Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Vom Umgang mit Infektionen und Exazerbationen Tobias Welte Klinik für Pneumologie

2
Pneumologische Infektiologie III
Oberer Atemwegsinfekt Pneumonie ambulant erworben nosokomial Tuberkulose

3
S3 Leitlinie untere Atemwegsinfektion Krankheitsbilder
akute Bronchitis akute Exazerbation einer chronischen Bronchitis Influenza und andere respiratorische Virusinfektionen ambulant erworbener Pneumonie

4
Neuraminidase Inhibitors in Influenza
Neuraminidase inhibitors (NI) prevent symptoms and shorten the duration of illness by about one day if taken within 48 hours of the onset of symptoms Oseltamivir did not reduce influenza related lower respiratory tract complications (RR 0.55, 95% CI 0.22 to 1.35) NI reduce the chance of people exposed to influenza developing laboratory confirmed influenza but not influenza-like illness Oseltamivir causes nausea Jefferson T et al. BMJ 2009; 339
 prevent symptoms and shorten the duration of illness by about one day if taken within 48 hours of the onset of symptoms. Oseltamivir did not reduce influenza related lower respiratory tract complications (RR 0.55, 95% CI 0.22 to 1.35) NI reduce the chance of people exposed to influenza developing laboratory confirmed influenza but not influenza-like illness. Oseltamivir causes nausea. Jefferson T et al. BMJ 2009; 339.")
5
Schwere Influenza: Oseltamivir nach 48h wirkunglos?
Studie: Kanada, 2004/05 Patienten: n=84, Intensivstation, PCR-positiv Ergebnisse: Letalität 25/84 (30%) Oseltamivir-Therapie: 3/25 (12%) kein Oseltamivir: 20/56 (36%p = 0,03) Keiner der Patienten erhielt Oseltamivir innerhalb der ersten 48 h ! McGeer et al. CID 2007 Dec 15;45(12):
 Oseltamivir-Therapie: 3/25 (12%) kein Oseltamivir: 20/56 (36%p = 0,03) Keiner der Patienten erhielt Oseltamivir innerhalb der ersten 48 h ! McGeer et al. CID 2007 Dec 15;45(12):")
6
AWMF-Leitlinien-Register Nr. 82/001

7
AECOPD Auslöser Annähernd die Hälfte aller AECOPD werden durch infektiöse Ursachen ausgelöst, wobei nach neueren Untersuchungen Viren die führende Ursache sind. Die häufigsten bakteriellen Erreger sind H. influenzae, S. pneumoniae, M. catarrhalis, Enterobacteriaceae und P. aeruginosa

8
Antibiotika bei AECOPD
Retrospektive Kohortenstudie Daten von 413 Akutkliniken der USA, 1/2006 – 12/2007 Patienten mit AECOPD über 40 Jahre 79% der Pat. bekamen mindestens für 2kconsecutive Tage Antibiotika Antibiotika behandelte Pat. unterschieden sich signifikant von nicht behandelten Patienten durch eine niedrigere Notwendigkeit der Beatmung eine geringere Sterblichkeit eine geringere Rate an Wiederaufnahmen aufgrund AECOPD Eine höhere Rate an Wiederaufnahmen wegen Clostridium difficile (0.19%; 95% CI, Eine komplizierte Adjustierung unter Berücksichtigung aller Einflußfaltoren zeigte eine Reduktion der Therapieversager um 13% (odds ratio, 0.87; 95% CI, ) These findings, that all patient groups seemed to benefit from therapy and that harms were minimal,support the notion that all patients hospitalized with acute exacerbations of COPD should be prescribed antibiotics. This recommendation,however, is not consistent with the fact that roughly 50% of COPD patients do not have a bacterial etiology for their exacerbation. Identifying these patients remains a challenge, because sputum cultures do not distinguish between active infection and colonization. Rothberg MB. JAMA. 2010;303(20): 16
 These findings, that all patient groups seemed to benefit from therapy and that harms were minimal,support the notion that all patients hospitalized with acute exacerbations of COPD should be prescribed antibiotics. This recommendation,however, is not consistent with the fact that roughly 50% of COPD patients do not have a bacterial etiology for their exacerbation. Identifying these patients remains a challenge, because sputum cultures do not distinguish between active infection and colonization. Rothberg MB. JAMA. 2010;303(20):")
9
COPD Was beweist die bakterielle Besiedlung?
Daniels J. Clin Microbiol Infect 2010; 16: 583–588

10
Antibiotics for AECOPD: Risk Stratification
MILD Only 1 of the 3 cardinal symptoms: Increased dyspnea Increased sputum volume Increased sputum purulence MODERATE OR SEVERE At least 2 of the 3 cardinal symptoms: Increased dyspnea Increased sputum volume Increased sputum purulence Uncomplicated COPD No risk factors: Age <65 years FEV1 >50% predicted <3 exacerbations/year No cardiac disease Complicated COPD 1 or More risk factors: Age >65 years FEV1 <50% predicted >3 exacerbations/year Cardiac disease No antibiotics Increased bronchodilator Symptomatic therapy Monitoring of symptoms Advanced macrolide (azithromycin, clarithromycin) Cephalosporin (cefuroxime, cefpodoxime, cefdinir) Doxycycline Trimethoprim–sulfamethoxazole If recent antibiotic exposure (<3 months), use alternative class Fluoroquinolone (moxi, gemi, levo) Amoxicillin-clavulanate If at risk for Pseudomonas, consider ciprofloxacin and obtain sputum culture If recent antibiotic exposure (<3 months), use alternative class Risk factors for poor outcome, such as age, severity of underlying airway obstruction, presence of comorbid illnesses, a history of recurrent exacerbations, use of home oxygen, use of chronic steroids, and hypercapnia should be considered in selecting antibiotics to for treating exacerbations. Theoretically, patients at greater risk for poor outcome would benefit most from early aggressive antibiotic therapy. Patients can least afford to be treated with an antibiotic that turns out to be ineffective against the pathogen that causes the exacerbation. Thresholds that are clinically useful and predictive of poor outcome include forced expiratory volume in 1 second (FEV1) less than 50% for severity of airway obstruction, significant cardiac disease among the comorbid illnesses, and more than 3 exacerbations in the previous 12 months among the group with recurrent exacerbations. In patients who fail initial empiric antimicrobial therapy, it would be appropriate to reexamine the patient to confirm the diagnosis, consider sputum studies to ascertain for resistant or difficult-to-treat pathogens, and treat with an alternative agent with better in vitro microbiologic efficacy. Although antibiotic treatment for exacerbations is now more evidence-based and rational, the impact of the risk stratification approach on the outcome of exacerbations needs to be evaluated. References: Sethi S, Murphy TF. Acute exacerbations of chronic bronchitis: new developments concerning microbiology and pathophysiology–impact on approaches to risk stratification and therapy. Infect Dis Clin N Am. 2004;18: Worsening clinical status or inadequate response in 72 hrs Sethi S, Murphy TF. NEJM 2008;359: Reevaluate Consider sputum culture 17 10
 Cephalosporin (cefuroxime, cefpodoxime, cefdinir) Doxycycline. Trimethoprim–sulfamethoxazole. If recent antibiotic exposure (<3 months), use alternative class. Fluoroquinolone (moxi, gemi, levo) Amoxicillin-clavulanate. If at risk for Pseudomonas, consider ciprofloxacin and obtain sputum culture. If recent antibiotic exposure (<3. months), use alternative class. Risk factors for poor outcome, such as age, severity of underlying airway obstruction, presence of comorbid illnesses, a history of recurrent exacerbations, use of home oxygen, use of chronic steroids, and hypercapnia should be considered in selecting antibiotics to for treating exacerbations. Theoretically, patients at greater risk for poor outcome would benefit most from early aggressive antibiotic therapy. Patients can least afford to be treated with an antibiotic that turns out to be ineffective against the pathogen that causes the exacerbation. Thresholds that are clinically useful and predictive of poor outcome include forced expiratory volume in 1 second (FEV1) less than 50% for severity of airway obstruction, significant cardiac disease among the comorbid illnesses, and more than 3 exacerbations in the previous 12 months among the group with recurrent exacerbations. In patients who fail initial empiric antimicrobial therapy, it would be appropriate to reexamine the patient to confirm the diagnosis, consider sputum studies to ascertain for resistant or difficult-to-treat pathogens, and treat with an alternative agent with better in vitro microbiologic efficacy. Although antibiotic treatment for exacerbations is now more evidence-based and rational, the impact of the risk stratification approach on the outcome of exacerbations needs to be evaluated. References: Sethi S, Murphy TF. Acute exacerbations of chronic bronchitis: new developments concerning microbiology and pathophysiology–impact on approaches to risk stratification and therapy. Infect Dis Clin N Am. 2004;18: Worsening clinical status or inadequate response in 72 hrs. Sethi S, Murphy TF. NEJM 2008;359: Reevaluate. Consider sputum culture")
11
Ambulant erworbene Pneumonie Definition
Eine Pneumonie, die außerhalb der Klinik (im ambulanten Bereich) erworben worden ist Aufgrund der Inkubationszeit der wichtigsten Erreger wird eine Pneumonie auch innerhalb der ersten 48 Stunden nach Krankenhausaufnahme noch als ambulant erworben betrachtet, umgekehrt gilt sie bis eine Woche nach Krankenhausentlassung noch als nosokomial.
 erworben worden ist. Aufgrund der Inkubationszeit der wichtigsten Erreger wird eine Pneumonie auch innerhalb der ersten 48 Stunden nach Krankenhausaufnahme noch als ambulant erworben betrachtet, umgekehrt gilt sie bis eine Woche nach Krankenhausentlassung noch als nosokomial.")
12
Pathogenes in CAP (using Bartlett Criteria) Data from the German CAPNETZ
Welte T. Semin Respir Crit Care Med 2009; 30:

13
CRB-65 Score C onfusion – neu aufgetretene Verwirrtheit
R espiratory rate (Atemfrequenz> 30/min) B lood pressure (RRsyst < 90 mmHg or RRdiast < 60mmHG) > 65 0 Punkte ambulante Behandlung 1 Punkt stationäre Aufnahme erwägen > 2 Punkte stationäre Aufnahme
 B lood pressure (RRsyst < 90 mmHg or RRdiast < 60mmHG) > Punkte ambulante Behandlung. 1 Punkt stationäre Aufnahme erwägen. > 2 Punkte stationäre Aufnahme.")
14
CAP und Alter Ewig S et al. Thorax 2009; 64: BQS Daten aller hospitalisierten Patienten mit CAP in 2005 and 2006 n = 388,406 Inzidenz der hospitalisierten CAP 2.75 und 2.96 per 1,000 Population/Jahr Inzidenz 3.21 für Männer versus 2.52 für Frauen Inzidenz von 7.65 per 1,000 Population/Jahr für ≥ 60 Jährige Sterblichkeit 13.72/14.44% CRB-65 sagt das Risiko für Tod zuverlässig voraus Höchste Sterblichkeit in den ersten 3 Tagen nach Aufnahme Nur wenige der Verstorbenen wurden beatmet (15.74%) 20
 20.")
15
Ewig S et al. Thorax 2009; 64:

16
Niedrig-Risiko Patienten mit unkomplizierter ambulant erworbener Pneumonie ohne Risikofaktoren

17
Diagnostik bei unkomplizierter CAP
CAP Diagnostik Diagnostik bei unkomplizierter CAP gründliche klinische Untersuchung Anfertigen einer Röntgenthorax-Aufnahme Laboruntersuchung zur Erfassung wichtiger biologischer Parameter begrenzen Eine mikrobiologische Diagnostik wird nicht empfohlen.

18
Substanzen* Dosierung (pro Tag)* Therapiedauer Mittel der Wahl
Aminopenicillin - Amoxicillin 70 kg: 3 x 1 g oral < 70 kg: 3 x 0,75 g oral 5 - 7 Tage Alternativen Makrolid - Azithromycin 1 x 500 mg oral 3 Tage - Clarithromycin 2 x 500 mg oral - Roxithromycin 1 x 300 mg oral oder Tetracyclin - Doxycyclin 1 x 200 mg oral initial, 70 kg: 1x200 mg < 70 kg: 1x100 mg 11

19
Therapieempfehlung für die kalkulierte Initialtherapie bei hospitalisierten Patienten mit ambulant erworbener Pneumonie ohne Risiko einer Infektion durch P. aeruginosa

20
Pathogenes in CAP (using Bartlett Criteria) Data from the German CAPNETZ
Welte T. Semin Respir Crit Care Med 2009; 30:

21
Risikostratefizierung für Intensivaufenthalt

22
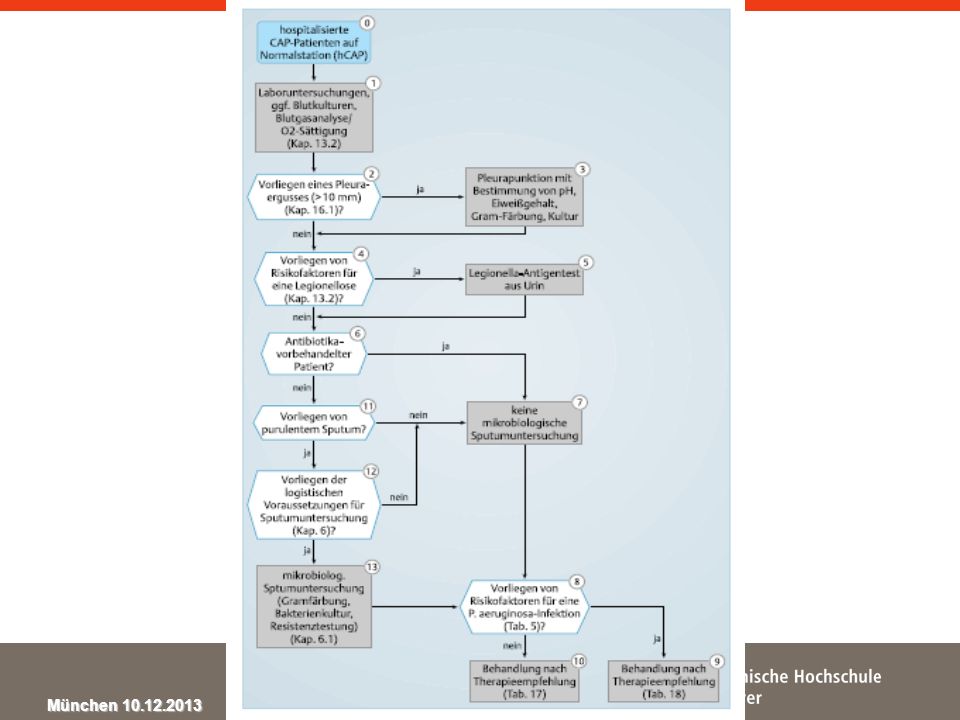
Diagnostik bei schwerer CAP

24
Substanzen für die Initialtherapie
Dosierung der Initialtherapie (pro Tag) Therapiedauer Betalaktam - Amoxicillin/Clavulansäure 3 x 2,2 g i.v. 5 – 7 Tage - Ampicillin/Sulbactam 3 x 3,0 g i.v. - Cefuroxim 3 x 1,5 g i.v. - Ceftriaxon 1 x 2,0 g i.v. - Cefotaxim 3 x 2,0 g i.v. Plus/minus Makrolid* oder Fluorchinolon - Levofloxacin 1 x 500 mg i.v. - Moxifloxacin 1 x 400 mg i.v. oder bei ausgewählten Patienten Carbapenem Ertapenem 1 x 1,0 g i.v. mit oder ohne Makrolid
 Therapiedauer. Betalaktam. - Amoxicillin/Clavulansäure. 3 x 2,2 g i.v. 5 – 7 Tage. - Ampicillin/Sulbactam. 3 x 3,0 g i.v. - Cefuroxim. 3 x 1,5 g i.v. - Ceftriaxon. 1 x 2,0 g i.v. - Cefotaxim. 3 x 2,0 g i.v. Plus/minus Makrolid* oder Fluorchinolon. - Levofloxacin. 1 x 500 mg i.v. - Moxifloxacin. 1 x 400 mg i.v. oder bei ausgewählten Patienten Carbapenem. Ertapenem. 1 x 1,0 g i.v. mit oder ohne Makrolid.")
25
Kombinationstherapie bei CAP
Retrospektive Kohortenstudie in San Antonio, Texas 237 von 787 Patienten mit schwerer Sepsis 104 Patienten mit Kombinationstherapie mit Makrolid 133 Patienten ohne Makrolid 30 Tage Letalität 20.3% 90 Tage Letalität 24.5% Sterblichkeitsreduktion um 70% mit Kombinationstherapie Restrepo MI. ERJ 2008; September 3; online

26
The ProCAP Study – Antibiotic Duration
Christ-Crain M et al, AJRCCM 2006; 174(1):84-93 20 Antibiotic Prescriptoin (%) 19 17 p < 0.001 15 13 Antibiotic duration (days) 12 10 8 6 4 2 Standard group PCT group Standard group PCT group
: Antibiotic Prescriptoin (%) p < Antibiotic duration (days) Standard group. PCT group. Standard group. PCT group.")
27
Therapieempfehlung für die kalkulierte Initialtherapie bei hospitalisierten Patienten mit ambulant erworbener Pneumonie mit Risiko einer Infektion durch P. aeruginosa

28
Mortality from CAP through PA „Definite“ and „indeterminate“
* 55% of all EB isolates were indeterminate Von Baum H, Welte T. ERJ 2010 Mar;35(3): resp. sample availabe, no EB/PA (n = 1840) definite PA (n = 22) indeterminate PA (n = 27) * age (mean, yrs) 58 ± 18 64 ± 17 68 ± 11 nursing home resident (%) 2 23 7 chronic resp. disease 37 68 52 enteral tube feeding 0.6 11 mortality 4 18
: resp. sample availabe, no EB/PA. (n = 1840) definite PA. (n = 22) indeterminate PA. (n = 27) * age (mean, yrs) 58 ± ± ± 11. nursing home resident (%) chronic resp. disease enteral tube feeding mortality")
29
Substanzen für die Initialtherapie
Dosierung der Initialtherapie (pro Tag) Therapiedauer Pseudomonasaktives Betalaktam - Piperacillin/Tazobactam 3 x 4,5 g i.v. Tage - Cefepim 3 x 2,0 g i.v. - Imipenem 3 x 1,0 g i.v. - Meropenem Plus Aminoglykosid 3 - 5 Tage oder Fluorchinolon - Levofloxacin 2 x 500 mg i.v. Tage - Ciprofloxacin plus Pneumokokken- und S. aureus-wirksames Antibiotikum 3 x 400 mg i.v.
 Therapiedauer. Pseudomonasaktives Betalaktam. - Piperacillin/Tazobactam. 3 x 4,5 g i.v Tage. - Cefepim. 3 x 2,0 g i.v. - Imipenem. 3 x 1,0 g i.v. - Meropenem. Plus Aminoglykosid Tage. oder Fluorchinolon. - Levofloxacin. 2 x 500 mg i.v Tage. - Ciprofloxacin plus Pneumokokken- und S. aureus-wirksames Antibiotikum. 3 x 400 mg i.v.")
30
Ambulant erworbene Pneumonie klinische Stabilität
Herzfrequenz ≤ 100/min, Atemfrequenz ≤ 24/min, Systolischer Blutdruck ≥ 90 mmHg Körpertemperatur ≤ 37,8 oC, Fähigkeit zur oralen Nahrungsaufnahme, normaler Bewusstseinszustand, keine Hypoxämie (PO2 ≥ 60 mm Hg bzw. SaO2 ≥ 90%).
.")
32
Pneumokokken-Vakzine und Influenzaimfpung
Interventionsstudie in Stockholm alle Einwohner >65 J. (n=259 627) konnten sich impfen lassen (Influenza/Pneumokokken) Erfassung von Krankenhausaufnahmen von 12/1998 – 05/1999 Geimpft (n=100242) Ungeimpft (n= ) Todesfälle/ 1000 E. 15,1 34,7 Mortalität (90%-CI) -57% (55-60) P-Wert < 0,0001 Cristenson et al., Lancet. 2001 32
 konnten sich impfen lassen (Influenza/Pneumokokken) Erfassung von Krankenhausaufnahmen von 12/1998 – 05/1999. Geimpft. (n=100242) Ungeimpft. (n= ) Todesfälle/ 1000 E. 15,1. 34,7. Mortalität (90%-CI) -57% (55-60) P-Wert. < 0,0001. Cristenson et al., Lancet")
33
Influenza viruses

34
Influenza Excess Mortality
Age-specic multiple linear regression models to all-cause and cause-specic mortality rates in Hong Kong ( ) Annual influenza-associated all-cause excess mortality rate was 11.1 per person-years. Estimated average of 751 excess deaths per year associated with influenza 95% of the excess deaths in persons aged 65 years Wu P, et al JID 2012;206:1862–71
 Annual influenza-associated all-cause excess mortality rate was 11.1 per person-years. Estimated average of 751 excess deaths per year associated with influenza. 95% of the excess deaths in persons aged 65 years. Wu P, et al JID 2012;206:1862–71.")
35
Geschichte der Influenzaimpfstoffe
McCullers & Huber. Hum Vaccin Immunother 2012;8:34-44 2009 pandemic 1968 pandemic ‘Swine’ H1N1 1957 pandemic H3N2 1918 pandemic H2N2 Re-emergence of seasonal H1N1 H1N1 H1N1 VICTORIA Influenza B lineages Describe the slide in terms of timeline of the circulation of different viruses, isolation of influenza A virus and then B virus YAMAGATA Trivalent vaccine Bivalent vaccine (influenza A and B) Quadrivalent influenza vaccine Monovalent influenza A vaccine 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 First isolation of influenza A virus First isolation of influenza B virus 35
 Quadrivalent influenza vaccine. Monovalent influenza A vaccine First isolation of influenza A virus. First isolation of influenza B virus. 35.")
36
Vaccines against influenza WHO position paper – November 2012
Influenza vaccination is highly recommended for pregnant womens Children aged 6-23 month Children aged 2-5 years Elderly > 65 years of age Persons with specific chronic conditions Health Care Workers International Travelers

37
Pneumonie bei Kindern- UK
2 + 1 Aufnahme in nationalen Impfplan Koshy E et al. Thorax 2010;65: 1 bis 4 Jahre Aufnahme PCV-7 in nationalen Impfplan 2 Jahre nach Einführung von routinemäßig PCV-7 sanken die durch bakterielle Pneumonien bedingten Hospitalisierungsraten bei Kindern < 15 Jahren um 19%. 37 37 37

38
Verfügbare Pneumokokken-Impfstoffe
konjugierte Vakzine (Prevenar13, Synflorix) Polysaccharide von 10/13 Serotypen konjugiert (Diphterietoxin, Tetanustoxin, Membranprotein H.influenzae) nicht-konjugierte Vakzine (Pneumovax) Polysaccharide von23 Serotypen nicht konjugiert (reine Polysaccharide) Pletz M et al, IJAAC, 2008 38
 Polysaccharide von 10/13. Serotypen. konjugiert. (Diphterietoxin, Tetanustoxin, Membranprotein H.influenzae) nicht-konjugierte Vakzine. (Pneumovax) Polysaccharide von23 Serotypen. nicht konjugiert. (reine Polysaccharide) Pletz M et al, IJAAC,")
39
Geometric Mean Ratio (GMR)
PCV13 induziert ähnliche funktionale Antikörper-antworten bei PPV-vorgeimpften Erwachsenen 80 Jahre NON-INFERIORITY PCV13 höhere Antikörper-Antwort 1 2 3 4 5 9 10 6A 6B 7F 9V 14 18C 19A 19F 23F Geometric Mean Ratio (GMR) Jackson L et al. ECCMID 2011
 Jackson L et al. ECCMID")
40
Pneumokokkenimpfung Vorgehen in der MHH November 2013
Impfung empfohlen für Patienten > 50 Jahre Patienten mit chronischen Erkrankungen Patienten mit Immunsuppression Splenektomie Transplantation Immunsuppressiva für andere Erkrankungen

41
Pneumokokkenimpfung Vorgehen in der MHH November 2013
Erstimpfung Konjugatimpfstoff Pneumovax vorgeimpfte Patienten Konjugatimpfung nach 5-10 Jahren (?) Konjugat vorgeimpfte Patienten Konjugatwiederimpfung nach ? Jahren Patienten nach Pneumonie Impfung ab 4 Wochen nach Krankenhausentlassung Patienten nach Splenektomie Impfung noch im (!) Krankenhaus Pneumokokken- und Influenzaimpfung parallel möglich
 Konjugat vorgeimpfte Patienten. Konjugatwiederimpfung nach Jahren. Patienten nach Pneumonie. Impfung ab 4 Wochen nach Krankenhausentlassung. Patienten nach Splenektomie. Impfung noch im (!) Krankenhaus. Pneumokokken- und Influenzaimpfung parallel möglich.")
42
Pertussis: Risikogruppen
Kinder Nicht oder unzureichend geimpft Säuglinge Erwachsene Risiko schwerer Komplikationen Immunität abnehmend Infektionsquelle zu 30-50% Familienmitglieder1) Erreger-Reservoir; keine natürliche oder impfbedingte Immunität 1) Bisgard K M et al, Pediatr Infect Dis J, 2004
 Erreger-Reservoir; keine natürliche oder impfbedingte Immunität. 1) Bisgard K M et al, Pediatr Infect Dis J,")
43
Dauer der Pertussis-Immunität
Schutz nach natürlicher Infektion 4-20 Jahre Schutz nach Ganzkeim-Pertussis-Impfung mindestens 3-5 Jahre, maximal 6-12 Jahre Schutz nach azellulärer-Pertussis-Impfung mindestens 5-6 Jahre, maximal ? lebenslange Immunität weder nach Pertussisinfektion, noch nach Impfung Symptomatic re-infection has been observed in adults and children, showing that naturally induced immunity is not life-long. Similarly, vaccine-acquired immunity wanes after 5–10 years without boosting. It is likely that previously vaccinated and previously infected individuals progress through several stages of declining protection against pertussis. Initially, there is protection against infection. Subsequently, susceptibility to infection develops, but protection against symptomatic disease is maintained. After this, individuals become susceptible to symptomatic disease. The longer the time since last vaccination, the more severe or typical the symptoms will be. The precise duration of naturally acquired immunty is undetermined. The duration of protection may differ between the various whole-cell vaccines, acellular vaccines and various schedules of administration. Protective immunity against pertussis provided by whole-cell vaccines appears to persist for at least 3–5 years, then progressively declines 6–10 years after vaccination.1-5 A limited amount of evidence suggests that most aP vaccines provide protection for at least 5 years after primary immunization with three or four doses.6-11 1. Jenkinson D. BMJ 1988;296,612–4. 2. Centers for Disease Control and Prevention. MMWR 1993;42:952–53/59– Bass JW, Stephenson SR. Pediatric Infect Dis J 1987;6:141–4. 4. Cattaneo LA, et al. J Infect Dis 1996;173:1256–9. 5. Aoyama T, et al. Acta Paediatr Jpn 1995;37:321–4. 6. Taranger J, et al. Pedatr Infect Dis J 1997;16:180–4. 7. Storsaeter J, Olin P. Vaccine 1992;10:142–4. 8. Tinfberg Y, et al. Pediatr Infect Dis J 1999;18:361–5. 9. Liese JG, et al. 40th ICAAC, 2000;abstract Lugauer S, et al. Eur J Pediatr 2002;161(3):142– Salmaso S, et al. Pediatrics 2001;108:e81. 1. Jenkinson, 1988; 2. CDC, 1993; 3. Bass & Stephenson, 1987; 4. Cattaneo et al, 1996; 5. Aoyama et al, 1995; 6. Taranger et al, 1997; 7. Storsaeter & Olin, 1992; 8. Tinfberg et al, 1999; 9. Liese et al, 2000; 10. Lugauer et al, 2002; 11. Salmaso et al, 2001 43
:142– Salmaso S, et al. Pediatrics 2001;108:e Jenkinson, 1988; 2. CDC, 1993; 3. Bass & Stephenson, 1987; 4. Cattaneo et al, 1996; 5. Aoyama et al, 1995; 6. Taranger et al, 1997; 7. Storsaeter & Olin, 1992; 8. Tinfberg et al, 1999; 9. Liese et al, 2000; 10. Lugauer et al, 2002; 11. Salmaso et al,")
44
Pertussis Erwachsene: nächste Td-Impfung: TdaP/TdaP-IPV
gebärfähige Frauen, Haushaltskontaktpersonen Neugeborener / chron. Kranker: letzte 10 Jahre keine Pertussis-Impfung: 1 Dosis TdaP/TdaP-IPV

45
Vielen Dank für Ihre Aufmerksamkeit!

Ähnliche Präsentationen



) www.capnetz.de Häufigkeit von Erregern der ambulant erworbenen.>")















 und Nichtinvasive Beatmung (NIV)>")