Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
3. Kurs Medikamentöse Tumortherapie
Kopf-Hals-Tumore: Lebensqualität, Sozioökonomische Aspekte, Qualitätssicherung Medikamentöse Tumortherapie Hamburg, S. Tribius Fachärztin für Strahlentherapie Palliativmedizin Universitätsklinikum Hamburg- Eppendorf

2
Inhalt Lebensqualität (QOL): Was macht Sinn?
Sozioökonomische Aspekte: Kosten sind nicht gleich WERT Qualitätssicherung (QA): Sicherheit und Konsequenzen
: Sicherheit und Konsequenzen.")
3
1) QOL: Was macht Sinn? Kopf-Hals-Tumore beeinflussen die QOL beträchtlich betreffen funktionell wichtige Bereiche; sind häufig kosmetisch auffällig QOL ist “ein globales Konstrukt, das das generelle Befinden der Patienten in Bezug auf die Erkrankung und die Therapie widerspiegelt QOL Instrumente- “alphabet soup”! Cancer-specific: … FACT-G, EORTC QLQ C30 HNC-specific: … FACT-HN, EORTC QLQ HN35, HNQOL, PSS-HNC, UWQOL

4
QOL: Optimierung ist notwendig
Erhebung der sog health-related QOL (HRQOL) – Effekt der Erkrankung und der Therapie auf die QOL mehr spezifische Instrumente– derzeit fehlt eine direkte Korrelation zwischen funktionellen Defiziten und global QOL scores Langzeitbeobachtungen fehlen (z.B. Longitudinal alle 6 Monate über >3 Jahre) und not miss data points “ the Devil hides in missing data” Alle prospektiven Studien sollten die Erhebung der QOL einbeziehen
 – Effekt der Erkrankung und der Therapie auf die QOL. mehr spezifische Instrumente– derzeit fehlt eine direkte Korrelation zwischen funktionellen Defiziten und global QOL scores. Langzeitbeobachtungen fehlen (z.B. Longitudinal alle 6 Monate über >3 Jahre) und not miss data points the Devil hides in missing data Alle prospektiven Studien sollten die Erhebung der QOL einbeziehen.")
5
Fall: Patient JD männlich, 43 Jahre alt Verheiratet berufstätig
wenig Nikotin (py) gelegentlich Alkohol kein Gewichtsverlust SCC rechte Tonsille Dx 10/11/2010 cT1 (15mmm) N2b M0, Stadium IVa 4cm zystisches LK-Konglomerat Level II 2 weitere LK < 1cm p16+, HPV 16+
 gelegentlich Alkohol. kein Gewichtsverlust. SCC rechte Tonsille. Dx 10/11/2010. cT1 (15mmm) N2b M0, Stadium IVa. 4cm zystisches LK-Konglomerat Level II. 2 weitere LK < 1cm. p16+, HPV 16+")
6
Cited Among Top 3 Priorities
What Do Patients Want? Item/Goal SCCHN (patients; %) Controls (non patients; %) Cure of my cancer 90 80 Living as long as possible 61 60 Having no pain 34 52 Returning to activities quickly 27 21 Normal energy level 23 20 Being able to swallow normally 18 Keeping my natural voice 15 8 Patients and controls were asked to prioritize potential outcomes when making treatment decisions. The top 3 ranked priorities in both groups were “being cured of cancer”, “living as long as possible” and “having no pain”. Controls had no prior personal diagnosis or treatment for SCCHN or any other cancer (except skin cancer). Compared with the control group, patients more frequently ranked “being cured of cancer” (90% vs 80%, respectively). However, patients accepted a certain degree of pain compared to nonpatients. Only 34% of patients ranked “having no pain” compared to 52% of the controls. [List p168, Table 4]. List et al, 2004 6
 Controls. (non patients; %) Cure of my cancer Living as long as possible Having no pain Returning to activities quickly Normal energy level Being able to swallow normally. 18. Keeping my natural voice Patients and controls were asked to prioritize potential outcomes when making treatment decisions. The top 3 ranked priorities in both groups were being cured of cancer , living as long as possible and having no pain . Controls had no prior personal diagnosis or treatment for SCCHN or any other cancer (except skin cancer). Compared with the control group, patients more frequently ranked being cured of cancer (90% vs 80%, respectively). However, patients accepted a certain degree of pain compared to nonpatients. Only 34% of patients ranked having no pain compared to 52% of the controls. [List p168, Table 4]. List et al,")
7
Mögliche Therapiealternativen für JD
TPF Induktion + definitive Radiochemotherapie Definitive Radiochemotherapie Radioimmuntherapie Primäre OP± adjuvante RT

8
No pain, no gain?

9
Pain TPF: Sepsis, Mukositis, Neutropenie, CRT verzögert
R(C)T/ R(I)T: Xerostomie, Dysphagie, Mucositis, Dermatitis, Gewichtsverlust Primäre OP± adjuvante (C)RT: Funktion?± Xerostomie QOL erheblich beeinflusst: Braucht Patient JD das?
T/ R(I)T: Xerostomie, Dysphagie, Mucositis, Dermatitis, Gewichtsverlust. Primäre OP± adjuvante (C)RT: Funktion ± Xerostomie. QOL erheblich beeinflusst: Braucht Patient JD das")
10
5-fold increase in toxicity burden Increased treatment intensity
9914 100 200 300 400 9911 9111 9703 Relative-value scale 9703 9703 9501 9003 9003 Please add a refererce Trotti et al, Lancet Oncology 2007 9111 9003 9000 9003 Increased treatment intensity Standard postoperative radiotherapy alone Hyperfractionated radiotherapy alone Concomitant boost radiotherapy alone Standard radiotherapy alone Standard radiotherapy alone: larynx Split-course accelerated radiotherapy alone Concurrent chemoradiotherapy (P) Concurrent chemoradiotherapy (P and 5-FU) Concurrent chemoradiotherapy (H and 5-FU) Concurrent chemoradiotherapy (P and PA) Induction chemoradiotherapy (P and 5-FU) and standard radiotherapy: larynx Concurrent chemoradiotherapy (P): larynx Concurrent chemoradiotherapy (P) with concomitant boost radiotherapy Trial group Trotti et al, Lancet Oncology 2007
 Concurrent chemoradiotherapy. (P and 5-FU) Concurrent chemoradiotherapy. (H and 5-FU) Concurrent chemoradiotherapy. (P and PA) Induction chemoradiotherapy (P and 5-FU) and standard radiotherapy: larynx. Concurrent chemoradiotherapy. (P): larynx. Concurrent chemoradiotherapy (P) with concomitant boost radiotherapy. Trial group. Trotti et al, Lancet Oncology")
11
RTOG 0129 OS by HPV Status 3-year difference 26%, 12–40
100 3-year difference 26%, 12–40 75 Overall survival (%) 50 Log-rank p<0.001 HPV +ve HPV –ve 25 1 2 3 4 5 Years after randomisation Patients at risk HPV +ve HPV –ve 206 117 193 89 180 76 162 64 119 34 30 9
 50. Log-rank p< HPV +ve. HPV –ve Years after randomisation. Patients at risk. HPV +ve. HPV –ve")
12
Ergebnis HPV assoziierte Oropharynkarzinome unterschieden sich von den sog. klassischen OPC Medianes F/U 4.8 Jahre: 3-y OS: 82.4% in HPV+ and 57.1% in HPV- HPV ist ein unabhängiger prognostischer Faktor für OS K. Ang et al. N. Eng. J. Med. 2010; 363: 24-35

13
Gain : Was ist die optimale Therapie für JD?
HPV-assoziierte Oropharynxkarzinome- was heißt “De-intensification” der Therapie? Ist die primäre Operation noch immer eine valide Option? Ist die R(C)T nötig? Genügt eine alleinige RT? Wieviel RT ist ausreichend? (Dosis? Volumen?)
T nötig Genügt eine alleinige RT Wieviel RT ist ausreichend (Dosis Volumen )")
14
Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer
K. Kian Ang, M.D., Ph.D., Jonathan Harris, M.S., Richard Wheeler, M.D., Randal Weber, M.D., David I. Rosenthal, M.D., Phuc Felix Nguyen-Tân, M.D., William H. Westra, M.D., Christine H. Chung, M.D., Richard C. Jordan, D.D.S., Ph.D., Charles Lu, M.D., Harold Kim, M.D., Rita Axelrod, M.D., C. Craig Silverman, M.D., Kevin P. Redmond, M.D., and Maura L. Gillison, M.D., Ph.D. N Engl J Med Volume 363(1):24-35 July 1, 2010
: July 1,")
15
“Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States”
“Results …..If recent incidence trends continue, the annual number of HPV-positive oropharyngeal cancers is expected to surpass the annual number of cervical cancers by the year 2020” Peters et al JCO May

16
Zukünftige klinische Studien…?
Prospectiv und stratifizieren nach HPV sollten QOL erheben Fallbeispiel JD – Low risk - long OS - Welche Therapie wird seine Lebensqualität am wenigsten nachhaltig negativ beeinflussen?

17
How to improve QOL for HPV survivors
How to improve QOL for HPV survivors? Research strategies to reduce toxicity Reduktion der Gesamtdosis der Bestrahlung Rolle der kombinierten Radiochemotherapie Rolle der Chirurgie mit neoadjuvanten Strategien Radioimmuntherapie statt Radiochemotherapie Induktionschemoptherapie und RT- Dosisreduktion bei CR Kombination!

18
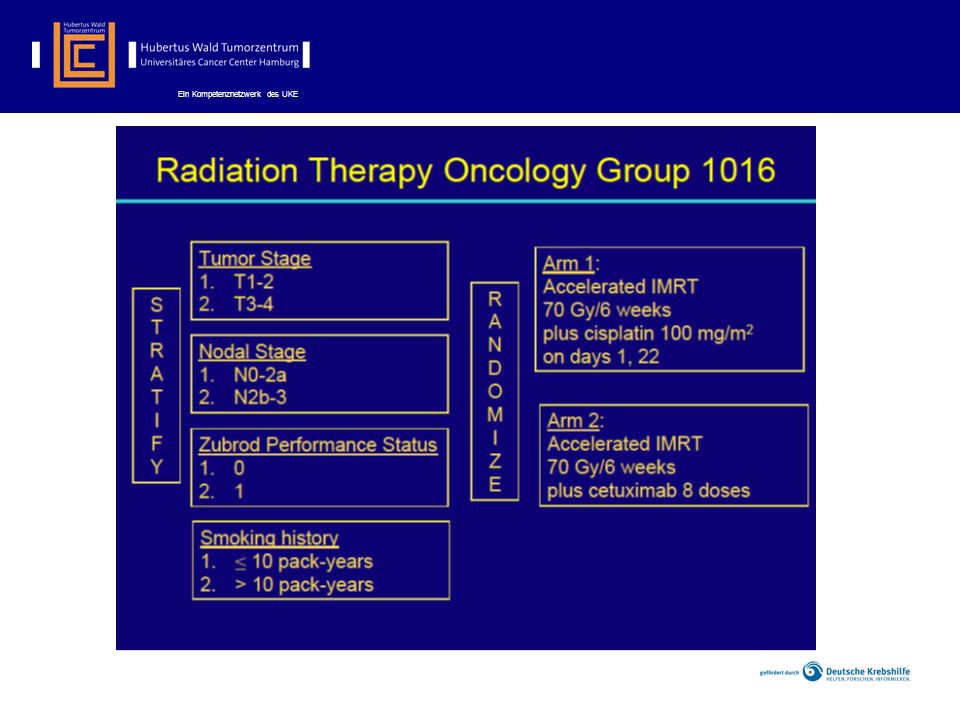
E1308: Using Chemotherapy to Select Patients for Lower Dose Radiation
Eligibility Stage: III, Iva,b resectable Site: Oropharynx only HPV 16 ISH +ve or p16 IHC +ve N=83 Concurrent IMRT 54 Gy + Cetuximab 250mg/m2/wk IMRT 69.3Gy Radiotherapy Cetuximab 250mg/m2 qwk REGISTRATION Induction (3 cycles) Paclitaxel 90mg/m2 qwk Cisplatin 75mg/m2 q21 Cetuximab 250mg/m2 qwk RESPONSE RESPONSE CR* Add the new box please with the arrow and < CR Can you make smaller the boxes ( “ crunch up) a little to make room top- bottom <CR**
 Paclitaxel. 90mg/m2 qwk. Cisplatin. 75mg/m2 q21. Cetuximab. 250mg/m2 qwk. RESPONSE. RESPONSE. CR* Add the new box please with the arrow and < CR Can you make smaller the boxes ( crunch up) a little to make room top- bottom. <CR**")
20
Secondary Outcomes To monitor and compare progression-free survival for “safety”. To compare patterns of failure (locoregional vs distant). To compare acute toxicity profiles (and overall toxicity burden). To compare overall quality of life (QOL) short-term (< 6 months) and long-term (2 years). To compare QOL Swallowing Domains short-term and long-term. To compare clinician-reported versus patient-reported CTCAE toxicity events. To explore differences in the cost effectiveness of cetuximab as compared to cisplatin. To explore differences in work status and time to return to work. To compare patient-reported changes in hearing. To compare audiometric assessment of hearing for ototoxicity. To compare CTCAE v. 4 late toxicity at 1, 2, and 5 years. To evaluate the effect of tobacco exposure (and other exposures) as measured by standardized computer-assisted self interview (CASI) on overall survival and progression-free survival. To pilot CASI collection of patient reported outcomes in a cooperative group setting. To determine whether specific molecular profiles are associated with overall or progression-free survival. To investigate associations between changes in serum biomarkers or HPV-specific cellular immune responses measured at baseline and three months with overall or progression-free survival.
. To compare overall quality of life (QOL) short-term (< 6 months) and long-term (2 years). To compare QOL Swallowing Domains short-term and long-term. To compare clinician-reported versus patient-reported CTCAE toxicity events. To explore differences in the cost effectiveness of cetuximab as compared to cisplatin. To explore differences in work status and time to return to work. To compare patient-reported changes in hearing. To compare audiometric assessment of hearing for ototoxicity. To compare CTCAE v. 4 late toxicity at 1, 2, and 5 years. To evaluate the effect of tobacco exposure (and other exposures) as measured by standardized computer-assisted self interview (CASI) on overall survival and progression-free survival. To pilot CASI collection of patient reported outcomes in a cooperative group setting. To determine whether specific molecular profiles are associated with overall or progression-free survival. To investigate associations between changes in serum biomarkers or HPV-specific cellular immune responses measured at baseline and three months with overall or progression-free survival.")
21
De-ESCALaTE HPV Determination of Epidermal growth factor receptor-inhibitor (cetuximab) versus Standard Chemotherapy (cisplatin) early And Late Toxicity Events in Human Papillomavirus-positive oropharyngeal squamous cell carcinoma Chief Investigator Hisham Mehanna
 early And Late Toxicity Events in. Human Papillomavirus-positive oropharyngeal squamous cell carcinoma. Chief Investigator. Hisham Mehanna.")
22
GLOBAL QUALITY OF LIFE DURING THE ACUTE TOXICITY PHASE OF PATIENTS WITH HEAD AND NECK CANCER: CAN WE IDENTIFY PATIENTS MOST AT RISK OF PROFOUND QUALITY OF LIFE DECLINE? Dr. med. Silke Tribius

23
QoL deteriorated significantly during therapy but many domains recovered in the 6–8 weeks after therapy Median QLQ-C30 score Better QoL Worse QoL *** ** *** *** *** ** *** *** *** *** *** *** Worse QoL Better QoL Before (C)RT End of (C)RT 6–8 weeks after (C)RT *p<0.01; *** p<0.0001
RT. End of (C)RT. 6–8 weeks after (C)RT. *p<0.01; *** p<")
24
Median HN35 score *** *** *** *** *** *** *** Worse QoL Better QoL
Before (C)RT End of (C)RT 6–8 weeks after (C)RT *** p<0.0001
RT. End of (C)RT. 6–8 weeks after (C)RT. *** p<")
25
Keine anderen prognostischen Faktoren für dieses Zeitintervall
QoL verschlechtert sich in mehr bei Patienten mit besserer Basis- QOL Global Health Status (score >median) Keine anderen prognostischen Faktoren für dieses Zeitintervall Poor QoL at baseline Good QoL at baseline
 Keine anderen prognostischen Faktoren für dieses Zeitintervall. Poor QoL at baseline. Good QoL at baseline.")
26
Intensity-modulated radiotherapy versus conventional and 3D conformal radiotherapy in patients with head and neck cancer: is there a worthwhile quality of life gain?

27
TomoTherapy®

28
Präzision in der Bestrahlungstechnik
Gy PTV larynx spinal cord brain stem r. parotid gland l. Parotid gland

29
2) Soziökonomische Aspekte
Patientenversorgung- 3 Arten von Kosten : direkte Kosten– Therapiekosten indirekte Kosten– Berufsunfähigkeit, Rente, Behinderung, Tod “Intangible” Kosten– QOL Wenige Daten für Patienten mit Kopf-Hals-Tumoren

30
Societal Cost of HNC: “ burden of disease” is always a big number
Lee at al Eur J Health Econom :70-80 Reference Country Parameter Year of reported costs Reported costs and base population size National burden of illness = societal cost Brown et al US Direct cost, morbidity cost, and mortality cost of cancers or the lip, oral, cavity and pharynx 1990 $US 943 million 250 million inhabitants Medicare expenditures for HNC 1996 $US 675 million 35 million beneficiaries Cronin et al Tx of annual incident HNC cases in US $US 976 million 280 million inhabitants Zavras et al Greece Tx of oral cancer 2001 $US 4.8 million 10 million inhabitants Ruff et al Germany Smoking related costs Oral cavity and pharynx Larynx 83 million inhabitants 771 million (total) €124 million (direct) €226 million (total) €47 million (direct)
 €124 million (direct) €226 million (total) €47 million (direct)")
31
Examples of Direct Costs - US
Patients with HNC caused significantly more direct cost than matched comparison patients without HNC Variable SCCHN cohort (n = 4536) Comparison cohort no SCCHN (n = 4536) Rate of hospitalisation (%) 82 55 Mean number of hospitalisations 2.5 1.4 Mean number of inpatient days 24 12 Rate of skilled nursing care use (%) 22 13 Mean number of days of skilled nursing care 9 5 Rate of home healthcare use (%) 48 26 Rate of resource use (%) 14 3 2004 SEER Medicare database study - Lang et al Arch Otolaryngol Head Neck Surg 2004; 130:
 Comparison cohort no SCCHN (n = 4536) Rate of hospitalisation (%) Mean number of hospitalisations Mean number of inpatient days Rate of skilled nursing care use (%) Mean number of days of skilled nursing care Rate of home healthcare use (%) Rate of resource use (%) SEER Medicare database study - Lang et al Arch Otolaryngol Head Neck Surg 2004; 130:")
32
Was bestimmt den WERT eines Gesundheitssystems?
Definition eines WERTES für Patienten sollte den GEWINN für alle “Akteure” im System darstellen korrelliert mit Ergebnissen, nicht Inputs, gemessen an Outcomes, nicht Prozessen Definiert als Outcome relativ zu Kosten Gesamtkosten müssen die Kosten des gesamten “Zyklus” der Versorgung für die jeweilige Erkrankung beinhalten Die Wahl der Therapie bestimmt die Gesamtkosten Pr Michael Porter, Harvard Business School, NEJM Dec

34
Dimensions of Value in Healthcare
Porter, M in NEJM

35
The Dimensions of Head and Neck Cancer
Porter, M in NEJM

36
Critical Impact of RT Protocol Compliance
Results From Study TROG N= 861 patients enrolled Methods: All RT plans and docs had post treatment review by Trial Management Committee for compliance Outcome data analyzed for protocol compliance and RT quality Results: 25% of patients had non-=compliant plans 47% of non-compliant plans had deficiencies affecting outcome Major deficiencies highly correlated with number of patients enrolled per centre (< 5 patients 30%; ≥ 20 patients 5%, P <. 001) Peters et al JCO May
 Peters et al JCO May")
37
For patients receiving at least 60 Gy:
Critical Impact of RT Protocol Compliance For patients receiving at least 60 Gy: RT Plan N = 2-year OS 2-year free loco-regional failure Major deficiencies 87 50% 54% Initially protocol compliant 502 70% 78% P<0.001 Conclusions: The critical importance of RT quality on outcome in CRT Centres treating few patients have major quality problems Peters et al JCO May

39
Herzlich Willkommen auf den Internet-Seiten der Strahlenschutzkommission Die Strahlenschutzkommission (SSK) berät das Bundesministerium für Umwelt, Naturschutz und Reaktorsicherheit (BMU) in allen Angelegenheiten des Schutzes vor ionisierenden und nicht-ionisierenden Strahlen. Als Vorsitzender der SSK freue ich mich über Ihr Interesse an Fragen des Strahlenschutzes. Auf den folgenden Seiten erhalten Sie Informationen über die Entstehungsgeschichte der SSK, ihre Zusammensetzung und ihre Aufgaben. Die Beratungsschwerpunkte der letzten Jahre werden ausführlich dargestellt, außerdem finden Sie eine Zusammenstellung der Beratungsergebnisse seit Besonders hingewiesen sei auf die ausführlichen Informationen über die Veröffentlichungen der SSK. Diese sind wie bisher über den Buchhandel erhältlich. Um der fachlich interessierten Öffentlichkeit eine schnelle Information zu ermöglichen, sind viele der aktuellen Stellungnahmen und Empfehlungen auch im Volltext wiedergegeben. Prof. Dr. Rolf Michel Vorsitzender der Strahlenschutzkommission
 berät das Bundesministerium für Umwelt, Naturschutz und Reaktorsicherheit (BMU) in allen Angelegenheiten des Schutzes vor ionisierenden und nicht-ionisierenden Strahlen. Als Vorsitzender der SSK freue ich mich über Ihr Interesse an Fragen des Strahlenschutzes. Auf den folgenden Seiten erhalten Sie Informationen über die Entstehungsgeschichte der SSK, ihre Zusammensetzung und ihre Aufgaben. Die Beratungsschwerpunkte der letzten Jahre werden ausführlich dargestellt, außerdem finden Sie eine Zusammenstellung der Beratungsergebnisse seit Besonders hingewiesen sei auf die ausführlichen Informationen über die Veröffentlichungen der SSK. Diese sind wie bisher über den Buchhandel erhältlich. Um der fachlich interessierten Öffentlichkeit eine schnelle Information zu ermöglichen, sind viele der aktuellen Stellungnahmen und Empfehlungen auch im Volltext wiedergegeben. Prof. Dr. Rolf Michel Vorsitzender der Strahlenschutzkommission.")
40
Danke!

Ähnliche Präsentationen









 = 5n 3 + n + 1000 für alle n a)Geben sie eine obere Schranke O(g(n)) an. b)Beweisen.>")



 in Germany elective subject for medical students during.>")






