Normal Bilirubin. Downstaging (neoadjuvant) Portal invasion or. N1 or M1. Yes No. Associated disease. No Yes. No Yes. Symptomatic. treatment or new agents. Sorafenib. (Child A) Resection LTX RFA/PEI Chemoembo.")
77
Offene Fragen der zielgerichteten HCC-Therapie
Sorafenib +/- X-nib u/o Y-mab ? Sorafenib vs. Bev/Tarceva - Kombination mit CTx bei CLIP 0-2? - Bei N0 oder M0 Kombination mit TACE? - Adjuvante Therapie nach RFA/Resektion? - Sorafenib + LTX = > Milan ?

78
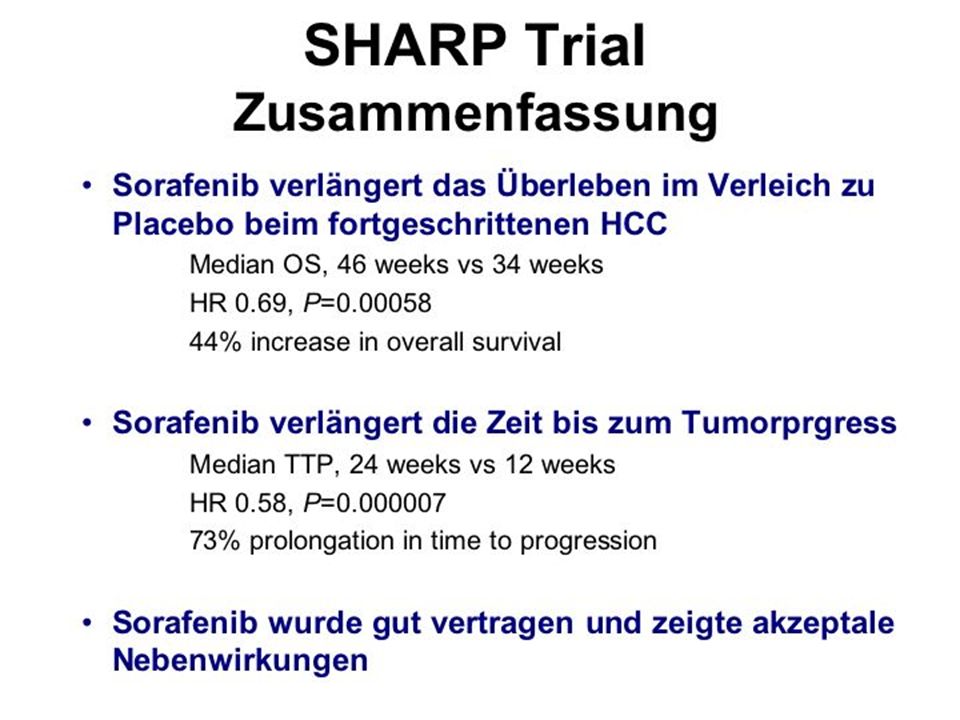
Sorafenib für Patienten mit HCC
Pro Erste Phase III Studie die eine signifikante Verlängerung des Überlebens durch eine systemische Therapie zeigt 44%-ige Verbesserung des Überlebens Relativ gute Verträglichkeit bei Patienten mit HCC und Child A Contra Selektiertes Patientenkollektiv: Europäer, Child A „Nur“ 2,7 Monate absolute Verlängerung des mittleren Überlebens Zeit bis zur symptomatischen Tumorprogression nicht verändert Einfluss auf die Lebensqualität bleibt unklar („clinical benefit?“) Kosten: ca. 4500,- € pro Monat
 Kosten: ca. 4500,- € pro Monat.")
79
Klinisch-experimentelle Ansätze an der MHH
Identifikation von small molecules: BMBF BIOPHARMA Phase II Studie zur Therapie mit Cetuximab (Erbitux) Testung von „drug-eluting“ Beads zur TACE Immuntherapeutische Ansätze: Peptidvakzination Depletion von regulatorischen T-Zellen
 Testung von „drug-eluting Beads zur TACE. Immuntherapeutische Ansätze: Peptidvakzination. Depletion von regulatorischen T-Zellen.")
80
“Immunotherapies against Cancer”
Helmholtz Alliance “Immunotherapies against Cancer” tumor CTL CD8 CD4 Tumor dendritische Zelle Greten et al. Design einer Tumorvakzine zur spezifischen Stimulation des eigenen Immunsystems gegen den Tumor

81
treatment or new agents
Stadien - adaptierte Therapie des HCC PST 0, PST PST 2 Child A, Child A-B Child C Okuda Okuda Okuda 3 SIRT very early stage early stage intermediate advanced terminal Single<2cm single ≤ 5cm or >3 nodules portal invasion stage D Carcinoma in situ ≤ 3 nodules ≤3cm single >5cm N1 / M1 Normal portal pressure Liver function : CHE >3, Normal Bilirubin Radiation Downstaging ? (neoadjuvant) Yes No Associated disease Child A Child B/C No Yes Symptomatic treatment or new agents Sorafenib Resection LTX RFA/PEI Chemoembo
 Yes No. Associated disease. Child A Child B/C. No Yes. Symptomatic. treatment or new agents. Sorafenib. Resection LTX RFA/PEI Chemoembo.")
82
Molekulare Vorhersage zum Ansprechen auf
5-FU+IFN-a beim fortgeschrittenen HCC 20 Pat. mit HCC mit Infiltration der Portalvene A 1.0 0.8 0.6 Genearray mit 3080 Genen overall survival rate 0.4 P=0.001 0.2 12 24 36 48 60 B months after surgery 1.0 0.8 0.6 disease-free survival rate 0.4 Identifikation von 63 Genen mit einem p Wert < 0.01 P=0.002 0.2 12 24 36 48 60 months after surgery Kurokowa ClinCanRes (2004) 10:6029
 10:6029.")
83
Phase II Study of Sorafenib in advanced HCC
(JCO 2006, 24:1) 400 mg Sorafenib 2 x tgl. 137 Patienten: OS: Monate PR: 3 Patienten MR: 8 Patienten SD über mind. 16 Wo: %) pERK Färbung
 400 mg Sorafenib 2 x tgl. 137 Patienten: OS: 9.2 Monate. PR: 3 Patienten. MR: 8 Patienten. SD über mind. 16 Wo: %) pERK Färbung.")
84
Design Stratification Randomization
International, multicentre Phase III study Inclusion criteria: Histology proven HCC Advanced HCC At least one measurable untreated lesion ECOG 0-2 Child-Pugh A No prior systemic treatment Stratification Macroscopic vascular invasion a/o extrahepatic spread ECOG PS Geographical region Randomization Double-blind placebo-controlled trial Accrual: March 2005 to April 2006

85
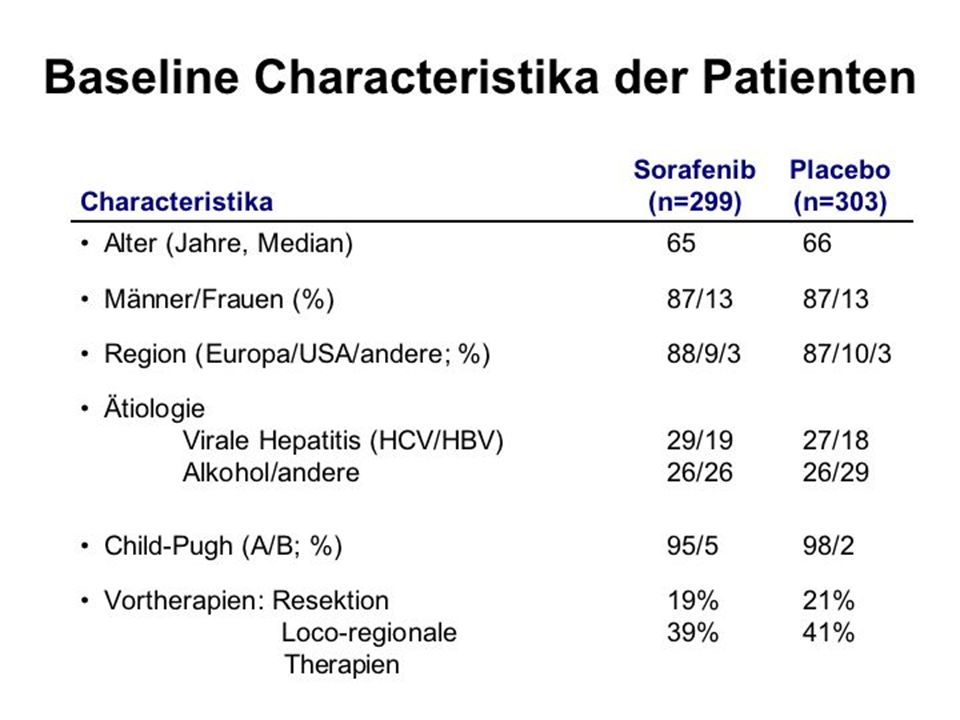
Baseline characteristics of patients
Sorafenib Placebo n=299 n=303 Age (median) 65 66 Male/Female 87 / / 13 Region (E / North Am / others) 88 / 9 / 3 87 / 10 / 3 Etiology (%) viral Hepatitis (HCV / HBV) 29 / / 18 Alcohol / other 26 / / 29 Child-Pugh (A/B; %) 95 / 5 98 /2 Prior therapies surgical resection 19 % 21 % Loco-regional therapies 39 % 41 %
 Male/Female 87 / / 13. Region (E / North Am / others) 88 / 9 / 3 87 / 10 / 3. Etiology (%) viral Hepatitis (HCV / HBV) 29 / / 18. Alcohol / other 26 / / 29. Child-Pugh (A/B; %) 95 / 5 98 /2. Prior therapies. surgical resection 19 % 21 % Loco-regional therapies 39 % 41 %")
86
Baseline characteristics of patients
Sorafenib Placebo n=299 n=303 BCLC stage (%) stage B (intermediate) 18 17 stage C (advanced) 82 83 ECOG ECOG ECOG 2 8 7 Vascular invasion / extrahepatic spread (%) present 70 70 absent 30 30
 stage B (intermediate) stage C (advanced) ECOG ECOG ECOG Vascular invasion / extrahepatic spread (%) present absent")
87
Exploratory subgroup survival analysis
SHARP Trial: Exploratory subgroup survival analysis ECOG PS 0 ECOG PS 1-2 No extrahepatic spread Extrahepatic spread No macro. vascular invasion Macro. vascular invasion No MVI / extrahep. spread MVI a/o extrahep. spread Hazard Radio (95% CI) Sorafenib benefit Placebo benefit
 Sorafenib benefit Placebo benefit.")
88
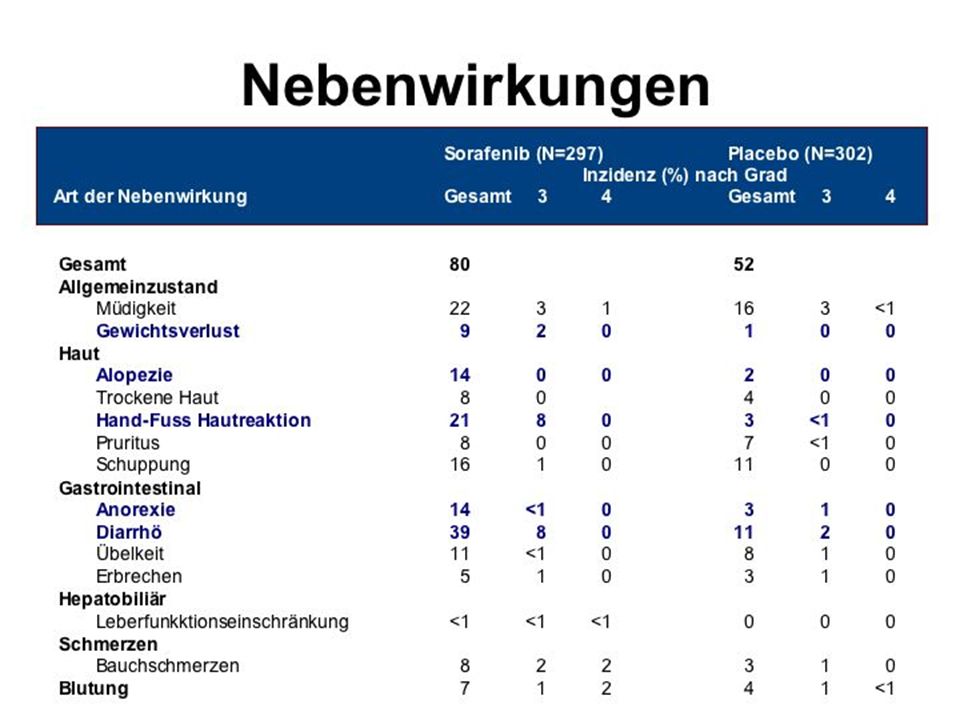
Safety events Sorafenib Placebo (n=299) (n=303)
Treatment emergent SAE (%) Drug related SAE (%) Drug related adverse events (%) All Grade 3/4 All Grade 3/4 Diarrhea 39 8/- 11 2/- Pain (abdomen) 8 2/- 3 <1/- Weight loss 9 2/- <1 0/- Anorexia 14 <1/- 3 <1/- Nausea 11 <1/- 8 <1/- Hand-foot skin reaction 21 8/- 3 <1/- Vomiting 5 1/- 3 <1/- Alopecia 14 0/- 2 0/- Liver dysfunction <1 <1/- 0 0/- Bleeding 7 <1/- 4 <1/<1
 Drug related SAE (%) Drug related adverse events (%) All Grade 3/4 All Grade 3/4. Diarrhea 39 8/- 11 2/- Pain (abdomen) 8 2/- 3 <1/- Weight loss 9 2/- <1 0/- Anorexia 14 <1/- 3 <1/- Nausea 11 <1/- 8 <1/- Hand-foot skin reaction 21 8/- 3 <1/- Vomiting 5 1/- 3 <1/- Alopecia 14 0/- 2 0/- Liver dysfunction <1 <1/- 0 0/- Bleeding 7 <1/- 4 <1/<1.")
89
SHARP Trial – Results and Toxicity
Sorafenib Placebo n=299 n=303 Median OS (mo) 10,7 7,9 TTSP - no significant difference – Median TTP (mo) 5,5 2,8 Toxicity Serious adverse events 52 54 Diarrhoea 8 2 HF skin toxicity 8 <1 p= p=
 10,7 7,9. TTSP - no significant difference – Median TTP (mo) 5,5 2,8. Toxicity. Serious adverse events Diarrhoea 8 2. HF skin toxicity 8 <1. p= p=")
90
Final results from a phase II randomized double-blind study of Sorafenib plus doxorubicin (S+D) versus placebo plus doxorubicin (P+D) in patients (pts) with advanced hepatocellular carcinoma. Abou-Alfa et al. ASCO-GI 2008 A-HCC, Child A, PS 0-2, no prior therapy n= 49 n=47 Doxorubicin 60mg/m2 i.V. d1, q22 + Placebo Max. 18 weeks until progression R Doxorubicin 60mg/m2 i.V. d1, q22 + Sorafenib 400mg p.o. 2x/die Max. 18 weeks until progression TTP OS PFS OR 3/4 fatuige 3/4 Neutrop. D+P 4,8 Mo 6,5 Mo 2,8 Mo 2 % 15 % 46 % D+S 8,6 Mo 13,7 Mo 6,9 Mo 4 % 15 % 53 %

91
treatment or new agents
Stadien - adaptierte Therapie des HCC PST 0, PST PST 2 Child A, Child A-B Child C Okuda Okuda Okuda 3 very early stage early stage intermediate advanced terminal Single<2cm single ≤ 5cm or >3 nodules portal invasion stage D Carcinoma in situ ≤ 3 nodules ≤3cm single >5cm N1 / M1, Performance (PST) PST PST PST 1-2 Normal portal pressure Liver function : CHE >3, Normal Bilirubin Downstaging ? (neoadjuvant) Yes No Associated disease Child A Child B/C No Yes Symptomatic treatment or new agents Sorafenib Resection LTX RFA/PEI Chemoembo
 0 PST 0 PST 0 PST 1-2. Normal portal pressure. Liver function : CHE >3, Normal Bilirubin. Downstaging (neoadjuvant) Yes No. Associated disease. Child A Child B/C. No Yes. Symptomatic. treatment or new agents. Sorafenib. Resection LTX RFA/PEI Chemoembo.")
92
…weitere offene Fragen der HCC-Therapie
Sorafenib +/- X-nib u/o Y-mab ? - Kombination mit CTx? - Bei N0 oder M0 Kombination mit TACE? - Adjuvante Therapie nach RFA/Resektion? - Sorafenib + LTX = > Milan ?

93
Systemische Chemotherapie beim HCC
MDR1 Genexpression => p-Glycoprotein Eingeschränkte Leberleistung =>Toxizität Schlechter Performance Status Ascites Portalvenenthrombose Bilirubin > 2.0 mg/dL Nagahama 1997 Doxorubicin Fluoropyrimidine Anthrazykline Topoisomeraseinhibitoren Nukleosidanaloga Cisplatin Thymidilatsynthetaseinhibitoren Taxane Nowak 2004

94
treatment or new agents
Stadien - adaptierte Therapie des HCC PST 0, PST PST 2 Child A, Child A-B Child C Okuda Okuda Okuda 3 very early stage early stage intermediate advanced terminal Single<2cm single ≤ 5cm or >3 nodules portal invasion stage D Carcinoma in situ ≤ 3 nodules ≤3cm single >5cm N1 / M1, Performance (PST) PST PST PST 1-2 Normal portal pressure Liver function : CHE >3, Normal Bilirubin Downstaging ? (neoadjuvant) Portal invasion or N1 or M1 Yes No Associated disease No Yes No Yes Symptomatic treatment or new agents Sorafenib (Child A) Resection LTX RFA/PEI Chemoembo
 0 PST 0 PST 0 PST 1-2. Normal portal pressure. Liver function : CHE >3, Normal Bilirubin. Downstaging (neoadjuvant) Portal invasion or. N1 or M1. Yes No. Associated disease. No Yes. No Yes. Symptomatic. treatment or new agents. Sorafenib. (Child A) Resection LTX RFA/PEI Chemoembo.")
Ähnliche Präsentationen




 bei der>")

 BENCHMRK: Blocking integrase in treatment Experienced patients.>")
 U N I V E R S I T Ä T H A M B U R G November 2011.>")
 U N I V E R S I T Ä T H A M B U R G November 2011.>")
Media Landesanstalt für Kommunikation Baden-Württemberg (LFK) Landeszentrale für Medien und Kommunikation.>")










