Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Thema / Bereich / Anlass Reizdarm und die FODMAP arme Ernährung
2. Fortbildungsnachmittag Klinische Ernährung Kantonsspital St.Gallen Dr. med. Claudia Krieger, Oberärztin Gastroenterologie/Hepatologie Referent / Bereich

2
Thema / Bereich / Anlass Reizdarm und die FODMAP arme Ernährung
Definition Pathophysiologie Ernährungsumstellung Literatur Referent / Bereich

3
Ernährung als Therapie ?
Symptomaggravation durch Nahrungsmittel Selbstdiagnostizierte Unverträglichkeiten → verminderte Lebensqualität → Aklärung von Intoleranzen Bohn L, Storsrud S, Tornblom H et al. Am J Gastroenterol. 2013;108(5), Simrén M, Mansson A, Langkilde. Am et al. Digestion 2001;63: , Monsbakken KW, Vandvik PO, Raup PG Eur J Clin Nutr 2006;60:667-72
, Simrén M, Mansson A, Langkilde. Am et al. Digestion 2001;63: , Monsbakken KW, Vandvik PO, Raup PG Eur J Clin Nutr 2006;60:")
4
Thema / Bereich / Anlass
Wie alles begann… In den 80er und 90er Jahren Hinweise auf Induktion von IBS-Symptomen unter Provokationstests mit Kohlenhydraten (Fruktose, Fruktooligosacharide, Sorbitol, Sucrose) Keine Symptome nach Sucrose Symptombesserung von IBS-Patienten nach Elimination dieser Kohlenhydrate Bezüglich Anteile dieser Kohlenhydrate in Nahrungsmitteln herrschte Unklarheit Twenty-five patients with functional bowel disease were given fructose, sorbitol, fructose-sorbitol mixtures, and sucrose. The occurrence of malabsorption was evaluated by means of hydrogen breath tests and the gastrointestinal symptoms, if any, were recorded. One patient could not be evaluated because of lack of H2 production. Based on a cut-off level of 10 ppm rise of H2 concentration, malabsorption was apparent in 13 patients, in 7 of which the calculated absorption capacities were below 15 g. In contrast, in patients given 50 g of sucrose, malabsorption could not be detected. Ingestion of fructose caused marked abdominal distress in patients with demonstrable malabsorption. Ingestion of sucrose in these patients gave less pronounced symptoms of abdominal distress. Malabsorption of a 5-g dose of sorbitol could be detected in 8 of 13 patients. Mixtures of 25 g of fructose and 5 g of sorbitol caused significantly increased abdominal distress, and more than additive malabsorption was found in several cases. The present study shows that pronounced gastrointestinal distress may be provoked by malabsorption of small amounts of fructose, sorbitol, and fructose-sorbitol mixtures in patients with functional bowel disease. The findings may have direct influence on the dietary guidance given to a major group of patients with functional bowel disease and may make it possible to define separate entities in this disease complex. Sucrose: Glucose-Fructose Disaccharid (Tafelzucker). Rumessen JJ, Gudmand-Hoyer E. Gastroenterology. 1988;95(3): Referent / Bereich
 Keine Symptome nach Sucrose. Symptombesserung von IBS-Patienten nach Elimination dieser Kohlenhydrate. Bezüglich Anteile dieser Kohlenhydrate in Nahrungsmitteln herrschte Unklarheit. Twenty-five patients with functional bowel disease were given fructose, sorbitol, fructose-sorbitol mixtures, and sucrose. The occurrence of malabsorption was evaluated by means of hydrogen breath tests and the gastrointestinal symptoms, if any, were recorded. One patient could not be evaluated because of lack of H2 production. Based on a cut-off level of 10 ppm rise of H2 concentration, malabsorption was apparent in 13 patients, in 7 of which the calculated absorption capacities were below 15 g. In contrast, in patients given 50 g of sucrose, malabsorption could not be detected. Ingestion of fructose caused marked abdominal distress in patients with demonstrable malabsorption. Ingestion of sucrose in these patients gave less pronounced symptoms of abdominal distress. Malabsorption of a 5-g dose of sorbitol could be detected in 8 of 13 patients. Mixtures of 25 g of fructose and 5 g of sorbitol caused significantly increased abdominal distress, and more than additive malabsorption was found in several cases. The present study shows that pronounced gastrointestinal distress may be provoked by malabsorption of small amounts of fructose, sorbitol, and fructose-sorbitol mixtures in patients with functional bowel disease. The findings may have direct influence on the dietary guidance given to a major group of patients with functional bowel disease and may make it possible to define separate entities in this disease complex. Sucrose: Glucose-Fructose Disaccharid (Tafelzucker). Rumessen JJ, Gudmand-Hoyer E. Gastroenterology. 1988;95(3): Referent / Bereich")
5
Thema / Bereich / Anlass
Wie alles begann… The subsequent rapid fermentation of FODMAPs in the distal small and proximal large intestine induces conditions in the bowel that lead to increased intestinal permeability, a predisposing factor to the development of Crohn’s disease The concept has biological plausibility in that inefficiencies in the intestinal barrier may lead to increased mucosal exposure to luminal pro-inflammatory molecules and micro-organisms, and to subsequent potential modulation of the mucosal immune responsiveness. Gibson PR, Shepherd SJ. Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
: Referent / Bereich")
6
Thema / Bereich / Anlass
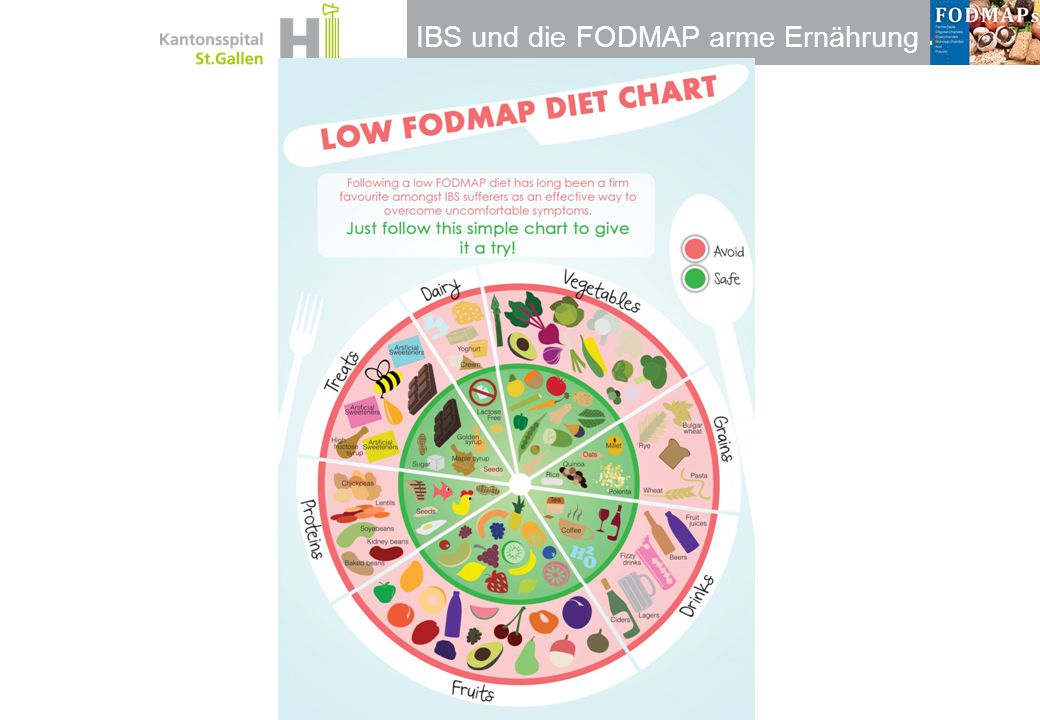
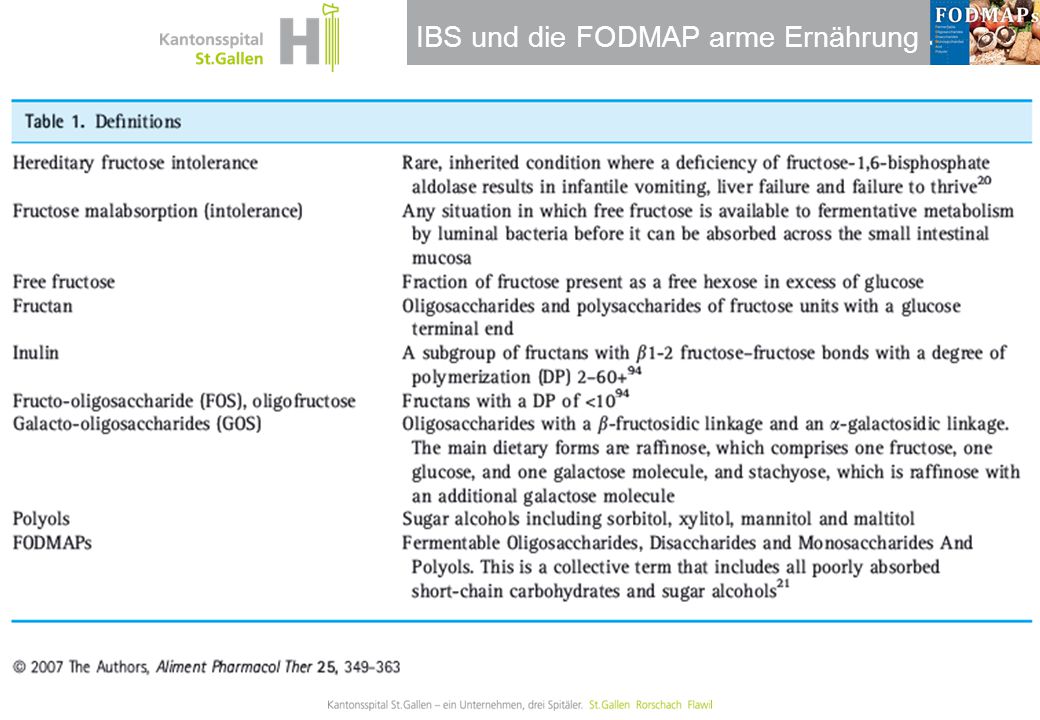
Definition FODMAP Fermentierbare Oligosaccharide Disaccharide Monosaccharide And Polyole Es handelt sich somit um eine Gruppe von kurzkettigen Kohlenhydraten und mehrwertigen Alkoholen, welche in vielen Nahrungsmitteln vorkommen. Gibson PR, Shepherd SJ. Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
: Referent / Bereich")
7
Wie alles begann… die FODMAP Hypothese
Thema / Bereich / Anlass Wie alles begann… die FODMAP Hypothese The subsequent rapid fermentation of FODMAPs in the distal small and proximal large intestine induces conditions in the bowel that lead to increased intestinal permeability, a predisposing factor to the development of Crohn’s disease The concept has biological plausibility in that inefficiencies in the intestinal barrier may lead to increased mucosal exposure to luminal pro-inflammatory molecules and micro-organisms, and to subsequent potential modulation of the mucosal immune responsiveness. Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
: Referent / Bereich")
8
Pathophysiologie Symptome bei FODMAP
Thema / Bereich / Anlass Pathophysiologie Symptome bei FODMAP Kurzkettige nicht resorbierte Kohlenhydrate → endoluminaler Wassereinstrom → erhöhte Gasproduktion →intestinalen Distension mit Symptomen wie Meteorismus, Flatulenz, Abdominalgien, Veränderung der Motilität und erhöhte intestinale Permeabilität J. Barrett, P. Gibson 2007; Pract. Gastroenterol Referent / Bereich

9
IBS - viszerale Hypersensitivität
Thema / Bereich / Anlass IBS - viszerale Hypersensitivität IBS Intensity of discomfort sensation. (B) Patients with IBS as a whole perceived phasic rectal distention more intensely than controls at pressures up to 40 mm Hg. Values are shown as mean +_ SEM; *P < 0.05. Background & Aims: Lowered visceral perception thresholds have been suggested as a biological marker of irritable bowel syndrome (IBS). The current study sought to determine the prevalence of altered rectal visceral perception in patients with IBS and the correlation of altered perception thresholds with subjective symptoms. Methods: Anorectal manometry and rectal perception thresholds to balloon distention were determined in 100 patients with IBS and 15 control subjects. Gastrointestinal and psychological symptoms were assessed by questionnaire. Perception thresholds and symptoms were reassessed after 3 months in 15 patients with IBS. Results: Ninety-four percent of patients showed altered rectal perception in the form of lowered thresholds for aversive sensations (discomfort), increased intensity of sensations, or altered viscerosomatic referral. Hypersensitivity was found only for aversive sensations in response to rapid phasic distention; stool thresholds and thresholds in response to slow ramp distention were normal. Cluster analysis by physiological parameters identified three IBS subgroups with predominant patterns of symptoms. Longitudinal evaluation indicated a correlation between changes in perception thresholds and symptom severity. Conclusions: Because altered rectal perception is present in almost all patients with IBS and perception thresholds correlate with temporal changes in retrospective symptom severity, altered rectal perception represents a reliable biological marker of IBS. Gesund Mertz H et al. Gastroenterology 109: 40-51; 1995 Referent / Bereich
 Patients with IBS as a whole perceived phasic rectal distention more intensely than controls at pressures up to 40 mm Hg. Values are shown as mean +_ SEM; *P < Background & Aims: Lowered visceral perception thresholds have been suggested as a biological marker of irritable bowel syndrome (IBS). The current study sought to determine the prevalence of altered rectal visceral perception in patients with IBS and the correlation of altered perception thresholds with subjective symptoms. Methods: Anorectal manometry and rectal perception thresholds to balloon distention were determined in 100 patients with IBS and 15 control subjects. Gastrointestinal and psychological symptoms were assessed by questionnaire. Perception thresholds and symptoms were reassessed after 3 months in 15 patients with IBS. Results: Ninety-four percent of patients showed altered rectal perception in the form of lowered thresholds for aversive sensations (discomfort), increased intensity of sensations, or altered viscerosomatic referral. Hypersensitivity was found only for aversive sensations in response to rapid phasic distention; stool thresholds and thresholds in response to slow ramp distention were normal. Cluster analysis by physiological parameters identified three IBS subgroups with predominant patterns of symptoms. Longitudinal evaluation indicated a correlation between changes in perception thresholds and symptom severity. Conclusions: Because altered rectal perception is present in almost all patients with IBS and perception thresholds correlate with temporal changes in retrospective symptom severity, altered rectal perception represents a reliable biological marker of IBS. Gesund. Mertz H et al. Gastroenterology 109: 40-51; Referent / Bereich")
10
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Raffinose, Stachyose Lactasemangel: 2% Scandinavien vs > 90% in Asien Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
: Referent / Bereich")
11
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Raffinose, Stachyose Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
: Referent / Bereich")
12
Thema / Bereich / Anlass
Lactose Disaccharid: Glucose - Galactose Lactase im prox. Dünndarm 1-95% Gibson P et al. Aliment Pharmacol 2006 Referent / Bereich

13
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Raffinose, Stachyose Keine Absorption bei Lactasemangel Lactasemangel: 2% Scandinavien vs > 90% in Asien Gibson PR, Shepherd SJ. Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
: Referent / Bereich")
14
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Raffinose, Stachyose Fructose: absorbiert mit Glucose oder als Sucrose (Glucose mit Fructose) ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Fructose aufzunehmen. Gibson PR, Shepherd SJ. Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
 ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Fructose aufzunehmen. Gibson PR, Shepherd SJ. Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich")
15
Thema / Bereich / Anlass
Fruktose / Fructane Monosacharid Disaccharid: Glucose + Fructose Polymerisierte Form: Fructane Inulin: n > 10 FOS: n = < 10 Fructose: absorbiert mit Glucose oder als Sucrose (Glucose mit Fructose) ca 85%. Freie Fructose kann nur reduziert mittels glucose-unabängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Fructose aufzunehmen. Fructose: Beitrag zu Adipositas? Fructane werden im Dünndarm gar nicht aufgespalten/ hydrolisiert werden. Aufbruch durch Kauen. Werden zu 90% wieder ausgeschieden. Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Gibson P et al., Aliment Pharmacol 2006 Referent / Bereich
 ca 85%. Freie Fructose kann nur reduziert mittels glucose-unabängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Fructose aufzunehmen. Fructose: Beitrag zu Adipositas Fructane werden im Dünndarm gar nicht aufgespalten/ hydrolisiert werden. Aufbruch durch Kauen. Werden zu 90% wieder ausgeschieden. Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Gibson P et al., Aliment Pharmacol Referent / Bereich")
16
Thema / Bereich / Anlass
Fruktose Die Bedeutung der Intestinalen Fruktoseintoleranz hat in der Vergangenheit zugenommen, da sich die Menge an Fructose in der Nahrung in den letzten Jahren durch industriell bereitgestellte Süßungsmittel dramatisch erhöht hat.[1] Schätzungen der Verbreitung gehen von bis zu 30 % der Gesamtbevölkerung in westlichen Ländern und Afrika aus und deuten eine mit 10 % der Bevölkerung geringere Verbreitung in Asien an. SGLT1: Sodium/Glc/Galact Cotransporter GLUT2: Fakultativ, Glc / Fruct / Galact, hohe Kapazität GLUT5: Fakultativ, fructosespezifisch, niedrige Kapazität → Fruktosemalabsorption ist physiologisch Fructose malabsorption may be reduced by regarding it not as an abnormality but as a physiological process offering an opportunity to improve functional gastrointestinal symptoms by dietary change. P. Gibson Referent / Bereich

17
Thema / Bereich / Anlass
Fruktose Fruktosemalabsorption definiert durch Nachweis von H2-Anstieg (15ppm) nach Gabe von 25 g Fruktose (Atemtest) Tgl. Einnahme 11 – 54 g Prävalenz Dosisabhängig 53% bei 25 g Fruktose 73% bei 50 g Fruktose Die Bedeutung der Intestinalen Fruktoseintoleranz hat in der Vergangenheit zugenommen, da sich die Menge an Fructose in der Nahrung in den letzten Jahren durch industriell bereitgestellte Süßungsmittel dramatisch erhöht hat.[1] Schätzungen der Verbreitung gehen von bis zu 30 % der Gesamtbevölkerung in westlichen Ländern und Afrika aus und deuten eine mit 10 % der Bevölkerung geringere Verbreitung in Asien an. Fructose malabsorption may be reduced by regarding it not as an abnormality but as a physiological process offering an opportunity to improve functional gastrointestinal symptoms by dietary change Süssgetränke! SGLT1: Sodium/Glc/Galact Cotransporter GLUT2: Fakultativ, Glc / Fruct / Galact, hohe Kapazität GLUT5: Fakultativ, fructosespezifisch, niedrige Kapazität Skoog SM, Bharucha AE. Am J Gastroenterol. 2004;99: Beyer PL et al. J Am Diet Assoc, 2005;105: P. Gibson et al, Aliment Pharmacol Ther 2006; 25, Referent / Bereich
 nach Gabe von 25 g Fruktose (Atemtest) Tgl. Einnahme 11 – 54 g. Prävalenz Dosisabhängig. 53% bei 25 g Fruktose. 73% bei 50 g Fruktose. Die Bedeutung der Intestinalen Fruktoseintoleranz hat in der Vergangenheit zugenommen, da sich die Menge an Fructose in der Nahrung in den letzten Jahren durch industriell bereitgestellte Süßungsmittel dramatisch erhöht hat.[1] Schätzungen der Verbreitung gehen von bis zu 30 % der Gesamtbevölkerung in westlichen Ländern und Afrika aus und deuten eine mit 10 % der Bevölkerung geringere Verbreitung in Asien an. Fructose malabsorption may be reduced by regarding it not as an abnormality but as a physiological process offering an opportunity to improve functional. gastrointestinal symptoms by dietary change. Süssgetränke! SGLT1: Sodium/Glc/Galact Cotransporter. GLUT2: Fakultativ, Glc / Fruct / Galact, hohe Kapazität. GLUT5: Fakultativ, fructosespezifisch, niedrige Kapazität. Skoog SM, Bharucha AE. Am J Gastroenterol. 2004;99: Beyer PL et al. J Am Diet Assoc, 2005;105: P. Gibson et al, Aliment Pharmacol Ther 2006; 25, Referent / Bereich")
18
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Keine Dünndarmhydro-lase; Absorption < 5% Raffinose, Stachyose Fructose: absorbiert mit Glucose oder als Sucrose (Glucose mit Fructose) ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. a low absorptive capacity of the small intestinal epithelium rapid transit through the small bowel SIBO Anderer Transporter wenn Glc unabhängig. GLUT 5 vs GLUT 2 Transporter Absorptionskapazität limitiert wenn in Exzess zu Glucose vorhanden; 30% Malabsorption Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
 ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. a low absorptive capacity of the small intestinal epithelium. rapid transit through the small bowel. SIBO. Anderer Transporter wenn Glc unabhängig. GLUT 5 vs GLUT 2 Transporter. Absorptionskapazität limitiert wenn in Exzess zu Glucose vorhanden; 30% Malabsorption. Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich")
19
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Raffinose, Stachyose Fructose: absorbiert mit Glucose oder als Sucrose (Glucose mit Fructose) ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose Stachyose: Glucose-Fructose, 2 Galactose Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten >10 Einheiten: Inuline Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
 ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose. Stachyose: Glucose-Fructose, 2 Galactose. Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten. >10 Einheiten: Inuline. Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien. Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten. Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich")
20
Thema / Bereich / Anlass
Galactane Speicherkohlenhydrat: wasserlöslicher Polysaccharide, die zu den Hemicellulose gehören und hauptsächlich aus D-Galactose bestehen Raffinose: Trisaccharid: Galactose, Glucose, Fructose Stachyose: Tetrasaccharid: Raffinose + Galactose Hülsenfrüchte Nicht GOS Gibson P et al. Aliment Pharmacol 2006 Referent / Bereich

21
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Keine α-Galactosidase, minimale Absorption Raffinose, Stachyose Fructose: absorbiert mit Glucose oder als Sucrose (Glucose mit Fructose) ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose Stachyose: Glucose-Fructose, 2 Galactose Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten >10 Einheiten: Inuline Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
 ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose. Stachyose: Glucose-Fructose, 2 Galactose. Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten. >10 Einheiten: Inuline. Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien. Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten. Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich")
22
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Raffinose, Stachyose Fructose: absorbiert mit Glucose oder als Sucrose (Glucose mit Fructose) ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose Stachyose: Glucose-Fructose, 2 Galactose Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten >10 Einheiten: Inuline Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
 ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose. Stachyose: Glucose-Fructose, 2 Galactose. Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten. >10 Einheiten: Inuline. Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien. Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten. Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich")
23
Thema / Bereich / Anlass
Polyole Sorbitol, Xylotol, Mannitol, Maltitol Natürlich vorkommend in versch. Früchten / Gemüsen industriell hergestellt aus Mais-/Weizenstärke E Stoffe ( E420, E967, E421, E965) Zahnfreundliche Zuckeraustauschstoffe Polyalkohole – Zuckeralkohol In Bonbons / Kaugummis Gibson P et al. Aliment Pharmacol 2006 Referent / Bereich
 Zahnfreundliche Zuckeraustauschstoffe. Polyalkohole – Zuckeralkohol. In Bonbons / Kaugummis. Gibson P et al. Aliment Pharmacol Referent / Bereich")
24
Thema / Bereich / Anlass
Was sind FODMAP’s Oligosaccharide Fructane Galaktane Fructooligosaccharide Inulin Disaccharide Laktose Monosaccharide Fruktose Polyole Sorbitol, Xylotol, Mannitol, Maltitol Raffinose, Stachyose Fructose: absorbiert mit Glucose oder als Sucrose (Glucose mit Fructose) ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose Stachyose: Glucose-Fructose, 2 Galactose Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten >10 Einheiten: Inuline Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten Nur passive Absorption < 20% Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich
 ca 85%. Freie Fructose kann nur reduziert mittels Glucose-unabhängigem Transporter aufgenommen werden. Ca. 30% der Bevölkerung hat eine stark limitierte Fähigkeit, Glucose aufzunehmen. Galactane: verzweigter, wasserlöslicher Polysaccharide, die zu den Hemicellulosen gehören und hauptsächlich aus D-Galactose. Stachyose: Glucose-Fructose, 2 Galactose. Fructane: Oligo / Polysaccharide mit Fructoseeinheiten und einem Glucoseende. Inuline. FOS < 10 Einheiten. >10 Einheiten: Inuline. Dietary Fructane are mostly FOS (wheat and onion) FOS/Inulin Nahrungsergänzungmittel als gesundheitsfördernd. Lactasemangel: 2% Scandinavien vs > 90% in Asien. Polyole: Zuckeralkohole: Früchten (Aepfel, Birnen, Steinfrüchte, künstl. Süssstoffe) GOS: Cooking reduces the GOS content. Raffinose: Fructose-Glucose-Galactose: in Hülsenfrüchten. Nur passive Absorption < 20% Gibson PR, Shepherd SJ Aliment Pharmacol Ther. 2005;21(12): Referent / Bereich")
25
Nahrungsmittel mit hohem FODMAP Gehalt
Thema / Bereich / Anlass Nahrungsmittel mit hohem FODMAP Gehalt Oligosaccharide Disaccharide Monosacharide Polyole Fruktane Galaktane Laktose Fruktose Früchte / Gemüse Süssstoffe Gemüse: Artischocke, Fenchel, Knoblauch, Kohl, Lauch, Randen, Rosenkohl, Spargel, Zwiebeln Getreide: Roggen, Weizen Gerste Früchte: Khaki , Nektarinen, weisse Pfirsich Wassermelone Hülsenfrüchte rote / weisse Bohnen , Kichererbsen, Linsen Milch, Joghurt, Glacé, Ricotta, Hüttenkäse Früchte: Äpfel, Birnen, Feigen Mango, Kirschen Konservenfrüchte Trockenfrüchte Wassermelone Süssstoff Fruktose Honig Äpfel Aprikosen Birnen Kirschen Nektarinen Pfirsich Pflaume Wassermelone Zwetschge Gemüse: Blumenkohl grüne Peperoni Pilze Isomalt, Mannit, Sorbit, Xylit Weizen, Dinkel, Roggen, Kamut, Emmer, Einkorn und Hartweizen. Hafer und Gerste haben einen niedrigen Anteil an Klebereiweiß Referent / Bereich

26
Nahrungsmittel mit niedrigem FODMAP Gehalt
Thema / Bereich / Anlass Nahrungsmittel mit niedrigem FODMAP Gehalt Früchte Gemüse Milchprodukte Getreide Weitere Ananas Banane Blaubeeren Datteln Erdbeeren Grapefruit Heidelbeeren Himbeeren Honigmelone Kiwi Mandarinen Orangen Papaya Passionsfrucht Rhabarber Trauben Zitrone Aubergine Blattsalat grüne Bohnen Chinakohl Endivien Frühlingszwie-bel grüner T. Gurke Karotten Kartoffeln Knollensellerie Kohlrabi Kürbis Mangold Pastinake Peperoni Schnittlauch Spinat Tomaten Zucchetti Lactosefreie Milch Lactosefreie Joghurt Hartkäse Brie Camembert Sorbet Cornflakes Glutenfreie Getreide Buchweizen Hafer Haferflocken Hirse Mais Maiswaffeln Marroni Quinoa Reis Reiswaffeln Reisnudeln Tapioka Süssstoffe: Ahornsirup Traubenzucker Zucker Proteine: Eier Fisch Fleisch Poulet Tofu Citrus / Südfrüchte aber auch Beeren Referent / Bereich

27
Praktische Umsetzung FODMAP Konzept
Thema / Bereich / Anlass Praktische Umsetzung FODMAP Konzept Restriktionsphase: für mindestens zwei Monate soll auf FODMAP reiche Nahrungsmittel verzichtet werden Falls keine Fructose- / Lactosemalabsorption besteht, muss nur auf die restlichen FODMAP reichen Nahrungsmittel verzichtet werden Graduelle Reexposition FODMAP reicher Nahrungsmittel nach 2 Monaten: Austestung individueller Toleranz Unter ERB Beratung. Kommt es während der 1. Phase zu einer Verbesserung der Symptomatik kann nach zwei Monaten begonnen werden, FODMAP-reiche Lebensmittel langsam wieder einzuführen. Ziel der 2. Phase ist es, die individuelle Toleranzgrenze zu bestimmen. Dabei soll pro Woche ein FODMAP Nahrungsmittel mit normaler Portionengrösse wieder eingenommen werden (mindestens 2x während der Testwoche). Falls keine Symptome auftreten, kann mit anderen Nahrungsmitteln aus derselben FODMAP Gruppe weitergefahren werden (höhere Zufuhr gleicher FODMAPs, erhöhte Toleranzgrenze?), oder es kann mit einer anderen FODMAP Gruppe weitergefahren und die Mengenzufuhr der 1. FODMAP-Gruppe beibehalten werden. Falls Symptome bei Reexposition auftreten, soll bis zur Symptomenfreiheit abgewartet werden. Dann kann die Portionengrösse reduziert und erneute getestet werden. Falls ein spezifisches FODMAP Nahrungsmittel ein Problem darstellt, soll ein anderes Nahrungsmittel aus derselben FODMAP Gruppe getestet werden um die Unverträglichkeit der FODMAP Gruppe zu verifizieren. Da sich die Sensitivität im Verlaufe ändern kann, sollte auch zu einem späteren Zeitpunkt ein Reexpositionsversuch gewagt werden. Die FODMAP arme Ernährung ruft bei ¾ aller Patienten eine deutliche Beschwerdelinderung hervor. Bei Therapieversagern ist die Adhärenz meist ungenügend. Verbesserung bei ¾ aller Patienten. Versagen: fehlende Therapieadhärenz The complete Low-FODMAP- Diet. Shepert S and Gibson P. The Experiment – New York, August 2013. Referent / Bereich
. Falls keine Symptome auftreten, kann mit anderen Nahrungsmitteln aus derselben FODMAP Gruppe weitergefahren werden (höhere Zufuhr gleicher FODMAPs, erhöhte Toleranzgrenze ), oder es kann mit einer anderen FODMAP Gruppe weitergefahren und die Mengenzufuhr der 1. FODMAP-Gruppe beibehalten werden. Falls Symptome bei Reexposition auftreten, soll bis zur Symptomenfreiheit abgewartet werden. Dann kann die Portionengrösse reduziert und erneute getestet werden. Falls ein spezifisches FODMAP Nahrungsmittel ein Problem darstellt, soll ein anderes Nahrungsmittel aus derselben FODMAP Gruppe getestet werden um die Unverträglichkeit der FODMAP Gruppe zu verifizieren. Da sich die Sensitivität im Verlaufe ändern kann, sollte auch zu einem späteren Zeitpunkt ein Reexpositionsversuch gewagt werden. Die FODMAP arme Ernährung ruft bei ¾ aller Patienten eine deutliche Beschwerdelinderung hervor. Bei Therapieversagern ist die Adhärenz meist ungenügend. Verbesserung bei ¾ aller Patienten. Versagen: fehlende Therapieadhärenz. The complete Low-FODMAP- Diet. Shepert S and Gibson P. The Experiment – New York, August Referent / Bereich")
28
Thema / Bereich / Anlass
Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management Shepherd SJ, Gibson PR Department of Gastroenterology and Monash University, Victoria, Australia J Am Diet Assoc. 2006;106(10): Referent / Bereich
: Referent / Bereich")
29
Outcome Fruktosearme Diät in Fructosemalabsorption
Thema / Bereich / Anlass Outcome Fruktosearme Diät in Fructosemalabsorption 62 IBS Pat mit Fruktose MA im H2 Atemtest 48 (77%) adhered to diet 14 did not adhere to diet 41 (85%) Improved 7 (15%) No improvement 5 (36%) 9 (64%) Ernährungsberatung Dietary fructose induces abdominal symptoms in patients with fructose malabsorption, but there are no published guidelines on its dietary management. The objective was to retrospectively evaluate a potentially successful diet therapy in patients with irritable bowel syndrome and fructose malabsorption. Tables detailing the content of fructose and fructans in foods were constructed. A dietary strategy comprising avoidance of foods containing substantial free fructose and short-chain fructans, limitation of the total dietary fructose load, encouragement of foods in which glucose was balanced with fructose, and co-ingestion of free glucose to balance excess free fructose was devised. Sixty-two consecutively referred patients with irritable bowel syndrome and fructose malabsorption on breath hydrogen testing underwent dietary instruction. Dietary adherence and effect on abdominal symptoms were evaluated via telephone interview 2 to 40 months (median 14 months) later. Response to the diet was defined as improvement of all symptoms by at least 5 points on a -10- to 10-point scale. Forty-eight patients (77%) adhered to the diet always or frequently. Forty-six (74%) of all patients responded positively in all abdominal symptoms. Positive response overall was significantly better in those adherent than nonadherent (85% vs 36%; P<0.01), as was improvement in individual symptoms (P<0.01 for all symptoms). This comprehensive fructosemalabsorption dietary therapy achieves a high level of sustained adherence and good symptomatic response. Shepherd SJ, Gibson PR. Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management J Am Diet Assoc. 2006;106(10): Referent / Bereich
 adhered to diet. 14 did not adhere to diet. 41 (85%) Improved. 7 (15%) No improvement. 5 (36%) 9 (64%) Ernährungsberatung. Dietary fructose induces abdominal symptoms in patients with fructose malabsorption, but there are no published guidelines on its dietary management. The objective was to retrospectively evaluate a potentially successful diet therapy in patients with irritable bowel syndrome and fructose malabsorption. Tables detailing the content of fructose and fructans in foods were constructed. A dietary strategy comprising avoidance of foods containing substantial free fructose and short-chain fructans, limitation of the total dietary fructose load, encouragement of foods in which glucose was balanced with fructose, and co-ingestion of free glucose to balance excess free fructose was devised. Sixty-two consecutively referred patients with irritable bowel syndrome and fructose malabsorption on breath hydrogen testing underwent dietary instruction. Dietary adherence and effect on abdominal symptoms were evaluated via telephone interview 2 to 40 months (median 14 months) later. Response to the diet was defined as improvement of all symptoms by at least 5 points on a -10- to 10-point scale. Forty-eight patients (77%) adhered to the diet always or frequently. Forty-six (74%) of all patients responded positively in all abdominal symptoms. Positive response overall was significantly better in those adherent than nonadherent (85% vs 36%; P<0.01), as was improvement in individual symptoms (P<0.01 for all symptoms). This comprehensive fructosemalabsorption dietary therapy achieves a high level of sustained adherence and good symptomatic response. Shepherd SJ, Gibson PR. Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management J Am Diet Assoc. 2006;106(10): Referent / Bereich")
30
Thema / Bereich / Anlass
BACKGROUND & AIMS Observational studies suggest dietary fructose restriction might lead to sustained symptomatic response in patients with irritable bowel syndrome (IBS) and fructose malabsorption. The aims of this study were first to determine whether the efficacy of this dietary change is due to dietary fructose restriction and second to define whether symptom relief was specific to free fructose or to poorly absorbed short-chain carbohydrates in general. METHODS The double-blinded, randomized, quadruple arm, placebo-controlled rechallenge trial took place in the general community. The 25 patients who had responded to dietary change were provided all food, low in free fructose and fructans, for the duration of the study. Patients were randomly challenged by graded dose introduction of fructose, fructans, alone or in combination, or glucose taken as drinks with meals for maximum test period of 2 weeks, with at least 10-day washout period between. For the main outcome measures, symptoms were monitored by daily diary entries and responses to a global symptom question. RESULTS 70% of patients receiving fructose, 77% receiving fructans, and 79% receiving a mixture reported symptoms were not adequately controlled, compared with 14% receiving glucose (P < or = 0.002, McNemar test). Similarly, the severity of overall and individual symptoms was significantly and markedly less for glucose than other substances. Symptoms were induced in a dose-dependent manner and mimicked previous IBS symptoms. CONCLUSIONS: In patients with IBS and fructose malabsorption, dietary restriction of fructose and/or fructans is likely to be responsible for symptomatic improvement, suggesting efficacy is due to restriction of poorly absorbed short-chain carbohydrates in general Dietary Triggers of Abdominal Symptoms in Patients With Irritable Bowel Syndrome: Randomized Placebo-Controlled Evidence Shepherd SJ, Parker FC, Muir JG, Gibson PR Department of Gastroenterology and Monash University Department of Medicine, Box Hill Hospital, Victoria, Australia Clin Gastroenterol Hepatol. 2008;6(7):765-71 Referent / Bereich
 and fructose malabsorption. The aims of this study were first to determine whether the efficacy of this dietary change is due to dietary fructose restriction and second to define whether symptom relief was specific to free fructose or to poorly absorbed short-chain carbohydrates in general. METHODS The double-blinded, randomized, quadruple arm, placebo-controlled rechallenge trial took place in the general community. The 25 patients who had responded to dietary change were provided all food, low in free fructose and fructans, for the duration of the study. Patients were randomly challenged by graded dose introduction of fructose, fructans, alone or in combination, or glucose taken as drinks with meals for maximum test period of 2 weeks, with at least 10-day washout period between. For the main outcome measures, symptoms were monitored by daily diary entries and responses to a global symptom question. RESULTS 70% of patients receiving fructose, 77% receiving fructans, and 79% receiving a mixture reported symptoms were not adequately controlled, compared with 14% receiving glucose (P < or = 0.002, McNemar test). Similarly, the severity of overall and individual symptoms was significantly and markedly less for glucose than other substances. Symptoms were induced in a dose-dependent manner and mimicked previous IBS symptoms. CONCLUSIONS: In patients with IBS and fructose malabsorption, dietary restriction of fructose and/or fructans is likely to be responsible for symptomatic improvement, suggesting efficacy is due to restriction of poorly absorbed short-chain carbohydrates in general. Dietary Triggers of Abdominal Symptoms in Patients With Irritable Bowel Syndrome: Randomized Placebo-Controlled Evidence Shepherd SJ, Parker FC, Muir JG, Gibson PR Department of Gastroenterology and Monash University Department of Medicine, Box Hill Hospital, Victoria, Australia Clin Gastroenterol Hepatol. 2008;6(7): Referent / Bereich")
31
Symptomkontrolle: Reexposition nach FODMAP Diät
Thema / Bereich / Anlass Symptomkontrolle: Reexposition nach FODMAP Diät Balken weiss ITT, in schwarz PP Intention to treat Per protocol «Waren ihre Symptome innerhalb der letzten Testphase adäquat kontrolliert?» Shepherd SJ, Parker SC, Muir JG, Gibson PR. Dietary Triggers of Abdominal Symptoms in Patients With Irritable Bowel Syndrome: Randomized Placebo-Controlled Evidence Clin Gastroenterol Hepatol. 2008;6(7): Referent / Bereich
: Referent / Bereich")
32
Symptomkontrolle: Reexpostion nach FODMAP Diät
Thema / Bereich / Anlass Symptomkontrolle: Reexpostion nach FODMAP Diät Symptomschwere für low-dose Exposition (weisse Boxen) verglichen mit high dose (schwarze Boxen) Shepherd SJ, Parker SC, Muir JG, Gibson PR. Dietary Triggers of Abdominal Symptoms in Patients With Irritable Bowel Syndrome: Randomized Placebo-Controlled Evidence Clin Gastroenterol Hepatol. 2008;6(7): . Referent / Bereich
 verglichen mit high dose (schwarze Boxen) Shepherd SJ, Parker SC, Muir JG, Gibson PR. Dietary Triggers of Abdominal Symptoms in Patients With Irritable Bowel Syndrome: Randomized Placebo-Controlled Evidence Clin Gastroenterol Hepatol. 2008;6(7): Referent / Bereich")
33
Thema / Bereich / Anlass
BACKGROUND & AIMS: Patients with non-celiac gluten sensitivity (NCGS) do not have celiac disease but their symptoms improve when they are placed on gluten-free diets. We investigated the specific effects of gluten after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates (fermentable, oligo-, di-, monosaccharides, and polyols [FODMAPs]) in subjects believed to have NCGS. METHODS: We performed a double-blind cross-over trial of 37 subjects (aged y, 6 men) with NCGS and irritable bowel syndrome (based on Rome III criteria), but not celiac disease. Participants were randomly assigned to groups given a 2-week diet of reduced FODMAPs, and were then placed on high-gluten (16 g gluten/d), low-gluten (2 g gluten/d and 14 g whey protein/d), or control (16 g whey protein/d) diets for 1 week, followed by a washout period of at least 2 weeks. We assessed serum and fecal markers of intestinal inflammation/injury and immune activation, and indices of fatigue. Twenty-two participants then crossed over to groups given gluten (16 g/d), whey (16 g/d), or control (no additional protein) diets for 3 days. Symptoms were evaluated by visual analogue scales. RESULTS: In all participants, gastrointestinal symptoms consistently and significantly improved during reduced FODMAP intake, but significantly worsened to a similar degree when their diets included gluten or whey protein. Gluten-specific effects were observed in only 8% of participants. There were no diet-specific changes in any biomarker. During the 3-day rechallenge, participants' symptoms increased by similar levels among groups. Gluten-specific gastrointestinal effects were not reproduced. An order effect was observed. CONCLUSIONS: In a placebo-controlled, cross-over rechallenge study, we found no evidence of specific or dose-dependent effects of gluten in patients with NCGS placed diets low in FODMAPs No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates Biesiekierskis JR, Peters SL, Newnham ED, Rosella O, Muir JG, Gibson PR Department of Gastroenterology, Eastern Health Clinical School, Monash University, Box Hill, Victoria, Australia Gastroenterology 2013;145:320-8 Referent / Bereich
 do not have celiac disease but their symptoms improve when they are placed on gluten-free diets. We investigated the specific effects of gluten after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates (fermentable, oligo-, di-, monosaccharides, and polyols [FODMAPs]) in subjects believed to have NCGS. METHODS: We performed a double-blind cross-over trial of 37 subjects (aged y, 6 men) with NCGS and irritable bowel syndrome (based on Rome III criteria), but not celiac disease. Participants were randomly assigned to groups given a 2-week diet of reduced FODMAPs, and were then placed on high-gluten (16 g gluten/d), low-gluten (2 g gluten/d and 14 g whey protein/d), or control (16 g whey protein/d) diets for 1 week, followed by a washout period of at least 2 weeks. We assessed serum and fecal markers of intestinal inflammation/injury and immune activation, and indices of fatigue. Twenty-two participants then crossed over to groups given gluten (16 g/d), whey (16 g/d), or control (no additional protein) diets for 3 days. Symptoms were evaluated by visual analogue scales. RESULTS: In all participants, gastrointestinal symptoms consistently and significantly improved during reduced FODMAP intake, but significantly worsened to a similar degree when their diets included gluten or whey protein. Gluten-specific effects were observed in only 8% of participants. There were no diet-specific changes in any biomarker. During the 3-day rechallenge, participants symptoms increased by similar levels among groups. Gluten-specific gastrointestinal effects were not reproduced. An order effect was observed. CONCLUSIONS: In a placebo-controlled, cross-over rechallenge study, we found no evidence of specific or dose-dependent effects of gluten in patients with NCGS placed diets low in FODMAPs. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates Biesiekierskis JR, Peters SL, Newnham ED, Rosella O, Muir JG, Gibson PR Department of Gastroenterology, Eastern Health Clinical School, Monash University, Box Hill, Victoria, Australia Gastroenterology 2013;145: Referent / Bereich")
34
Non-Celiac Gluten Sensitivity und FODMAP
Thema / Bereich / Anlass Non-Celiac Gluten Sensitivity und FODMAP Individual responses in mean overall symptom severity score during the run-in period, where low FODMAP diet was commenced, compared with the baseline period, where participant’s usual gluten-free diet was consumed during 7-day trial. Scores were significantly greater during the baseline period (P < .0001, Wilcoxon signed rank test). glutenfreier Diät low FODMAP Diät Biesiekierski et al. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates Gastroenterology 2013 Referent / Bereich
. glutenfreier Diät low FODMAP Diät. Biesiekierski et al. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates Gastroenterology Referent / Bereich")
35
Non-Celiac Gluten Sensitivity und FODMAP
Thema / Bereich / Anlass Non-Celiac Gluten Sensitivity und FODMAP Gluten Specific effects in only 3 (8%) patients! Whey Milchserum inkl. Lactose Biesiekierski et al. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates Gastroenterology 2013 Referent / Bereich
 patients! Whey Milchserum inkl. Lactose. Biesiekierski et al. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates Gastroenterology Referent / Bereich")
36
Thema / Bereich / Anlass
BACKGROUND: Emerging evidence indicates that the consumption of FODMAPs may result in symptoms in some patients with irritable bowel syndrome (IBS). The present study aimed to determine whether a low FODMAP diet is effective for symptom control in patients with IBS and to compare its effects with those of standard dietary advice based on the UK National Institute for Health and Clinical Excellence (NICE) guidelines. METHODS: Consecutive patients with IBS who attended a follow-up dietetic outpatient visit for dietary management of their symptoms were included. Questionnaires were completed for patients who received standard (n = 39) or low FODMAP dietary advice (n = 43). Data were recorded on symptom change and comparisons were made between groups. RESULTS: more patients in the low FODMAP group reported satisfaction with their symptom response (76%) standard g(54%, P = 0.038). Composite symptom score data showed better overall symptom response in the low FODMAP group (86%) standard g (49%, P < 0.001). Significantly more patients in the low FODMAP group reported improvements in bloating (low FODMAP 82% vs standard 49%, P = 0.002), abdominal pain (low FODMAP 85% vs standard 61%, P = 0.023) and flatulence (low FODMAP 87% vs standard 50%, P = 0.001). CONCLUSIONS: A low FODMAP diet appears to be more effective than standard dietary advice for symptom control in IBS. Comparison of symptom response following advice for a low FODMAP vs standard dietary advice in patients with irritable bowel syndrome Staudacher HM, Whelan K, Irving PM, Lomer MC King's College London, Nutritional Sciences Division, London, UK J Hum Nutr Diet. 2011;24(5): Referent / Bereich
. The present study aimed to determine whether a low FODMAP diet is effective for symptom control in patients with IBS and to compare its effects with those of standard dietary advice based on the UK National Institute for Health and Clinical Excellence (NICE) guidelines. METHODS: Consecutive patients with IBS who attended a follow-up dietetic outpatient visit for dietary management of their symptoms were included. Questionnaires were completed for patients who received standard (n = 39) or low FODMAP dietary advice (n = 43). Data were recorded on symptom change and comparisons were made between groups. RESULTS: more patients in the low FODMAP group reported satisfaction with their symptom response (76%) standard g(54%, P = 0.038). Composite symptom score data showed better overall symptom response in the low FODMAP group (86%) standard g (49%, P < 0.001). Significantly more patients in the low FODMAP group reported improvements in bloating (low FODMAP 82% vs standard 49%, P = 0.002), abdominal pain (low FODMAP 85% vs standard 61%, P = 0.023) and flatulence (low FODMAP 87% vs standard 50%, P = 0.001). CONCLUSIONS: A low FODMAP diet appears to be more effective than standard dietary advice for symptom control in IBS. Comparison of symptom response following advice for a low FODMAP vs standard dietary advice in patients with irritable bowel syndrome Staudacher HM, Whelan K, Irving PM, Lomer MC King s College London, Nutritional Sciences Division, London, UK J Hum Nutr Diet. 2011;24(5): Referent / Bereich")
37
Have regular meals and take time to eat.
Avoid missing meals or leaving long gaps between eating Drink at least 8 cups of fluid per day, esp water / herbal teas. Restrict tea and coffee to 3 cups per day. Reduce intake of alcohol and fizzy drinks. Consider limiting intake of high-fibre food (wholemeal / high-fibre flour / breads, cereals high in bran, and whole grains such as brown rice). Reduce intake of 'resistant starch' (starch that resists digestion in the small intestine and reaches the colon intact), often found in processed or re-cooked foods. Limit fresh fruit to 3 portions (of 80 g each) per day. For diarrhoea, avoid sorbitol, an artificial sweetener found in sugar-free sweets (including chewing gum) and drinks, and in some diabetic and slimming products. For wind and bloating consider increasing intake of oats (for example, oat-based breakfast cereal or porridge) and linseeds (up to 1 tablespoon per day). Review the person's fibre intake and adjust (usually reduce) according to symptoms. Discourage intake of insoluble fibre (for example, bran). If more fibre is needed, recommend soluble fibre such as ispaghula powder, or foods high in soluble fibre (for example, oats). If the person wants to try probiotics, advise them to take the dose recommended by the manufacturer for at least 4 weeks while monitoring the effect.
. Reduce intake of resistant starch (starch that resists digestion in the small intestine and reaches the colon intact), often found in processed or re-cooked foods. Limit fresh fruit to 3 portions (of 80 g each) per day. For diarrhoea, avoid sorbitol, an artificial sweetener found in sugar-free sweets (including chewing gum) and drinks, and in some diabetic and slimming products. For wind and bloating consider increasing intake of oats (for example, oat-based breakfast cereal or porridge) and linseeds (up to 1 tablespoon per day). Review the person s fibre intake and adjust (usually reduce) according to symptoms. Discourage intake of insoluble fibre (for example, bran). If more fibre is needed, recommend soluble fibre such as ispaghula powder, or foods high in soluble fibre (for example, oats). If the person wants to try probiotics, advise them to take the dose recommended by the manufacturer for at least 4 weeks while monitoring the effect.")
38
Low FODMAP versus Standard ERB
Thema / Bereich / Anlass Low FODMAP versus Standard ERB Have regular meals and take time to eat. Avoid missing meals or leaving long gaps between eating Drink at least 8 cups of fluid per day, especially water or other non-caffeinated drinks such as herbal teas. Restrict tea and coffee to 3 cups per day. Reduce intake of alcohol and fizzy drinks. Consider limiting intake of high-fibre food (for example, wholemeal or high-fibre flour and breads, cereals high in bran, and whole grains such as brown rice). Reduce intake of 'resistant starch' (starch that resists digestion in the small intestine and reaches the colon intact), often found in processed or re-cooked foods. Limit fresh fruit to 3 portions (of 80 g each) per day. For diarrhoea, avoid sorbitol, an artificial sweetener found in sugar-free sweets (including chewing gum) and drinks, and in some diabetic and slimming products. For wind and bloating consider increasing intake of oats (for example, oat-based breakfast cereal or porridge) and linseeds (up to 1 tablespoon per day). Review the person's fibre intake and adjust (usually reduce) according to symptoms. Discourage intake of insoluble fibre (for example, bran). If more fibre is needed, recommend soluble fibre such as ispaghula powder, or foods high in soluble fibre (for example, oats). If the person wants to try probiotics, advise them to take the dose recommended by the manufacturer for at least 4 weeks while monitoring the effect. % Verbesserung von Symptom Scores für Patienten die 4 Wochen eine FODMAP-arme versus Standard ERB erhielten Staudacher et al. Comparison of symptom response following advice for a low FODMAP vs standard dietary advice in patients with irritable bowel syndrome J Hum Nutr Diet. 2011;24(5): Referent / Bereich
. Reduce intake of resistant starch (starch that resists digestion in the small intestine and reaches the colon intact), often found in processed or re-cooked foods. Limit fresh fruit to 3 portions (of 80 g each) per day. For diarrhoea, avoid sorbitol, an artificial sweetener found in sugar-free sweets (including chewing gum) and drinks, and in some diabetic and slimming products. For wind and bloating consider increasing intake of oats (for example, oat-based breakfast cereal or porridge) and linseeds (up to 1 tablespoon per day). Review the person s fibre intake and adjust (usually reduce) according to symptoms. Discourage intake of insoluble fibre (for example, bran). If more fibre is needed, recommend soluble fibre such as ispaghula powder, or foods high in soluble fibre (for example, oats). If the person wants to try probiotics, advise them to take the dose recommended by the manufacturer for at least 4 weeks while monitoring the effect. % Verbesserung von Symptom Scores für Patienten die 4 Wochen eine FODMAP-arme versus Standard ERB erhielten. Staudacher et al. Comparison of symptom response following advice for a low FODMAP vs standard dietary advice in patients with irritable bowel syndrome J Hum Nutr Diet. 2011;24(5): Referent / Bereich")
39
Thema / Bereich / Anlass
BACKGROUND & AIMS: A diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) often is used to manage functional gastrointestinal symptoms in patients with irritable bowel syndrome (IBS), yet there is limited evidence of its efficacy, compared with a normal Western diet. We investigated the effects of a diet low in FODMAPs compared with an Australian diet, in a randomized, controlled, single-blind, cross-over trial of patients with IBS. METHODS: In a study of 30 patients with IBS and 8 healthy individuals (controls, matched for demographics and diet), we collected dietary data from subjects for 1 habitual week. Participants then randomly were assigned to groups that received 21 days of either a diet low in FODMAPs or a typical Australian diet, followed by a washout period of at least 21 days, before crossing over to the alternate diet. Daily symptoms were rated using a 0- to 100-mm visual analogue scale. Almost all food was provided during the interventional diet periods, with a goal of less than 0.5 g intake of FODMAPsper meal for the low-FODMAP diet. All stools were collected from days and assessed for frequency, weight, water content, and King's Stool Chart rating. RESULTS: Subjects with IBS had lower overall gastrointestinal symptom scores (22.8; 95% confidence interval, mm) while on a diet low inFODMAPs, compared with the Australian diet (44.9; 95% confidence interval, mm; P < .001) and the subjects' habitual diet. Bloating, pain, and passage of wind also were reduced while IBS patients were on the low-FODMAP diet. Symptoms were minimal and unaltered by either dietamong controls. Patients of all IBS subtypes had greater satisfaction with stool consistency while on the low-FODMAP diet, but diarrhea-predominant IBS was the only subtype with altered fecal frequency and King's Stool Chart scores. CONCLUSIONS: In a controlled, cross-over study of patients with IBS, a diet low in FODMAPs effectively reduced functional gastrointestinalsymptoms. This high-quality evidence supports its use as a first-line therapy. A Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome Emma P. Halmos, Victoria A. Power, Susan J. Shepherd, Peter R. Gibson, Jane G. Muir Department of Medicine, Eastern Health Clinical School, Monash University, Box Hill, Victoria, Australia; Department of Gastroenterology, Central Clinical School, Monash University, Melbourne, Victoria, Australia Gastroenterology 2014 Jan;146(1):67-75 Referent / Bereich
 often is used to manage functional gastrointestinal symptoms in patients with irritable bowel syndrome (IBS), yet there is limited evidence of its efficacy, compared with a normal Western diet. We investigated the effects of a diet low in FODMAPs compared with an Australian diet, in a randomized, controlled, single-blind, cross-over trial of patients with IBS. METHODS: In a study of 30 patients with IBS and 8 healthy individuals (controls, matched for demographics and diet), we collected dietary data from subjects for 1 habitual week. Participants then randomly were assigned to groups that received 21 days of either a diet low in FODMAPs or a typical Australian diet, followed by a washout period of at least 21 days, before crossing over to the alternate diet. Daily symptoms were rated using a 0- to 100-mm visual analogue scale. Almost all food was provided during the interventional diet periods, with a goal of less than 0.5 g intake of FODMAPsper meal for the low-FODMAP diet. All stools were collected from days and assessed for frequency, weight, water content, and King s Stool Chart rating. RESULTS: Subjects with IBS had lower overall gastrointestinal symptom scores (22.8; 95% confidence interval, mm) while on a diet low inFODMAPs, compared with the Australian diet (44.9; 95% confidence interval, mm; P < .001) and the subjects habitual diet. Bloating, pain, and passage of wind also were reduced while IBS patients were on the low-FODMAP diet. Symptoms were minimal and unaltered by either dietamong controls. Patients of all IBS subtypes had greater satisfaction with stool consistency while on the low-FODMAP diet, but diarrhea-predominant IBS was the only subtype with altered fecal frequency and King s Stool Chart scores. CONCLUSIONS: In a controlled, cross-over study of patients with IBS, a diet low in FODMAPs effectively reduced functional gastrointestinalsymptoms. This high-quality evidence supports its use as a first-line therapy. A Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome Emma P. Halmos, Victoria A. Power, Susan J. Shepherd, Peter R. Gibson, Jane G. Muir Department of Medicine, Eastern Health Clinical School, Monash University, Box Hill, Victoria, Australia; Department of Gastroenterology, Central Clinical School, Monash University, Melbourne, Victoria, Australia Gastroenterology 2014 Jan;146(1): Referent / Bereich")
40
Thema / Bereich / Anlass
Low FODMAP - IBS Design randomisiert kontrolliert crossover, einseitig verblindet Methods 30 IBS Patienten, 8 gesunde Probanden 3 Wochen FODMAP arme/ reiche Ernährung 3 Wochen washout Phase Tgl. GI-Symptome (VAS), Stuhlbewertung (Kings Stool Chart) Halmos et al. Gastroenterol 2014 Jan;146(1):67-75 Referent / Bereich
, Stuhlbewertung (Kings Stool Chart) Halmos et al. Gastroenterol 2014 Jan;146(1): Referent / Bereich")
41
FODMAP IBS Interventionsstudie: Resultate
Thema / Bereich / Anlass FODMAP IBS Interventionsstudie: Resultate Mean overall gastrointestinal symptoms from the (A) IBS cohort and the (B) healthy cohort using a VAS during baseline, low FODMAP and typical Australian diets. Symptoms improved significantly on low FODMAP compared with baseline and the typical Australian diet for the IBS cohort. No differences were observed between any of the diets in the healthy cohort. Patienten mit IBS profitieren von einer FODMAP armen Diät im Vergleich zu einer normalen westlichen Ernährung bzgl. ihrer gastrointestinalen Symptomatik deutlich Halmos et al. Gastroenterol 2014 Jan;146(1):67-75 Referent / Bereich
 IBS cohort and the (B) healthy cohort using a VAS during baseline, low FODMAP and typical Australian diets. Symptoms improved significantly on low FODMAP compared with baseline and the typical Australian diet for the IBS cohort. No differences were observed between any of the diets in the healthy cohort. Patienten mit IBS profitieren von einer FODMAP armen Diät im Vergleich zu einer normalen westlichen Ernährung bzgl. ihrer gastrointestinalen Symptomatik deutlich Halmos et al. Gastroenterol 2014 Jan;146(1): Referent / Bereich")
42
FODMAP Interventionsstudie
Thema / Bereich / Anlass FODMAP Interventionsstudie Results Tabelle Supplement 4. Median breath hydrogen from 12 midday until 8 pm taken at hourly intervals following a typical Australian diet and low FODMAP diet in all participants (n=28). Area under the curve indicates that less breath hydrogen was produced on the low FODMAP diet (Median (interquartile range): 22.8 ( ) ppm. 8 h) compared to the typical Australian diet (80.9 ( ) ppm. 8 h; P < 0.001; Wilcoxon signed rank Halmos Gastroenterol 2014 Jan;146(1):67-75 Referent / Bereich
. Area under the curve indicates that less breath hydrogen was produced on the low FODMAP diet (Median (interquartile range): 22.8 ( ) ppm. 8 h) compared to the typical Australian diet (80.9 ( ) ppm. 8 h; P < 0.001; Wilcoxon signed rank. Halmos Gastroenterol 2014 Jan;146(1): Referent / Bereich")
43
Evidenz IBS FODMAP - Metaanalyse
Thema / Bereich / Anlass Evidenz IBS FODMAP - Metaanalyse Re-Induktion von Fruktose / Fruktanen nach FODMAP armer Diät verschlimmert Blähungen, Flatulenz und Bauchschmerzen Hohe Dosen an Fruktanen, Galakto-Oligo-sachariden und Sorbit führen zu schwereren Blähungen bei IBS Hohe Fruktosedosen lösen mehr Blähungen bei Pat mit IBS und Fruktosemalabsorption aus scottish intercollegiate guidelines network McKenzie YA, British Dietetic Association evidence-based guidelines for the dietary management of irritable bowel syndrome in adults. J Hum Nutr Diet 2012; 25:260-74 Referent / Bereich

44
Literatur

45
Take home message FODMAPs sind kurzkettige nicht
resorbierte Kohlenhydrate → endoluminalen Wassereinstrom → erhöhter Gasproduktion führen → intestinalen Distension (Wind, Schmerz, Blähungen) → Veränderung der Motilität /erhöhte intestinale Permeabilität Bei motivierten Patienten kann eine FODMAP arme Ernährung kontrolliert durch eine Ernährungsberaterin durchgeführt werden
 → Veränderung der Motilität /erhöhte intestinale Permeabilität. Bei motivierten Patienten kann eine FODMAP arme Ernährung kontrolliert durch eine Ernährungsberaterin durchgeführt werden.")
46
Vielen Dank für Ihr Interesse

48
Thema / Bereich / Anlass
IBD und FODMAP Objective Functional gut symptoms are common in patients with inflammatory bowel disease (IBD). Since poorly absorbed, short-chain carbohydrates (FODMAPs) appear to play an important role in the induction of functional gut symptoms, we aimed to determine the effect of their dietary restriction on abdominal symptoms in patients with stable IBD and to examine factors associated with success of and adherence to the diet. Material and method 52 consecutive patients with Crohn's disease and 20 with ulcerative colitis who received dietary advice at least 3 months prior at a gastrointestinal dietetic service in Victoria, Australia, underwent a retrospective telephone questionnaire. Information gathered included patient demographics, recall of dietary advice, dietary adherence, and change in gastrointestinal symptoms. Results Up to 70% of patients were adherent to the diet. Approximately one in two patients responded (defined as improvement of at least 5 out of 10 in overall symptoms). Overall abdominal symptoms, abdominal pain, bloating, wind and diarrhoea improved in patients with Crohn's disease and ulcerative colitis (p<0.02 for all), but constipation did not. For Crohn's disease, efficacy was associated with dietary adherence (p= 0.033) and inefficacy with non-adherence (p=0.013). Sustained response was associated with post-secondary education and working 35 h per week or less (p<0.03). Conclusions These data suggest that reduction of FODMAP intake offers an efficacious strategy for patients with IBD who have concurrent functional gut symptoms. A controlled dietary intervention trial is indicated. Gearry RB, et al. The effect of reduction of poorly absorbed, highly fermentable short-chain carbohydrates (FODMAPs) on the symptoms of patients with inflammatory bowel disease (IBD). JCC. 2009;3(1):8-14 Referent / Bereich
. Since poorly absorbed, short-chain carbohydrates (FODMAPs) appear to play an important role in the induction of functional gut symptoms, we aimed to determine the effect of their dietary restriction on abdominal symptoms in patients with stable IBD and to examine factors associated with success of and adherence to the diet. Material and method. 52 consecutive patients with Crohn s disease and 20 with ulcerative colitis who received dietary advice at least 3 months prior at a gastrointestinal dietetic service in Victoria, Australia, underwent a retrospective telephone questionnaire. Information gathered included patient demographics, recall of dietary advice, dietary adherence, and change in gastrointestinal symptoms. Results. Up to 70% of patients were adherent to the diet. Approximately one in two patients responded (defined as improvement of at least 5 out of 10 in overall symptoms). Overall abdominal symptoms, abdominal pain, bloating, wind and diarrhoea improved in patients with Crohn s disease and ulcerative colitis (p<0.02 for all), but constipation did not. For Crohn s disease, efficacy was associated with dietary adherence (p= 0.033) and inefficacy with non-adherence (p=0.013). Sustained response was associated with post-secondary education and working 35 h per week or less (p<0.03). Conclusions. These data suggest that reduction of FODMAP intake offers an efficacious strategy for patients with IBD who have concurrent functional gut symptoms. A controlled dietary intervention trial is indicated. Gearry RB, et al. The effect of reduction of poorly absorbed, highly fermentable short-chain carbohydrates (FODMAPs) on the symptoms of patients with inflammatory bowel disease (IBD). JCC. 2009;3(1):8-14. Referent / Bereich")
50
Thema / Bereich / Anlass
Rom III Kriterien Wiederkehrende abdominelle Schmerzen / Unbehagen für mind. 3 Tage / Monat während der letzten 3 Monate verbunden mit ≥ zwei Symptome 1. Verbesserung nach Defäkation 2. Beginn assoziiert mit Veränderung der Stuhlfrequenz 3. Beginn assoziiert mit Veränderung der Stuhlkonsistenz Symptomenbeginn seit mind. 6 Monaten Referent / Bereich

51
Definition Reizdarm S 3 Leitlinien DGVS / DGNM
Thema / Bereich / Anlass Definition Reizdarm S 3 Leitlinien DGVS / DGNM Chronische (> 3 M) Beschwerden, die vom Arzt und Patienten auf den Darm bezogen werden und in der Regel mit Stuhlgangsveränderungen einhergehen Die Beschwerden sollen begründen, dass der Patient deswegen Hilfe sucht und/oder sich sorgt und so stark sein, dass die Lebensqualität relevant hierdurch beeinträchtigt ist Voraussetzung ist, dass keine für andere Krankheitsbilder charakteristische Veränderung vorliegt, welche wahrscheinlich für die Symptome verantwortlich ist Schweregrad wird berücksichtigt Blähungen, abdominelle Distension Layer P et al. S3-Leitlinie zur Definition. Z Gastroenterol 2011; 49: 237–293 Referent / Bereich
 Beschwerden, die vom Arzt und Patienten auf den Darm bezogen werden und in der Regel mit Stuhlgangsveränderungen einhergehen. Die Beschwerden sollen begründen, dass der Patient deswegen Hilfe sucht und/oder sich sorgt und so stark sein, dass die Lebensqualität relevant hierdurch beeinträchtigt ist. Voraussetzung ist, dass keine für andere Krankheitsbilder charakteristische Veränderung vorliegt, welche wahrscheinlich für die Symptome verantwortlich ist. Schweregrad wird berücksichtigt. Blähungen, abdominelle Distension. Layer P et al. S3-Leitlinie zur Definition. Z Gastroenterol 2011; 49: 237–293. Referent / Bereich")
52
Differentialdiagnosen Reizdarm
Thema / Bereich / Anlass Differentialdiagnosen Reizdarm Diarrhoe Infektös Zöliakie CED Mikroskop. Colitis Chron. Pankreatitis Hyperthreose Malabsorption Kolon -Ca Obstipation Hypothyreose Kolon-Ca Funktionelle / strukturelle Stuhlentlee-rungsstörung Schmerz Ulcus Mesent. Ischämie Endometriose Ovarial-Ca Dünndarm- Stenosen Meteorismus SIBO Referent / Bereich

53
Thema / Bereich / Anlass
Abklärung Reizdarm Basislabor Blutbild CRP Elektrolyte Creatinin Leber-/Pancreas Glucose U-Status Zusatz Labor TSH Stuhl Mikrobiologie Zöliakie Antikörper Calprotectin im Stuhl Pancreaselastase Lactasemangel Referent / Bereich

54
Thema / Bereich / Anlass
Abklärung Reizdarm Diagnostik Abdomensonographie Obere Panendoskopie Ileokoloskopie Gyn. Untersuch CAVE Alarmsypmtome Blut im Stuhl / Anämie Fieber Nächtliche Sz > 50 y Pos. FA Referent / Bereich

55
Workshop 3. Ernährungstipps ERB A. Niedermann 2. Fallbeispiele S. Sigrist, G. Bourgeois 1. PEG Handling J. Haarer Haus 08 2. STOCK Grosser Hörsaal Haus 20 1. STOCK

Ähnliche Präsentationen







 beschreibt die sofortige Wirkung der Lebensmittel auf den Blutzuckerverlauf. Der schnelle Anstieg des.>")











