Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
B3-Läsionen Ist eine operative Intervention immer nötig? C. Schumacher Brustzentrum St. Elisabeth-Krankenhaus

2
B-Klassifikation B1: nicht verwertbares oder ausschließlich normales Gewebe B2: benigne B3: benigne, aber mit unsicherem biologischen Potenzial B4: verdächtig auf Malignität B5: maligne

3
B3-Läsionen Flache epitheliale Atypie (FEA) Lobuläre Neoplasie (ALH/LCIS) Atypische duktale Hyperplasie (ADH) Radiäre Narbe, komplexe sklerosierende Läsion Papilläre Läsion Phylloides Tumor, zellreiches Fibroadenom
 Lobuläre Neoplasie (ALH/LCIS) Atypische duktale Hyperplasie (ADH) Radiäre Narbe, komplexe sklerosierende Läsion Papilläre Läsion Phylloides Tumor, zellreiches Fibroadenom")
4
B3-Läsionen: Bedeutung 1.Nicht obligatorische Präkanzerose, Indikator für ein erhöhtes ipsilaterales Mammakarzinomrisiko 2.Indikator für eine generell erhöhtes bilaterales Mammakarzinomrisiko 3. Indikator für ein benachbartes Karzinom

5
B3-Läsionen Datenlage: Häufigkeit

6
B3-Läsionen: Häufigkeit Mammographie (3-10% aller Biopsien) Ultraschall (ca. 5 % aller Biopsien) MRT-Mammographie (6-14% aller Biopsien) Heywang-Köbrunner, S.H. et al, Breast Care 2010;5:209-217
 MRT-Mammographie (6-14% aller Biopsien) Heywang-Köbrunner, S.H. et al, Breast Care 2010;5:")
7
B3-Läsionen: Häufigkeit Is mode of presentation of B3 breast core biopsies (screen-detected or symptomatic) a distinguishing factor in the final histopathologic result or risk of diagnosis of malignancy? Maclean GM, World J Surg. 2013 Nov;37(11):2607-12 B3 classification: 3.8 % (131/3.440) From symptomatic: 78 (59 %) From screen detected: 53 (41 %)
: B3 classification: 3.8 % (131/3.440) From symptomatic: 78 (59 %) From screen detected: 53 (41 %).")
8
B3-Läsionen: Häufigkeit Review showed that the histology was benign and consistent in 30 (46%) patients all of whom were discharged to routine screening. 19 (29%) cases were reported as B3 (ADH, flat atypia, LCIS or ALH) in whom all the calcifications had been removed in 13 (20%) and the patients discharged and 6 (9%) went to open biopsy for residual calcifications all of whom were benign on final analysis. There was one (1.5%) radial scar reported as B4 that went to open excision and proved benign. 15 (23%) proved malignant (B5a, B5b) and went on to definitive treatment (with one patient entered into the LORIS low risk DCIS trial). SABCS 2015 A review of 66 consecutive patients investigated for mammographic abnormalities by digital tomosynthesis guided vacuum assisted breast biopsy Munir A. et al
 cases were reported as B3 (ADH, flat atypia, LCIS or ALH) in whom all the calcifications had been removed in 13 (20%) and the patients discharged and 6 (9%) went to open biopsy for residual calcifications all of whom were benign on final analysis. There was one (1.5%) radial scar reported as B4 that went to open excision and proved benign. 15 (23%) proved malignant (B5a, B5b) and went on to definitive treatment (with one patient entered into the LORIS low risk DCIS trial). SABCS 2015 A review of 66 consecutive patients investigated for mammographic abnormalities by digital tomosynthesis guided vacuum assisted breast biopsy Munir A. et al.")
9
B3-Subtypen Häufigkeit Minimal Invasive Biopsy Results of ”Uncertain Malignant Potential ” in Digital Mammography Screening: High Prevalence but also High Predictive Value for Malignancy Weigel S et al. Fortschr Röntgenstr 2011; 183: 743–748

10
B3-Subtypen Häufigkeit Correlation of needle core biopsy with excision histology in screen-detected B3 lesions: the Merrion Breast Screening Unit experience. Hayes BD et al, J Clin Pathol. 2009 Dec;62(12):1136-40. Häufigste Subtypen (n=141) Radiäre Narbe: 57 (40,4%) ADH 25 (17,7%) Papilläre Läsion: 24 (17,0%) Predictive value of needle core biopsy diagnoses of lesions of uncertain malignant potential (B3) in abnormalities detected by mammographic screening. El-Sayed ME et al, Histopathology. 2008 Dec;53(6):650-7. The results of 523 NCBs of women screened over a 7-year period (1999-2006) in the East Midlands region, UK, with a B3 diagnosis who underwent surgical excision, were reviewed and compared with the final excision histology. Five percent of NCBs were reported as B3. The most frequent histological subtypes were atypical intraductal epithelial proliferation (AIDEP) and radial scar/complex sclerosing lesion (RS/CSL).
: Häufigste Subtypen (n=141) Radiäre Narbe: 57 (40,4%) ADH 25 (17,7%) Papilläre Läsion: 24 (17,0%) Predictive value of needle core biopsy diagnoses of lesions of uncertain malignant potential (B3) in abnormalities detected by mammographic screening. El-Sayed ME et al, Histopathology Dec;53(6): The results of 523 NCBs of women screened over a 7-year period ( ) in the East Midlands region, UK, with a B3 diagnosis who underwent surgical excision, were reviewed and compared with the final excision histology. Five percent of NCBs were reported as B3. The most frequent histological subtypes were atypical intraductal epithelial proliferation (AIDEP) and radial scar/complex sclerosing lesion (RS/CSL)..")
11
B3-Läsionen Datenlage: Späteres Mammakarzinomrisiko

12
B3 – Läsionen Späteres Mammakarzinomrisiko ADH: Indikator-/Vorläuferläsion: Ipsi-and kontralateral erhöhtes Brustkrebsrisiko: 3–5-fach nach 10 Jahren. LIN: Indikator-/Vorläufer-Läsion: Ipsi-und kontralateral erhöhtes Brustkrebsrisiko: 7-fach nach 10 Jahren Atypisches Papillom: Indikatorläsion erhöhtes ipsilaterales Karzinomrisiko (4.6% bis zu 13%)
.")
13
Späteres Mammakarzinomrisiko ADH / ALH Hwang, SABCS 2015

14
Späteres Mammakarzinomrisiko Papillom Intraductal papillomas: Risk of cancer, immediate and delayed Khan S et al., SABCS 2015 For patients without atypia or ADH/ALH at the time of biopsy and no cancer on excision, the probability of remaining cancer-free was not significantly different for patients who had immediate surgical excision versus those that were observed (93.8% and 91.5% cancer-free at 10 years, p= 0.773). For patients with atypia or ADH/ALH at the time of biopsy but no cancer on excision, the probability of remaining cancer- free in both breasts was 85.9% at 10 years, and did not differ between patients who were excised or observed (p= 0.518). However, those w/atypia or ADH/ALH were significantly less likely to remain cancer-free than those w/o atypia (85.9% versus 92.8% at 10 years, respectively, p=0.008).
. However, those w/atypia or ADH/ALH were significantly less likely to remain cancer-free than those w/o atypia (85.9% versus 92.8% at 10 years, respectively, p=0.008)..")
15
B3-Läsionen Datenlage: Benachbartes Karzinom

16
B3-Subtypen Positiver prädiktiver Wert für Malignität Borderline breast core needle histology: predictive values for malignancy in lesions of uncertain malignant potential (B3) N Houssami et al, British Journal of Cancer 2007
 N Houssami et al, British Journal of Cancer 2007")
17
B3-Subtypen Positiver prädiktiver Wert für Malignität Minimal Invasive Biopsy Results of ”Uncertain Malignant Potential ” in Digital Mammography Screening: High Prevalence but also High Predictive Value for Malignancy Weigel S et al. Fortschr Röntgenstr 2011; 183: 743–748

18
B3-Subtypen Positiver prädiktiver Wert für Malignität Correlation of needle core biopsy with excision histology in screen-detected B3 lesions: the Merrion Breast Screening Unit experience. Hayes BD et al, J Clin Pathol.2009 Dec;62(12):1136-40 N=141, Exzisionsbiopsien mit maligner Histologie: Insgesamt 16,0% ALH, LCIS: 50,0% ADH: 32,0% FEA: 12,5% Papilläre Läsion: 8,3% V.a. Phylloides Tumor: 7,7% Predictive value of breast lesions of "uncertain malignant potential" and "suspicious for malignancy" determined by needle core biopsy Dillon MF et al, Ann Surg Oncol.2007 Feb;14:704-11. N=210, Exzisionsbiopsien mit maligner Histologie: Insgesamt 21,0% ALH, LCIS: 44,0% ADH: 35,0% Radiäre Narbe 6,0% Papilläre Läsion: 14.0%
: N=141, Exzisionsbiopsien mit maligner Histologie: Insgesamt 16,0% ALH, LCIS: 50,0% ADH: 32,0% FEA: 12,5% Papilläre Läsion: 8,3% V.a. Phylloides Tumor: 7,7% Predictive value of breast lesions of uncertain malignant potential and suspicious for malignancy determined by needle core biopsy Dillon MF et al, Ann Surg Oncol.2007 Feb;14: N=210, Exzisionsbiopsien mit maligner Histologie: Insgesamt 21,0% ALH, LCIS: 44,0% ADH: 35,0% Radiäre Narbe 6,0% Papilläre Läsion: 14.0%.")
19
B3-Subtypen Positiver prädiktiver Wert für Malignität Atypical ductal hyperplasia and breast cancers – A ten year clinical and pathological review on core biopsy, lumpectomy and mastectomy specimens Co M, Kwong A., SABCS 2015

20
Improved malignancy prediction by B3 breast lesions subclassification. de Beça FF et al.,Ann Diagn Pathol.2013 Oct;17(5):434-6. B3 category lesions had an overall PPV for malignancy of 12.5% and significant low odds of malignancy of 0.14. When subclassified, B3b (lesions with atypia) demonstrated a higher PPV for malignancy (36.36%) with a nonsignificant odds. Inversely, B3a (lesions without atypia) demonstrated a PPV for malignancy of only 5.41% and a significant low odds of malignancy of only 0.06. B3 - Läsionen Einflußfaktoren auf den PPW für Malignität B3 breast lesions determined by vacuum-assisted biopsy: how to reduce the frequency of benign excision biopsies. Tonegutti M, Radiol Med.2010 Dec;115(8):1246-57 Atypia at VAB was reported in 60 of 102 cases (58.8%). Carcinoma was found at excision in 5/60 (8%) B3 lesions with atypia and in no B3 lesions without atypia (p=0.146).
: B3 category lesions had an overall PPV for malignancy of 12.5% and significant low odds of malignancy of When subclassified, B3b (lesions with atypia) demonstrated a higher PPV for malignancy (36.36%) with a nonsignificant odds. Inversely, B3a (lesions without atypia) demonstrated a PPV for malignancy of only 5.41% and a significant low odds of malignancy of only B3 - Läsionen Einflußfaktoren auf den PPW für Malignität B3 breast lesions determined by vacuum-assisted biopsy: how to reduce the frequency of benign excision biopsies. Tonegutti M, Radiol Med.2010 Dec;115(8): Atypia at VAB was reported in 60 of 102 cases (58.8%). Carcinoma was found at excision in 5/60 (8%) B3 lesions with atypia and in no B3 lesions without atypia (p=0.146)..")
21
B3 – Läsionen Einflußfaktoren auf den PPW für Malignität Nonmalignant Breast Papillary Lesions at Core-Needle Biopsy: A Meta-analysis of Underestimation and Influencing Factors Xin Wen et al, Annals of Surgical Oncology, January 2013, Volume 20, Issue 1, pp 94-101 A total of 34 studies, which included 2,236 nonmalignant breast papillary lesions diagnosed at CNB and histologically examined after surgical excision, were included. The pooled estimate for the percentage of underestimation was 15.7 % [95 % confidence interval (CI): 12.8–18.5 %]. The factors associated with higher underestimation included atypical papillary lesions (P < 0.001), positive mammographic findings (P = 0.022), and article publication year before 2005 (P < 0.05).
: 12.8–18.5 %]. The factors associated with higher underestimation included atypical papillary lesions (P < 0.001), positive mammographic findings (P = 0.022), and article publication year before 2005 (P < 0.05)..")
22
B3 – Läsionen Einflußfaktoren auf den PPW für Malignität Intraductal papillomas: Risk of cancer, immediate and delayed Khan S et al., SABCS 2015 When surgical excision was performed for IP w/ atypia or IP + ADH/ALH on CNBx, cancer was found in 32% and 38.5% respectively. IP w/o atypia, cancer was found in 8.3%, significantly different from IP w/ atypia (p=0.004) and IP + ADH/ALH (p=0.007).
 and IP + ADH/ALH (p=0.007)..")
23
B3 - Läsionen Einflußfaktoren auf den PPW für Malignität Is mode of presentation of B3 breast core biopsies (screen-detected or symptomatic) a distinguishing factor in the final histopathologic result or risk of diagnosis of malignancy? Maclean GM, World J Surg. 2013 Nov;37(11):2607-12 There was no statistically significant difference between papillary and fibroepithelial diagnoses between the two groups (47 vs. 42 %, p = 0.59, NS). There was no difference between the groups for atypia, lobular neoplasia, or sclerosing lesions (49 vs. 51 %, p = 0.8, NS). Cancer was found in 20 % of the symptomatic patients and in 17 % of the screen-detected group (p = 0.65, NS).
: There was no statistically significant difference between papillary and fibroepithelial diagnoses between the two groups (47 vs. 42 %, p = 0.59, NS). There was no difference between the groups for atypia, lobular neoplasia, or sclerosing lesions (49 vs. 51 %, p = 0.8, NS). Cancer was found in 20 % of the symptomatic patients and in 17 % of the screen-detected group (p = 0.65, NS)..")
24
B3 - Läsionen Einflußfaktoren auf den PPW für Malignität Borderline breast lesions: comparison of malignancy underestimation rates with 14- gauge core needle biopsy versus 11-gauge vacuum-assisted device Viviana Londero, Eur Radiol 2011 Jun 12;21(6):1200-6 Overall malignancy underestimation rate was 12.7% at 14-g CNB and 12.5% at 11-g VAB ( n=4764 biopsies) Based on excision histology or follow-up, lesion-specific underestimation rates were: benign papillomas: 14-g CNB 11%, 11-g VAB 0%; RSL: 14-g CNB 6%, 11-g VAB 4%; LN: 14-g CNB 40%, 11-g VAB 23%; ADH: 14-g CNB 33%; 11-g VAB 22%.
: Overall malignancy underestimation rate was 12.7% at 14-g CNB and 12.5% at 11-g VAB ( n=4764 biopsies) Based on excision histology or follow-up, lesion-specific underestimation rates were: benign papillomas: 14-g CNB 11%, 11-g VAB 0%; RSL: 14-g CNB 6%, 11-g VAB 4%; LN: 14-g CNB 40%, 11-g VAB 23%; ADH: 14-g CNB 33%; 11-g VAB 22%.")
25
Daten aus Hohenlind B3-Läsionen zwischen 1/2008 und 10/2015

26
B3-Läsionen von 1/2008 bis 10/2015 Anzahl / Jahr n=234 Detektion Bildgebendes Verfahren Häufigkeit Mammographie- screening 85 (36,3%) Mammographie (kurativ) 58 (24,8%) Sonographie83 (35,5%) MRT-Mammographie 8 ( 3,4%)
 Mammographie (kurativ) 58 (24,8%) Sonographie83 (35,5%) MRT-Mammographie 8 ( 3,4%)")
27
Häufigkeit der B3-Subtypen SubtypInsgesamt n=234 Screening-MG n=85 Kurative MG n=58 Sono n=83 MRT-MG n=8 ADH 61 (26,1%)36 (42,3%)13 (22,4%) 8 ( 9,6%) 4 (50,0%) ALH, LCIS 15 ( 6,4%) 7 ( 8,2%) 7 (12,1%) 0 1 (12,5%) FEA 38 (16,2%)18 (21,2%)15 (25,9%) 4 ( 4,8%) 1 (12,5%) Papilläre Läsion 87 (37,2%)21 (24,7%)20 (34,5%)45 (54,2%) 1 (12,5%) Radiäre Narbe 12 ( 5,1%)3 ( 3,5%) 3 ( 5,2%) 5 ( 6,0%) 1 (12,5%) Zellreiches Fibroadenom, V.a. Phylloides Tumor 21 ( 9,0%)0 021 (25,3%) 0
0 021 (25,3%) 0.")
28
Diagnoserelevante mammographische Auffälligkeit SubtypInsgesamtMikrokalk +/- Architekturstörung Herdbefund +/- Architekturstörung ADH4944 (89,8%) 5 (10,2%) ALH, LCIS1414 (100%) 0 FEA3331 (93,9%) 2 ( 6,1%) Papilläre Läsion4127 (65,9%)14 (34,1%) Radiäre Narbe 6 3 (50,0%)
 5 (10,2%) ALH, LCIS1414 (100%) 0 FEA3331 (93,9%) 2 ( 6,1%) Papilläre Läsion4127 (65,9%)14 (34,1%) Radiäre Narbe 6 3 (50,0%)")
29
B3-Läsionen: PPW für Malignität BildgebungAnteil maligner Befunde nach PE Insgesamt in situ invasiv 42 / 234 (17,9%) 26 / 234 (11,1%) 16 / 234 ( 6,8%) Screening in situ invasiv 17 / 85 (20,0%) 9 / 85 (10,6%) 8 / 85 ( 9,4%) Kuratives Setting in situ invasiv 25 / 149 (16,8%) 17 / 149 (11,4%) 8 / 149 ( 5,4%)
 26 / 234 (11,1%) 16 / 234 ( 6,8%) Screening in situ invasiv 17 / 85 (20,0%) 9 / 85 (10,6%) 8 / 85 ( 9,4%) Kuratives Setting in situ invasiv 25 / 149 (16,8%) 17 / 149 (11,4%) 8 / 149 ( 5,4%)")
30
B3-Läsionen PPW für Malignität SubtypPPWAnteil in situAnteil invasiv ADH10 / 61 (16,4%) 10 / 10 (100,0%) ALH,LCIS ALH LCIS 2 / 15 (13,3%) 1 / 12 ( 8,3%) 1 / 3 (33,3%) 1 / 15 ( 50,0%) 1 / 12 (100,0%) 1 / 15 ( 50,0%) 1 / 3 (100,0%) FEA 7 / 38 (18,4%) 7 / 7 (100,0%) Papilläre Läsion typ. Papillom atyp. Papillom 14 / 87 (16,1%) 8 / 73 (11,0%) 6 / 14 (42,9%) 12 / 14 ( 85,7%) 7 / 8 ( 87,5%) 5 / 6 ( 83,3%) 2 / 14 ( 14,3%) 1 / 8 ( 12,5%) 1 / 6 ( 16,7%) Radiäre Narbe 1 / 12 ( 8,3%) 1 / 1 (100,0%) Zellreiches Fibroadenom, V.a. Phylloides Tumor 8 / 21 (14,3%)Ben. Phylloides-Tu: 5/8 (62,5%)Mal.Phylloides-Tu: 3/8 (37,5%)
 8 / 73 (11,0%) 6 / 14 (42,9%) 12 / 14 ( 85,7%) 7 / 8 ( 87,5%) 5 / 6 ( 83,3%) 2 / 14 ( 14,3%) 1 / 8 ( 12,5%) 1 / 6 ( 16,7%) Radiäre Narbe 1 / 12 ( 8,3%) 1 / 1 (100,0%) Zellreiches Fibroadenom, V.a. Phylloides Tumor 8 / 21 (14,3%)Ben. Phylloides-Tu: 5/8 (62,5%)Mal.Phylloides-Tu: 3/8 (37,5%).")
31
Empfehlungen für die Praxis

32
Management nach minimalinvasiver Biopsie Dabei ist zu beachten: Repräsentativität der Stanzbiopsie (Ausdehnung der Läsion in der Bildgebung, prozentuale Entfernung durch die Stanzbiopsie) Überwachbarkeit der Patientin
 Überwachbarkeit der Patientin")
33
B3 – Läsion Bedeutung der Subtypen Repräsentativität?

34
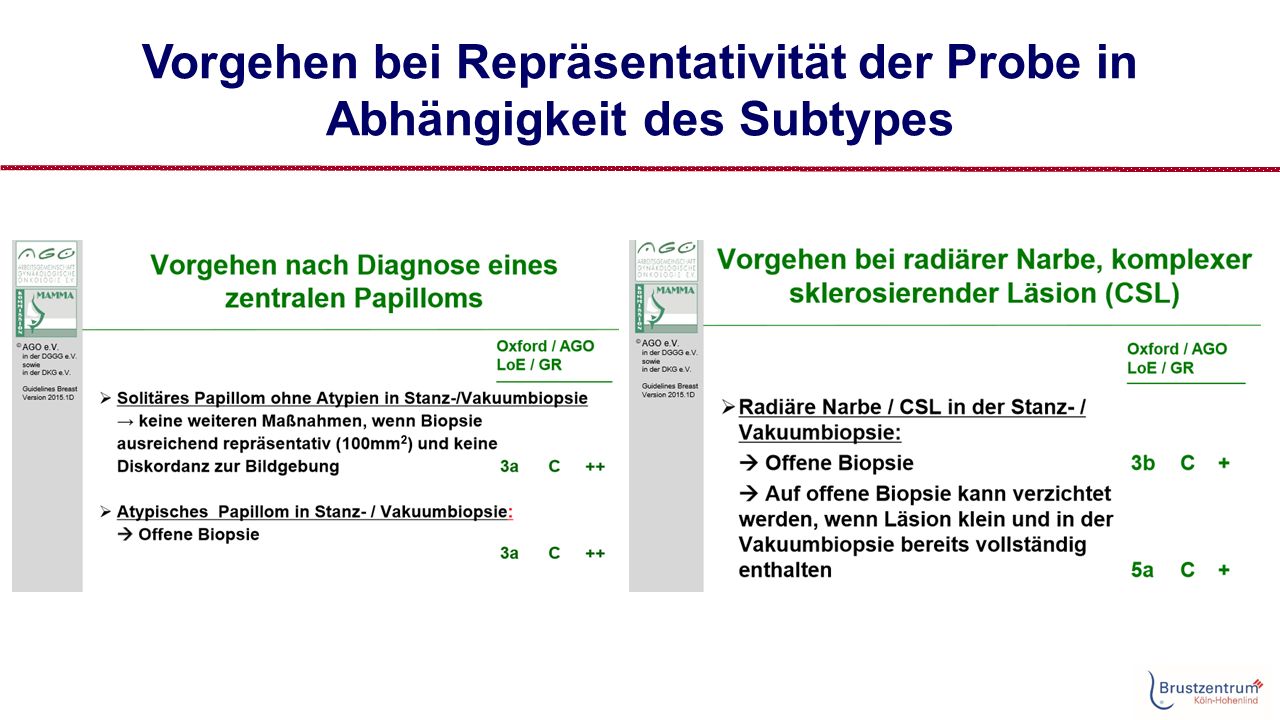
Vorgehen bei Repräsentativität der Probe in Abhängigkeit des Subtypes

36
Endokrine Prävention Hwang E., SABCS 2015

37
Vielen Dank für Ihre Aufmerksamkeit!

Ähnliche Präsentationen







 András Bárdossy IWS Universität Stuttgart.>")

 The dependence of convection-related parameters on surface and.>")









