Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Wann denke ich an Rheuma 1. Lernen im Internet 2. Beschwerden, Diagnostik, Therapie 3. Rheumatoide ArthritisRA 4. SpondylarthritisSpA 5. PsoriasisarthritisPsA 6. OsteoarthritisOA 7.OsteoporoseOpor PK MD 8/13

2
1. Lernen im Internet A)Lesezeichen B)Adressen C)Google Bilder D)Screendump./. Power Point E)Downloads If you want to learn, just teach !
Downloads If you want to learn, just teach !.")
3
A) Lesezeichen
 Lesezeichen")
6
B) Adressen www.eular.org http://www.rheumatology.org/ www.dgrh.de www.asas-group.org http://www.youtube.com/watch?v=E6tP4wP8ja M http://www.youtube.com/watch?v=E6tP4wP8ja M www.dr-kaltwasser.de
 Adressen v=E6tP4wP8ja M v=E6tP4wP8ja M")
11
2. Beschwerden, Diagnostik, Therapie DiagnoseBeschwerdenTherapie______ RAschmerzhaft geschwollene Fingergelenke; TJC SJC NSAR, NSAID`s SpA 3Mon, morgensteif, Rückenschmerz, Colitis, Uveitis DEMARDS: MTX, PsAPsoriasis, Arthritis Sulfosalazin,... milde bis schwere Schuppenflechte plus Gelenkentzündung Biologicals: OABewegungsschmerz der GelenkeMonoklonale nach Trauma oder VerschleißAntikörper Oposkeine Beschwerden bis FX WK Verdacht bei Postmenopause

12
Dosierung von NSAID`s in SpA

13
Halbwertszeitmax mg/Tag Ibuprofen1,8 - 3,52400 - 3200 Ketoprofen1,5 - 2,5200 - 300 Aceclofenac 4200 Diclofenac° 2 Celecoxib 8 - 12400 Etoricoxibca. 22 90 Meloxicamca. 20 15 Piroxicam30 - 60 20 Naproxen10 - 181000 Indomethacin 2150 - 200 Phenylbutazon50 - 100600

14
DEMARD`s: Disease Modifying Anti Rheumatic Drugs DosierungAbk. Methotrexat10 - 20 mg s.c. p.o.MTX Azathioprin2 - 2,5 mg / kg KG Sulfasalazin500 - 2000 mg wtl. Steiger.SSZ Cloroquin100 mg / Tag Hydroxycloroquin Leflunomid10 - 20 mg / Tag CyclophosphamidD-Penicillamin Ciclosporin2 x 100 mg Gold: z.B. Auranofin2 x 50 mg / Monat

15
Biologicals: Monoclonale Antikörper Abatacept (Orencia)Bristol-Mey. Squ TNF alpha Blocker: Adalimumab (Humira)AbbVie Ltd. Etanercept (Enbrel)Pfizer Infliximab (Remicade)Centocor CD 20 Antikörper: Rituximab (Rituxan)Biogen / Roche BAFF Inhibitor Belumimab (Benlysta)GlaxoSmithKline IL-1 Rezeptorantagonist: Anakinra(Kineret)Swed. Orph. Biov
AbbVie Ltd. Etanercept (Enbrel)Pfizer Infliximab (Remicade)Centocor CD 20 Antikörper: Rituximab (Rituxan)Biogen / Roche BAFF Inhibitor Belumimab (Benlysta)GlaxoSmithKline IL-1 Rezeptorantagonist: Anakinra(Kineret)Swed. Orph. Biov.")
16
3. RA Rheumatoide Arthritis Wann denke ich an RA Beschwerden der Patienten DiagnostikKlassifikationTherapie

17
Beschwerden bei V.a. RA schmerzhaft geschwollene Fingergelenke, die morgens geschwollen sind, die Beschwerden lassen nach 2 – 3 h nach. mehr als 2 Fingergelenke betroffen und das länger als 6 Wochen

18
3. Rheumatoide ArthritisRA WIN und HOT what is new how to treat personal account: EULAR Madrid 2013 Beschwerden des Patienten DiagnostikTherapie

19
Target Population of the Criteria

20
2010 ACR/EULAR Classification Criteria for RA JOINT DISTRIBUTION (0-5) 1 large joint 0 2-10 large joints1 1-3 small joints (large joints not counted)2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA What if the score is <6? Patient might fulfill the criteria… Prospectively over time (cumulatively) Retrospectively if data on all four domains have been adequately recorded in the past
 Retrospectively if data on all four domains have been adequately recorded in the past.")
21
Classification vs. Diagnosis We don’t have diagnostic criteria for RA Typically in rheumatic diseases, criteria are labeled as “classification” criteria – These are helpful in defining homogeneous treatment populations for study purposes A clinical “diagnosis” has to be established by the physician (rheumatologist) – It includes many more aspects than can be included in formal criteria – Formal classification criteria might be a guide to establish a clinical diagnosis
 – It includes many more aspects than can be included in formal criteria – Formal classification criteria might be a guide to establish a clinical diagnosis.")
22
Definitions ≥6 = definite RA JOINT DISTRIBUTION (0-5) 1 large joint0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of “JOINT INVOLVEMENT” - Any swollen or tender joint (excluding DIP of hand and feet, 1st MTP, 1st CMC) - Additional evidence from MRI / US may be used for confirmation of the clinical findings
 1 large joint large joints small joints (large joints not counted) small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of JOINT INVOLVEMENT - Any swollen or tender joint (excluding DIP of hand and feet, 1st MTP, 1st CMC) - Additional evidence from MRI / US may be used for confirmation of the clinical findings")
23
Definitions JOINT DISTRIBUTION (0-5) 1 large joint0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA Definition of “SMALL JOINT” MCP, PIP, MTP 2-5, thumb IP, wrist NOT: DIP, 1 st CMC, 1 st MTP
 1 large joint large joints small joints (large joints not counted) small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA Definition of SMALL JOINT MCP, PIP, MTP 2-5, thumb IP, wrist NOT: DIP, 1 st CMC, 1 st MTP")
24
Definitions JOINT DISTRIBUTION (0-5) 1 large joint0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA Definition of “SMALL JOINT” MCP, PIP, MTP 2-5, thumb IP, wrist NOT: DIP, 1 st CMC, 1 st MTP
 1 large joint large joints small joints (large joints not counted) small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA Definition of SMALL JOINT MCP, PIP, MTP 2-5, thumb IP, wrist NOT: DIP, 1 st CMC, 1 st MTP")
25
Definitions ≥6 = definite RA JOINT DISTRIBUTION (0-5) 1 large joint0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of “LARGE JOINT” Shoulder, elbow, hip, knee, ankles
 1 large joint large joints small joints (large joints not counted) small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of LARGE JOINT Shoulder, elbow, hip, knee, ankles")
26
JOINT DISTRIBUTION (0-5) 1 large joint0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA Definition of “>10 JOINTS” -At least one small joint -Additional joints include: temporomandibular, sternoclavicular, acromioclavicular, and others (reasonably expected in RA) Definitions
 1 large joint large joints small joints (large joints not counted) small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA Definition of >10 JOINTS -At least one small joint -Additional joints include: temporomandibular, sternoclavicular, acromioclavicular, and others (reasonably expected in RA) Definitions")
27
≥6 = definite RA JOINT DISTRIBUTION (0-5) 1 large joint 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of “SEROLOGY” Negative: ≤ULN (for the respective lab) Low positive: >ULN but ≤3xULN High positive: >3xULN
 1 large joint large joints small joints (large joints not counted) small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of SEROLOGY Negative: ≤ULN (for the respective lab) Low positive: >ULN but ≤3xULN High positive: >3xULN")
28
Definitions ≥6 = definite RA JOINT DISTRIBUTION (0-5) 1 large joint0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of “SYMPTOM DURATION” Refers to the patient’s self-report on the maximum duration of signs and symptoms of any joint that is clinically involved at the time of assessment.
 1 large joint large joints small joints (large joints not counted) small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 Definition of SYMPTOM DURATION Refers to the patient’s self-report on the maximum duration of signs and symptoms of any joint that is clinically involved at the time of assessment.")
29
RA Diagnostik Inspektion und Palpation der Fingergelenke, wenn diese schmerzhaft geschwollen sind Rö Hände und Füße bei V.a. RA Labor: BB, CRP, CCP, ENA, ANA, dsDNA, AK Borrelien, Yersinien, Clamydien

30
2010 ACR/EULAR Classification Criteria for RA JOINT DISTRIBUTION (0-5) 1 large joint 0 2-10 large joints1 1-3 small joints (large joints not counted)2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA What if the score is <6? Patient might fulfill the criteria… Prospectively over time (cumulatively) Retrospectively if data on all four domains have been adequately recorded in the past
 Retrospectively if data on all four domains have been adequately recorded in the past.")
31
RA Therpie Feuer sofort und dauerhaft löschen, jeder Schub zerstört Gelenkstrukturen ! NSAID `sCortison, Lyrica DEMARDSBiologicals

32
4. SpondylarthritisSpA Wann denke ich an Spondylarthritis Beschwerden der Patienten DiagnostikKlassifikationTherapie

33
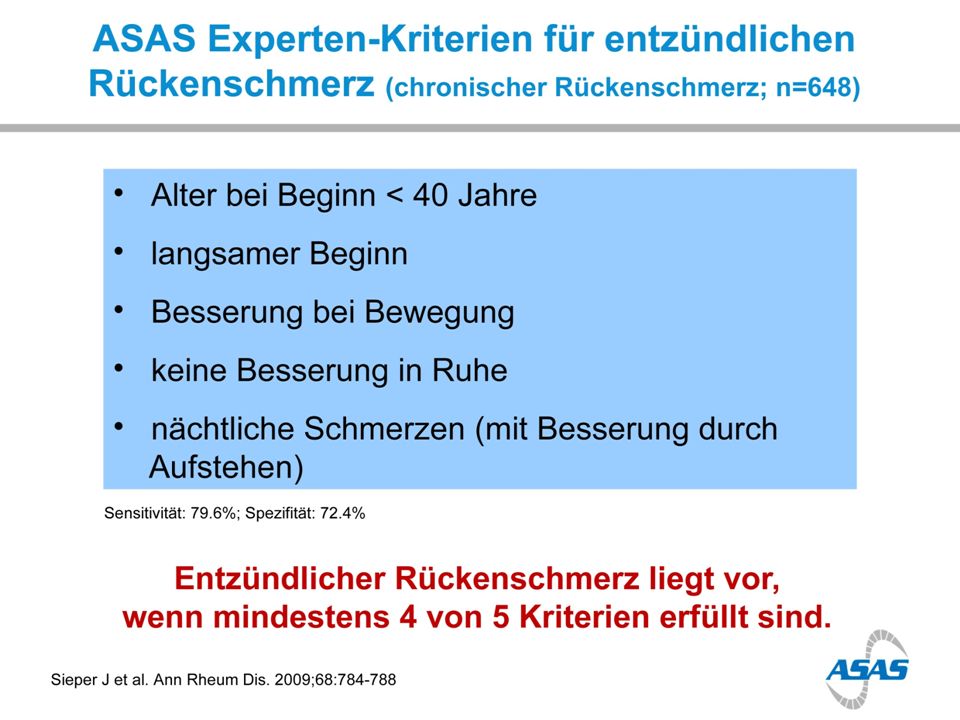
Klagen der Patienten Nächtlicher Rückenschmerz, Schlafstörung Morgentlicher Schmerz / Steifigkeit der WS Besserung in Verlauf des Morgens Fragen des Doktors Wurstförmige Finger / Zehen:Daktylitis Fersen schmerzh. Geschw.:Enthesitis Urethritis / Cervizitis M. Crohn, Blanitis, Uveitis

34
SPA Diagnostik Anamnese, Anamnese, Anamnese; MRI: ISG bds. STIR (bei V.a. Sakroiliitis) Labor:CRP, BSG; (HLA B27) U Ortho:FBA, Schober; WS Rot. / Neig.; lumb. Muskulatur tasten periphere Gelenke, Achillessehne Haut, Harnröhre, Uvea
 Labor:CRP, BSG; (HLA B27) U Ortho:FBA, Schober; WS Rot. / Neig.; lumb. Muskulatur tasten periphere Gelenke, Achillessehne Haut, Harnröhre, Uvea.")
38
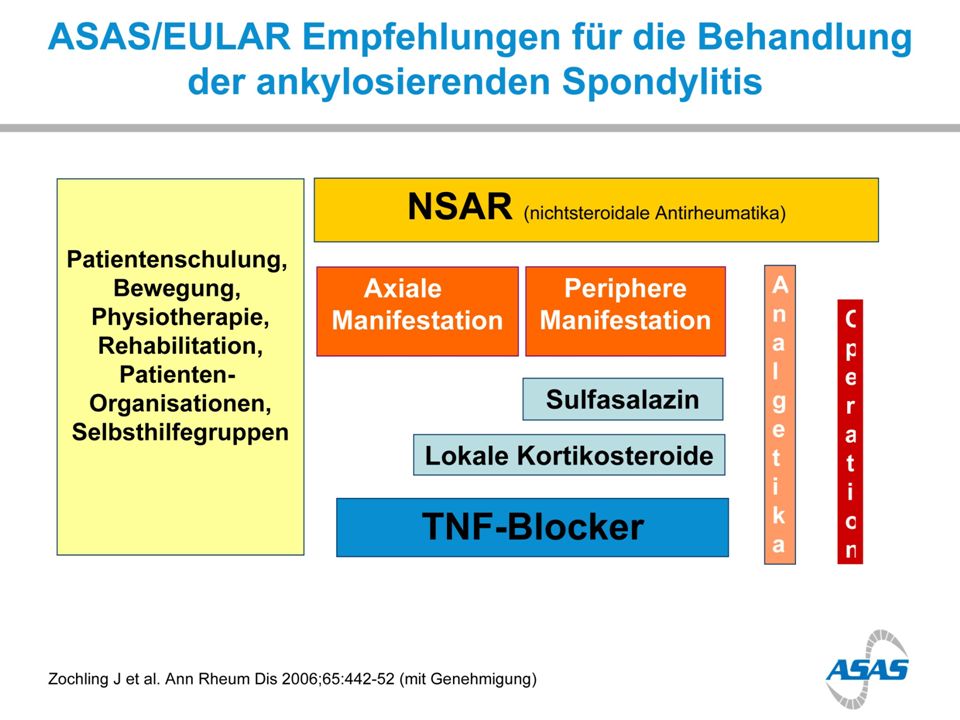
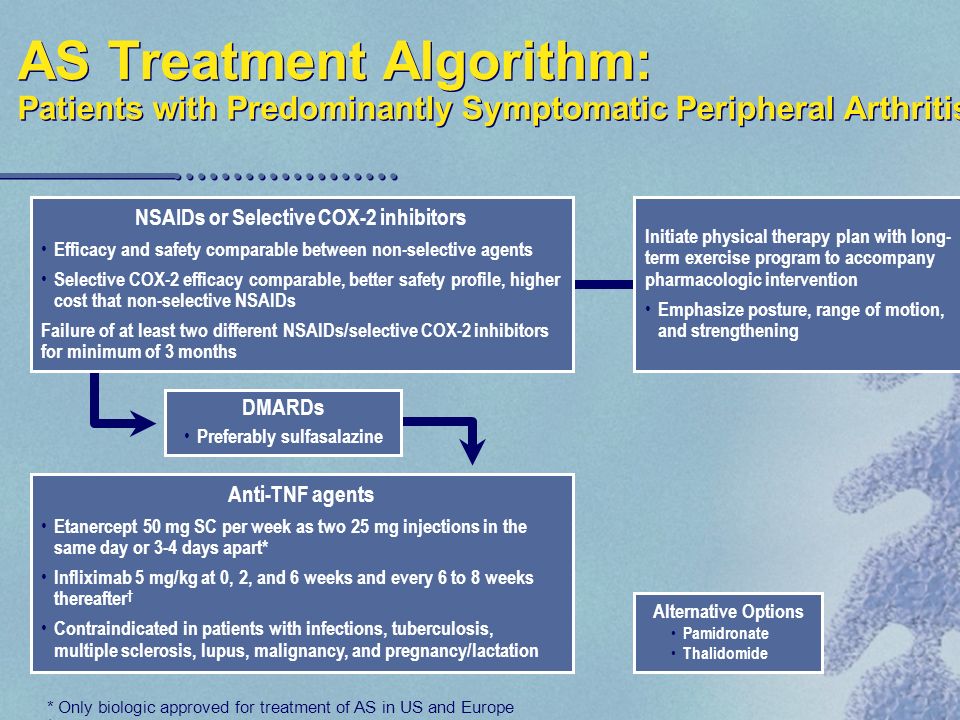
SpA Therapie Multimodal es droht Erwerbsunfähigkeit ! Aufklärung, Beratung Physikalische Therapie: Mikrowelle, Reizstrom, Neuraltherapie, Reha Sport, „Kur beantragen“ Krankenkasse, Arbeitsamt, Rententräger Pharmakotherapie

39
Beispiel:

42
SpA Klassifikation Axiale Spondylarthritis Periphere Spondylarthritis

43
5. Psoriasis ArthritisPsA http://www.youtube.com/watch?E6tP4wP8jaM Wann denke ich an Psoriasisarthritis Beschwerden der Patienten Diagnostik CASPAR Kriterien Therapie

44
Beispiel: Kr, Val; W 08.09.53 06.09.13ich Schmerzen Bein re, 2 Jahre Operation: Fragen:ganz genau: welches Gelenk, wann schmerzhaft, in Ruhe oder nach Bewegung; Schuppenflechte: vor 1J Hautarzt, Cortis. Augenentzündung x 2 in 3J Befund:Z.n. Psoriasis und Uveitis; seit 2 Mon Knie re, OSG re schmerz. gesch

45
Autoimmunerkrankungen Rheumatische Begleiterkrankungen Morbus Crohn, Colitis ulcerosa UveitisDactylitisPsoriasis Rheumatische (chron. entz.) Autoimmunerkrankg RA, SpA, PsA, SLE, Vaskulitiden, JRA,
 Autoimmunerkrankg RA, SpA, PsA, SLE, Vaskulitiden, JRA,.")
46
PsA Google Bilder

47
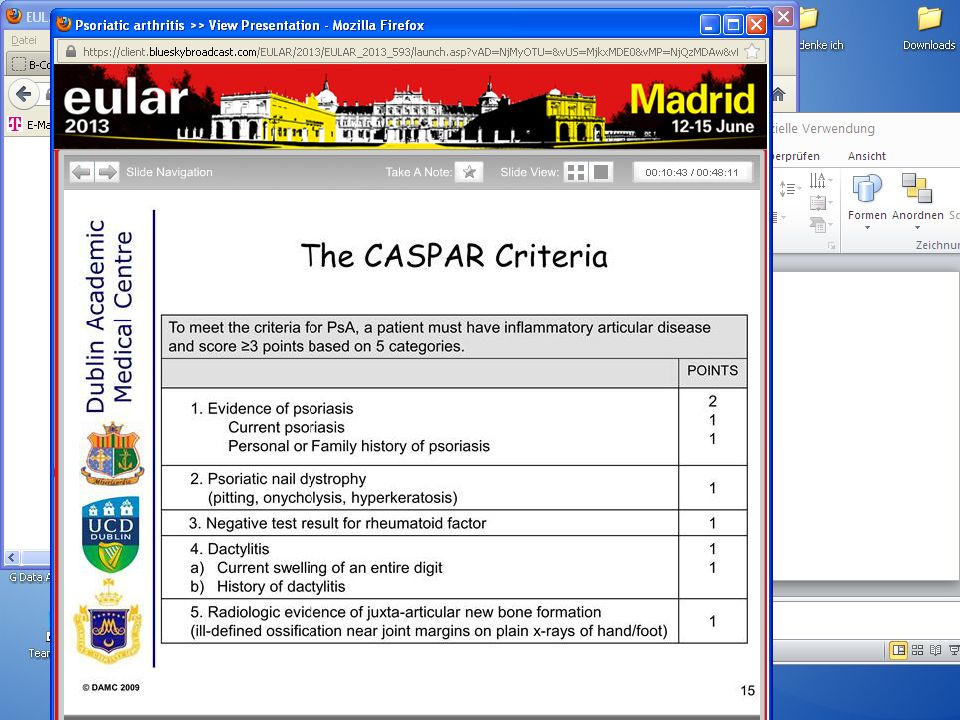
CASPAR Kriterien in PsA Um die diagnostischen Kriterien der PsA zu erfüllen, muss der Patient eine entzündliche Gelenkerkrankung haben und > 3 von max. 9 Punkten aus 5 Kategorien aufweisen Punkte 1. Nachweis einer Psoriasis entweder akut vorhanden oder pos. Fam. Anamnese und Psoriasis Vorgeschichte 2 1 2.Psoriatische Nageldystrophie (Pitting, Onychclyse, Hyperkeratose) 1 3. Rheumafaktor negativ (LABOR) 1 4.Dactylitis akute, entzündliche Schwellung eines ganzen Fingers Dactylitis in der Anamnese 1 5.Radiologische Zeichen einer periartikulaeren Knochenbildung (auf Roe Hand/Fuss undeutliche Ossifikation an Gelenkraendern) 1
 1 3. Rheumafaktor negativ (LABOR) 1 4.Dactylitis akute, entzündliche Schwellung eines ganzen Fingers Dactylitis in der Anamnese 1 5.Radiologische Zeichen einer periartikulaeren Knochenbildung (auf Roe Hand/Fuss undeutliche Ossifikation an Gelenkraendern) 1.")
50
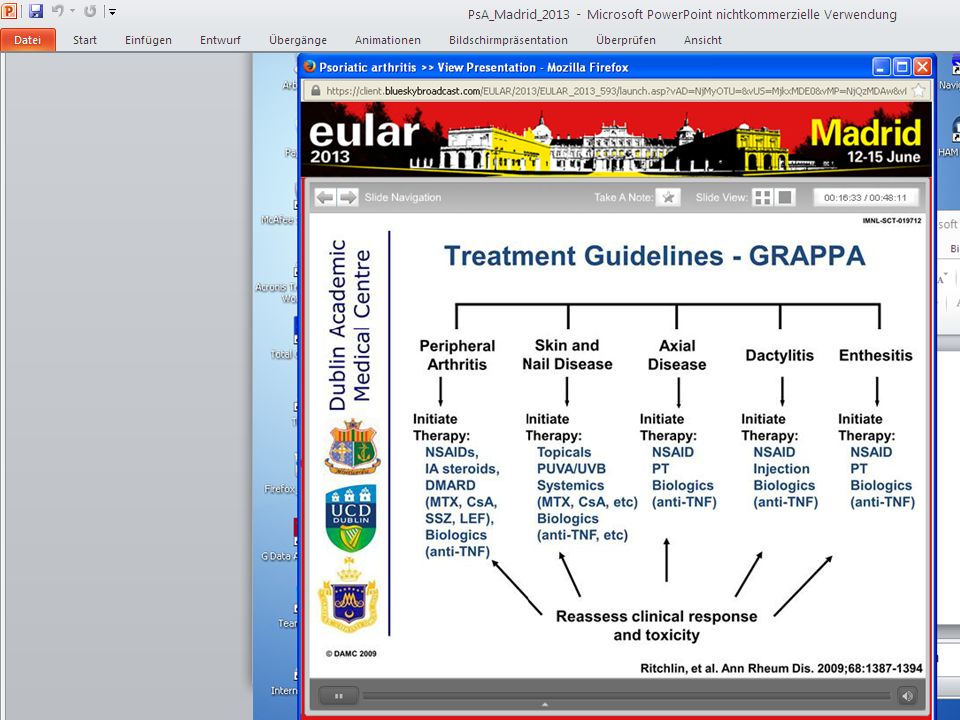
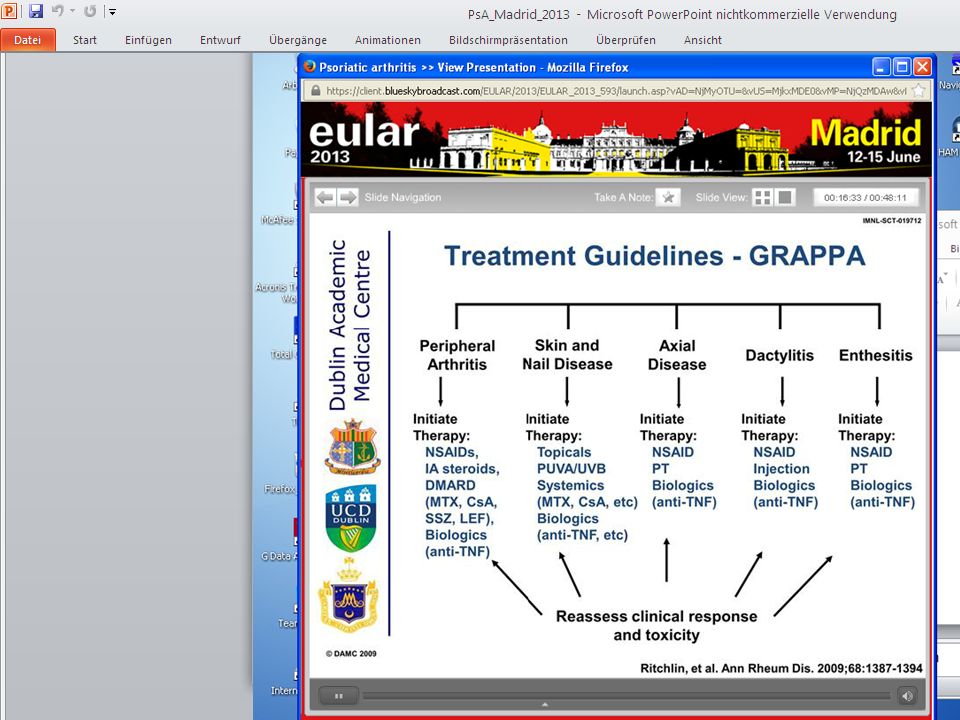
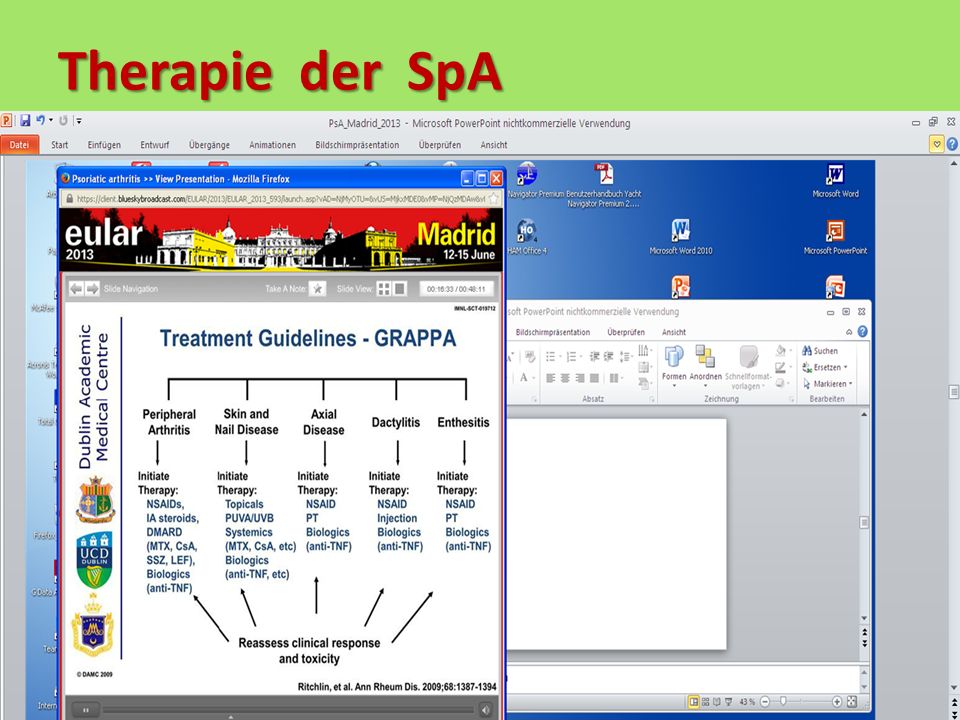
Therapie der SpA

53
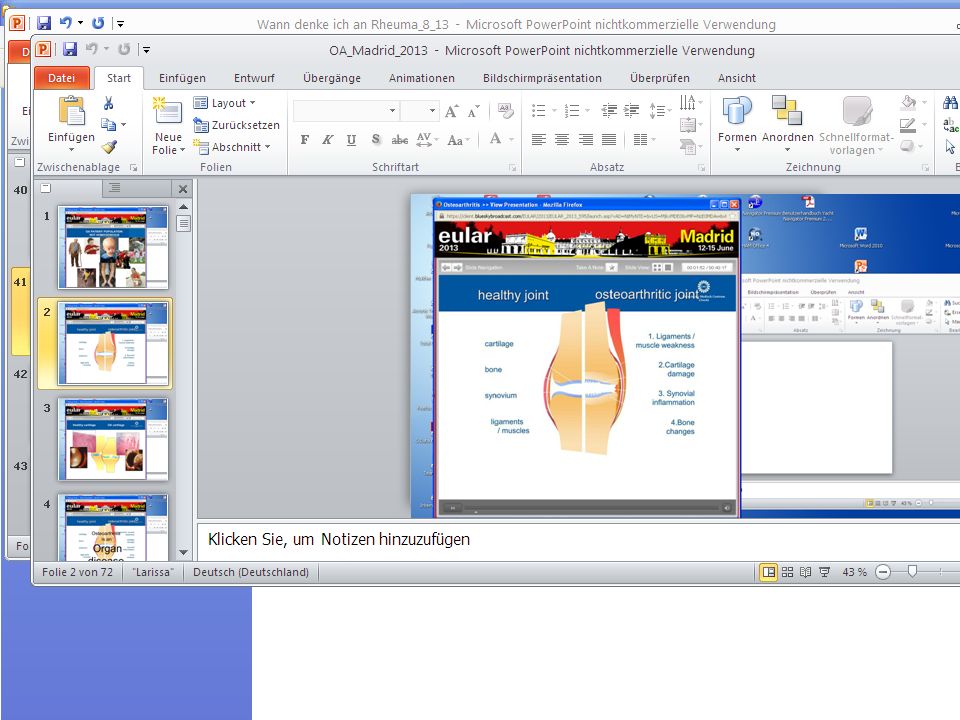
6. OsteoarthritisOA Wann denke ich an OA Beschwerden der Patienten DiagnostikTherapie

58
7. OsteoporoseOpor Wann denke ich an Osteoporose Beschwerden der Patienten DiagnostikTherapie

59
Wann denke ich an Osteoporose 1.Bei Frauen nach der Menopause 2.Bei Dauertherapie mit Cortison 3.Bei Z.n. Wirbelkörperfraktur 4.Bei Z.n. OS-Halsfraktur älterer Patienten

60
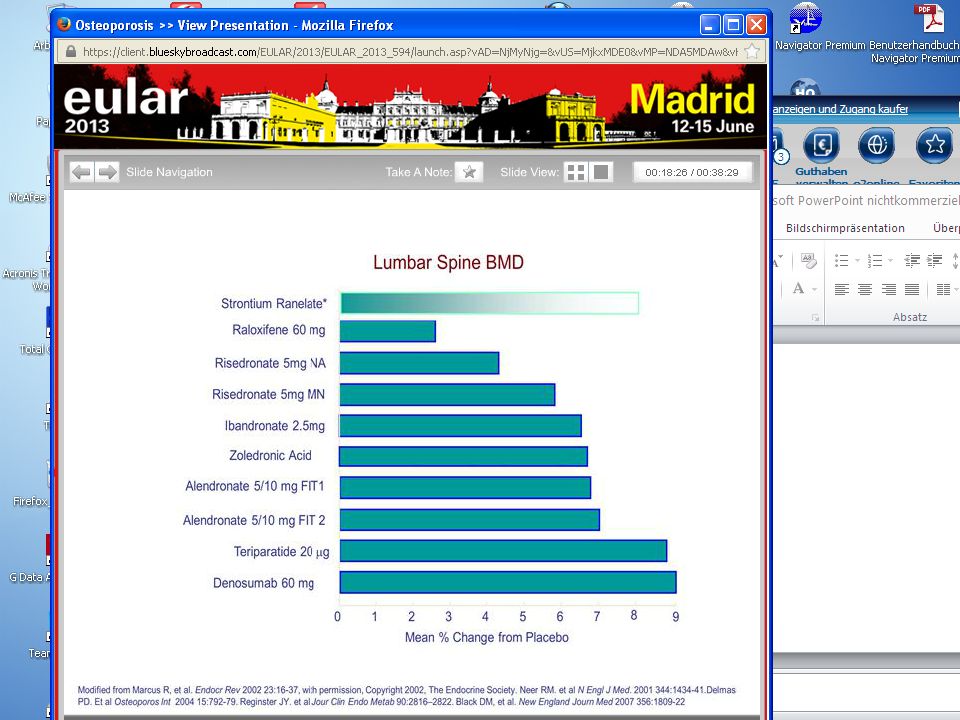
Beschwerden / Diagnostik Beschwerden:vor einer Fx WK oder OSH 0 Diagnostik:Rö BWS, LWS; Osteodensitometrie Vit. D Spiegel ? Therapie:Vit. D plus Ca 1000/ ResorptionshemmerOsteoblastenstimulationRaloxifen Strontium ?

62
Beschwerden / Diagnostik Beschwerden: keine Diagnostik:Rö Hüften, Wirbelkörper Osteodensitometrie Vitamin D Spiegel Therapie:Aufklärung / Beratung LebenswandelMedikamente

65
Zusammenfassung take home message 1.RA: autoimmune Entzündung der kleinen Fingergelenke kleinen Fingergelenke 2. SpA:autoimmune Entzündung der WS mit / ohne Gelenkbeteiligung 3. PsA:autoimmune Erkrankung der Haut und chaotischer Gelenkbeteiligung 4. OA:Verschleiß der „Organs“ Gelenk 5. OsPo:aktivitäts- und hormonell bedingter Verlust von Knochenmasse

Ähnliche Präsentationen















 but young men are no.>")

 Fluxgate: noise + distortion gets worse than the searchcoil at ~ 6 Hz. Searchcoil:>")



>")




