Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Die komplizierten Infekte in der Praxis
Stefan Zimmerli Universitätsklinik für Infektiologie Inselspital 3010 Bern

2
Background ESKAPE-Problemkeime
E nterococcus Gram-positive Bakterien S taphylococcus aureus K lebsiella Gram-negative Bakterien A cinetobacter P seudomonas E nterobacter Bei allen diesen Keimen zunehmende Antibiotika-Resistenz und wenige Behandlungsoptionen Boucher et al, CID 2009;48:1.

3
Resistenz in verschiedenen Pathogenen
Gram-positive Bakterien Gram-negative Bakterien Mykobakterien (zB MDR-Tuberkulose) Pilze (zB Candida spp. und Fluconazol) Protozoen (zB Plasmodium spp. und Chloroquin) Viren (zB HIV und antiretrovirale Medikamente)
 Pilze (zB Candida spp. und Fluconazol) Protozoen (zB Plasmodium spp. und Chloroquin) Viren (zB HIV und antiretrovirale Medikamente)")
4
Epidemiologie resistenter Keime Schweiz 2004 - 2014
19.6% BAG Bulletin 35; 24. August 2014

5
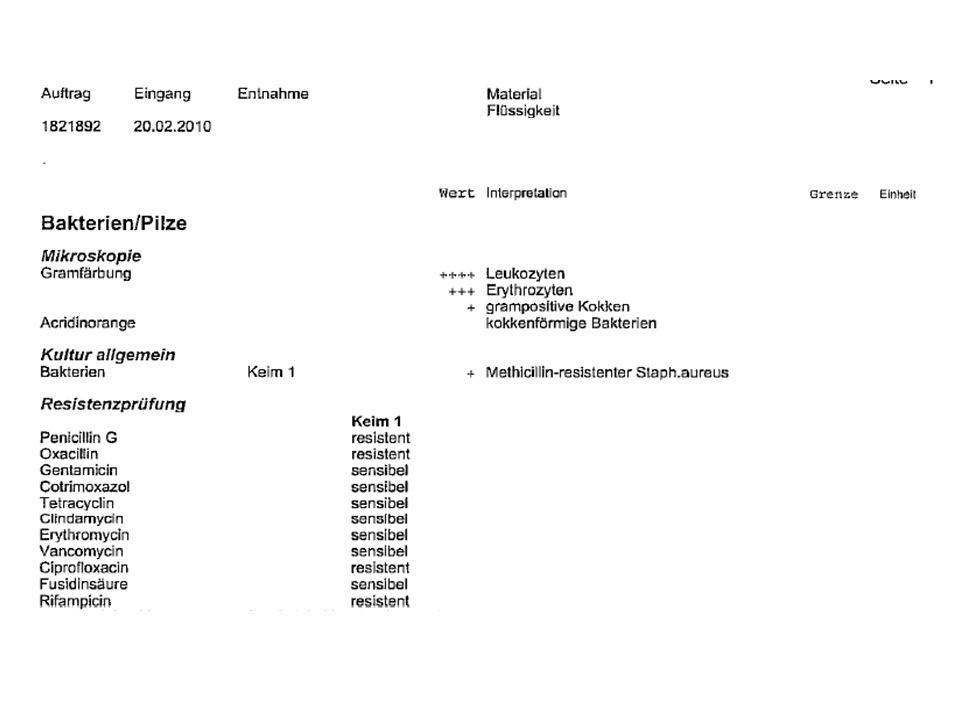
Furunkulose mit MRSA

7
Proportion of Methicillin Resistant S
Proportion of Methicillin Resistant S. aureus (MRSA) Isolates in Participating Countries, in 2006 and 2012 (Methicillin-Resistenz als Marker für alle Betalaktam-Antibiotika)
 Isolates in Participating Countries, in 2006 and (Methicillin-Resistenz als Marker für alle Betalaktam-Antibiotika)")
8
Proportion of MRSA Isolates in Switzerland, 2008 and 2012
West 17.5% Central 5.8% East (incl. Ticino) 4.7% Central 4.8% East 4.5% West 11.3% Ticino 19.7%
 4.7% Central. 4.8% East. 4.5% West. 11.3% Ticino. 19.7%")
9
MRSA (Methicillin-resistenter S. aureus)
Staphylococcus HA-MRSA CA-MRSA aureus (MSSA) Methicillin S R R Clindamycin S R S/R Erythromycin S R S/R Gentamicin S R S Rifampicin S R S TMP/SMX S R S Vancomycin S S S Fusidinsäure S R S Teicoplanin S R S CA-MRSA jünger und mehr Weichteilinfekte S = sensibel, R = resistent, HA = hospital acquired, CA = community acquired
 Methicillin S R R. Clindamycin S R S/R. Erythromycin S R S/R. Gentamicin S R S. Rifampicin S R S. TMP/SMX S R S. Vancomycin S S S. Fusidinsäure S R S. Teicoplanin S R S. CA-MRSA jünger und mehr Weichteilinfekte. S = sensibel, R = resistent, HA = hospital acquired, CA = community acquired.")
10
MRSA-Prävalenz Schweiz, hospitalisierte vs. ambulante Patienten
%

11
MRSA am Inselspital 1991 –

12
Know your hospital’s antibiogram! Beispiel eines US-Unispitals
46% der S. aureus-Isolate sind methicillin-sensibel Patient mit V.a. Endokarditis und Gram-positiven Kokken in der Blutkultur Welches empirische Antibiotikum? Toolbook, BJH, St. Louis, Missouri, 2013

13
MRSA Krankheitsbilder Haut- und Weichteilinfekte Sepsis, Endokarditis Pneumonie Septische Arthritis, Osteomyelitis Impetigo Therapieoptionen: Vancomycin (iv) Daptomycin (iv) Bactrim (po) Clindamycin (po, iv)
 Daptomycin (iv) Bactrim (po) Clindamycin (po, iv)")
14
Grundsätzliches zur MRSA Dekolonisation
Die Dauer beträgt 5 Tage und wird an 5 aufeinanderfolgenden Tagen vorge- nommen. Für die Dekolonisation werden Desinfektionsmittel und Antibiotikum lokal angewendet. Auf der Rückseite ist eine genaue Anweisung zur Anwendung der einzelnen Präparate beschrieben. Alle Präparate sind in der Schweiz geprüft und zugelassen. Bitte nur die rezeptierten Präparate verwenden. Falls möglich, für die Körperdusche Fremdkörper wie z. B. Fingerringe, Ohrenringe und Piercings entfernen. Diese vor dem Anziehen mit 70% Alkohol desinfizieren. Künstliche Fingernägel und Nagellack möglichst entfernen. Nach der ersten Dusche einmalig Kleider, Bettwäsche sowie Hand- und Badetücher wechseln. Träger von Perücken / Haartoupets desinfizieren deren Innenseite mit 70% Alkohol einmal täglich. Falls möglich, Nassrasuren und jegliche Haarentfernungen (Achselhöhle, Intimbereich, Beine) während der Dekolonisation vermeiden.
 während der Dekolonisation vermeiden.")
15
Grundsätzliches zur MRSA Dekolonisation
Nebenwirkungen Hautirritationen sind grundsätzlich möglich, jedoch selten. Bei Verdacht auf eine Unverträglichkeit oder Nebenwirkung die Spitalhygiene kontaktieren. Eine Aufnahme der einzelnen Substanzen erfolgt, falls überhaupt, nur in geringsten Mengen und ist medizinisch unbedenklich. Schwangerschaft und Stillzeit stellen keine Kontraindikation dar und sind unbedenklich. Kontrollabstriche und Entisolation Die Kontrollabstriche erfolgen nach Verordnung der Spitalhygiene oder des Arztes. Eine Entisolation erfodert mehrere negative Abstriche über einen Zeitraum von mindestens 3-6 Monaten.

16
Anweisung zur MRSA Dekolonisierung für Patienten
Anwendung Intervall Präparat Anweisung für die Anwendung Duschen 1x Tag Hibiscrub® Haut vollständig vor dem Gebrauch des Hibiscrub benetzen. Hibiscrub auf der gesamten Körperoberfläche mit den Händen verteilen. Am Kopf beginnen und danach den Körper von oben nach unten einseifen. Pro Körpterteil (Kopf, pro Arm, Bein, Oberkörper, Bauch ect.) je einen Dispenserhub verwenden. Am 1., 3. und 5. Tag die Haare ebenfalls mit Hibiscrub einseifen. Den Hautfalten im Gesicht, Achselhöhlen, Leisten und Intimbereich besondere Aufmerksamkeit schenken. Hibiscrub vor dem Abduschen während Sekunden einwirken lassen. Bei Säuglingen ≤ 6 Monate analog verfahren. Anstelle von Hibiscrub jedoch Octenisan verwenden. Patienten welche nicht duschen können, waschen den ganzen Körper mit derselben Menge an Hibiscrub und mit derselben Verweildauer. Mund 3x Tag Dentohexin Gurgellösung® 3x täglich den Mund mit Dentohexin Gurgellösung (5ml in 5ml Wasser aufgelöst) während 20 Sekunden spülen. Jeweils während des Spülens 5-10 Sekunden gurgeln. Dentohexin Gurgellösung ausspucken. Zahnprothese immer vor dem Spülen entfernen. Diese in gereinigtem Zustand einmal pro Tag während 5 Minuten in Dentohexin Gurgellösung ® einlegen. Nase 3xTag Bactroban® Nasensalbe 1cm der Salbe auf ein Wattestäbchen auftragen und damit die Nasenöffnung ausstreichen. Gleiches Prozedere für die 2. Nasenöffnung. Bei Schnupfen die Nase vor der Behandlung putzen und nach Salbenapplikation möglichst lange auf das Putzen der Nase zu verzichten. Wunden 2x Tag Betadine Lösung Mit sterilem Wattestäbchen gleichmässig auf die Wunde auftragen. Einwirkzeit: 2-3 Minuten oder bis eingetrocknet.
 je einen Dispenserhub verwenden. Am 1., 3. und 5. Tag die Haare ebenfalls mit Hibiscrub einseifen. Den Hautfalten im Gesicht, Achselhöhlen, Leisten und Intimbereich besondere Aufmerksamkeit schenken. Hibiscrub vor dem Abduschen während Sekunden einwirken lassen. Bei Säuglingen ≤ 6 Monate analog verfahren. Anstelle von Hibiscrub jedoch Octenisan verwenden. Patienten welche nicht duschen können, waschen den ganzen Körper mit derselben Menge an Hibiscrub und mit derselben Verweildauer. Mund. 3x Tag. Dentohexin Gurgellösung® 3x täglich den Mund mit Dentohexin Gurgellösung (5ml in 5ml Wasser aufgelöst) während 20 Sekunden spülen. Jeweils während des Spülens 5-10 Sekunden gurgeln. Dentohexin Gurgellösung ausspucken. Zahnprothese immer vor dem Spülen entfernen. Diese in gereinigtem Zustand einmal pro Tag während 5 Minuten in Dentohexin Gurgellösung ® einlegen. Nase. 3xTag. Bactroban® Nasensalbe. 1cm der Salbe auf ein Wattestäbchen auftragen und damit die Nasenöffnung ausstreichen. Gleiches Prozedere für die 2. Nasenöffnung. Bei Schnupfen die Nase vor der Behandlung putzen und nach Salbenapplikation möglichst lange auf das Putzen der Nase zu verzichten. Wunden. 2x Tag. Betadine Lösung. Mit sterilem Wattestäbchen gleichmässig auf die Wunde auftragen. Einwirkzeit: 2-3 Minuten oder bis eingetrocknet.")
17
Epidemiologie resistenter Keime Schweiz 2004 - 2014
BAG Bulletin 35; 24. August 2014

18
Epidemiologie resistenter Keime Schweiz 2004 - 2014
BAG Bulletin 35; 24. August 2014

19
Antibiotikaeinsatz bei ambulanten Patienten in DDD: Schweiz 2007
FIG. 1. Standardized DDD per 1000 inhabitants per day, for outpatient prescriptions in 2007 for all antibiotics and selected antibiotics for seven Swiss regions and Switzerland. Measures are standardized for age and sex to the Swiss population. NW, northwest; CH, Switzerland. Achermann R et al. Clin Microbiol Infect 2011; 17: 855–861

21
Antibiotikakonsum Schweiz, ambulanter Bereich
Alle Antibiotika Nur Chinolone Filippini, Health Pol 2006;78:77.

22
Assoziation Penicillinkonsum und Anteil non-suszeptibler Pneumokokken
CH Goossens, Lancet 2005;365:579.

23
Risk factors for carriage of penicillin-nonsusceptible pneumococci, children <5 years old
Day care (current) 1.44 0.002 Antibiotic exposure, last 8 weeks 1.49 1.13 – 1.96 0.003 Western Switzerland 1.62 1.29 – 2.03 <0.001 Mühlemann et al. J Infect Dis 2003
 Antibiotic exposure, last 8 weeks – Western Switzerland – < Mühlemann et al. J Infect Dis")
25
Borreliose Wie behandeln Sie einen Patienten mit gesicherter Neuroborreliose? a) mit einer Radiculitis b) mit einer Encephalitis?
 mit einer Radiculitis b) mit einer Encephalitis. .")
26
Bremell and Dotevall European Journal of Neurology 2014, 21: 1162–1167

27
Bremell and Dotevall European Journal of Neurology 2014, 21: 1162–1167

28
Bremell and Dotevall European Journal of Neurology 2014, 21: 1162–1167

29
Doxycyclin für Neuroborreliose des zentralen und peripheren Nervensystems
Retrospektiver Vergleich. Abfall der Zellzahl im Liquor als Erfolgsparameter Bremell and Dotevall European Journal of Neurology 2014, 21: 1162–1167

30
Studienpatienten mit Neuroborreliose
Ljostad et al. Lancet Neurol 2008;7:690

31
Behandlungsresultat Ljostad et al. Lancet Neurol 2008;7:690

34
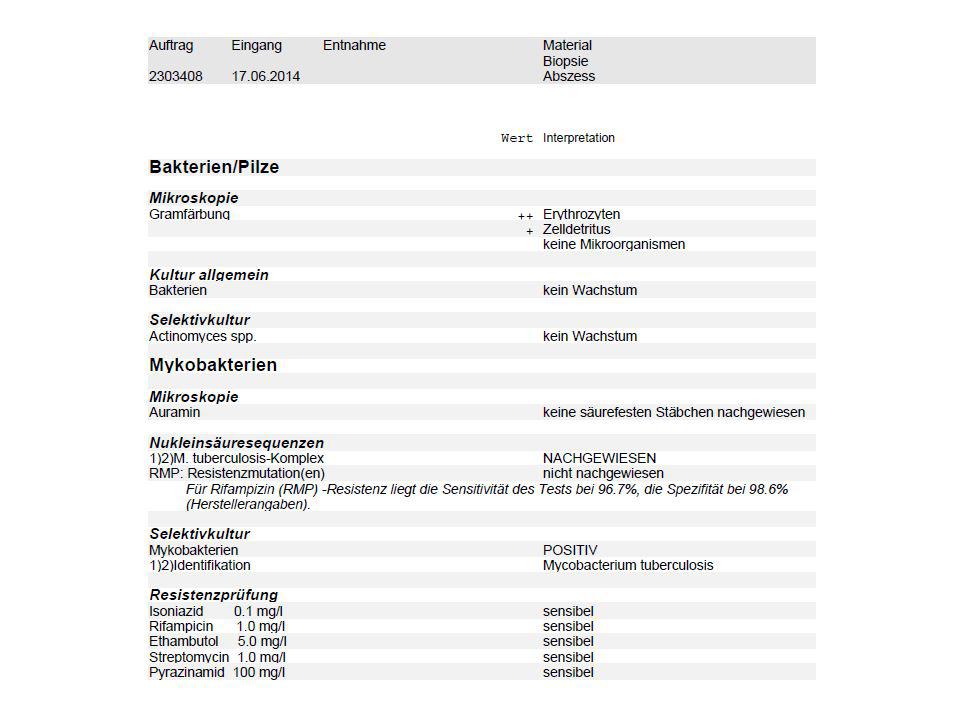
Diagnose der Tuberkulose
Kultur von Mycobacterium tuberculosis! Dauert 2-3 ( bis 8) Wochen bis Kulturen positiv werden Verdacht auf TB: Säurefeste Stäbchen im Sputum (oder in der Biopsie) Amplifikation (PCR) direkt aus dem Sputum kann den Nachweis von M: tuberculosis innert Stunden erbringen PCR Amplifikation der Genloci mit bekannten Resistenzmutationen kann innert Stunden Informationen über die Empfindlichkeit liefern
 Wochen bis Kulturen positiv werden. Verdacht auf TB: Säurefeste Stäbchen im Sputum (oder in der Biopsie) Amplifikation (PCR) direkt aus dem Sputum kann den Nachweis von M: tuberculosis innert Stunden erbringen. PCR Amplifikation der Genloci mit bekannten Resistenzmutationen kann innert Stunden Informationen über die Empfindlichkeit liefern.")
35
Xpert® MTB/RIF assay Lawn Future Microbiol 2011;6:1067
>95% der Rifampicin-resistenten M. tuberculosis Stämme haben eine Mutation in der 81-bp hot spot region des rpoB Gens Figure 1. The rpoB gene core region target sequence and molecular beacon technology (A) The rpoB gene, the nucleotide sequence of the core region and the localization of the complementary overlapping molecular beacon probes that span the complete core region. (B) The stem-and-loop structure of a molecular beacon and onset of fluorescence following binding to a complementary DNA strand. The loop structure of the molecular beacon contains the complementary oligonucleotide probe sequence, and the fluorophore and quencher molecules are attached to the ends of the stem structure. Following hybridization, conformational change in the probe leads to separation of the fluorophore and quencher molecules and onset of fluorescence. Lawn Future Microbiol 2011;6:1067 Lawn Future Microbiol 2011;6:1067
 The rpoB gene, the nucleotide sequence of the core region and the localization of the. complementary overlapping molecular beacon probes that span the complete core region. (B) The stem-and-loop structure of a molecular beacon and onset of fluorescence following. binding to a complementary DNA strand. The loop structure of the molecular beacon. contains the complementary oligonucleotide probe sequence, and the fluorophore and. quencher molecules are attached to the ends of the stem structure. Following hybridization, conformational change in the probe leads to separation of the fluorophore and quencher. molecules and onset of fluorescence. Lawn Future Microbiol 2011;6:1067. Lawn Future Microbiol 2011;6:1067.")
36
GeneXpert® MTB/RIF assay
Figure 2. Various steps within the Xpert® MTB/RIF assay procedure SR: Sample reagent. Diagram supplied by C Boehme, Foundation for Innovative New Diagnostics. Lawn Future Microbiol 2011;6:1067

37
Xpert® MTB/RIF assay Lawn Future Microbiol 2011;6:1067
SPC: sample processing control Figure 3. GeneXpert user view of the amplified probes A-E and the sample processing control Trace (A) shows the read-out from processing a rifampicin-sensitive strain of Mycobacterium tuberculosis as denoted by amplification of all five probes with a similar cycle threshold. Trace (B) shows the read-out of a rifampicin-resistant strain as shown by the failure of amplification of Probe B. SPC: Sample processing control. Lawn Future Microbiol 2011;6:1067
 shows the read-out from processing a rifampicin-sensitive strain of. Mycobacterium tuberculosis as denoted by amplification of all five probes with a similar. cycle threshold. Trace (B) shows the read-out of a rifampicin-resistant strain as shown by. the failure of amplification of Probe B. SPC: Sample processing control. Lawn Future Microbiol 2011;6:1067.")
38
Xpert® MTB/RIF assay Lawn Future Microbiol 2011;6:1067

39
Resistenz gegen antituberkulöse Medikamente 2005 - 2009
BAG Bulletin 10/2011

40
Schweiz: stabiler Anteil an resistenten M. tuberculosis Isolaten
30 MDR Fälle 6 Ex-USSR 5 Somalia und Äthiopien 4 Tibet BAG Bulletin 10/2011

41
Anteil multiresistenter TB
Neue Fälle Vorbehandelte Fälle Gandhi Lancet 2010;375:1930

42
Anteil der MDR-TB von neuen TB-Fällen - WHO 2011
Global Tuberculosis control - WHO Report 2012

43
MDR-TB Worldwide and in most countries with a high burden of MDR-TB, <25% of the people estimated to have MDR-TB were detected in GeneXpert® MTB/RIF, a rapid molecular diagnostic test, is being rapidly adopted by countries to detect TB and rifampicin-resistant TB.

44
WHO treatment recommendations for MDR-TB
Intensive phase of at least 8 months Total treatment duration of at least 20 months is recommended WHO Guidelines for the programmatic management of drug-resistant tuberculosis 2011 update

45
Second-line drugs to treat MDR-TB
WHO Guidelines for the programmatic management of drug-resistant tuberculosis 2011 update

46
Natural history of untreated TB
10-year case fatality 53% and 86%, with a weighted mean of 70%. 10-year case fatality approximately 20%. Tiemersma EW. Et al Plos one 2011;6:e17601

48
Was tun bei kulturellem Nachweis von Candida
Aus dem Urin (meist) Nichts Candida spp. werden oft im Urin gefunden, v.a bei Patienten mit Blasenkatheter und antibiotischer Therapie. Die meisten sind asymptomatisch. Meist ist dies kein Hinweis auf einen Harnwegsinfekt mit Candida Die Kolonienzahl im Urin hilft nicht bei der Unterscheidung Kolonisation vs. Infektion Die Diagnose eines Harnwegsinfekts beruht auf dem cystoskopischen Nachweis eines Pilzballs oder dem bioptischen Nachweis einer Gewebeinvasion
 Nichts. Candida spp. werden oft im Urin gefunden, v.a bei Patienten mit Blasenkatheter und antibiotischer Therapie. Die meisten sind asymptomatisch. Meist ist dies kein Hinweis auf einen Harnwegsinfekt mit Candida. Die Kolonienzahl im Urin hilft nicht bei der Unterscheidung Kolonisation vs. Infektion. Die Diagnose eines Harnwegsinfekts beruht auf dem cystoskopischen Nachweis eines Pilzballs oder dem bioptischen Nachweis einer Gewebeinvasion.")
49
Candida spp. im Urin Bei Patienten mit Diabetes mellitus, Blasensteinen oder Abflusshindernissen kann eine Candidurie persistieren oder es kann ein Pilzball auftreten. Ohne diese Risikofaktoren verschwinden iatrogene Candidurien meist spontan Candida spp. in Urinzylindern kann auf eine invasive Niereninfektion hinweisen Behandlung indiziert bei Patienten mit Nierentransplantation, Neutropenie, bevorstehenden Eingriffen an den Harnwegen

50
Inzidenz der Candidurie auf der IPS
Bougnoux M-E et al. Intensive Care Med 2008;34:292

51
Candidurie auf der Intensivpflegestation
Bei Erwachsenen fast immer Kolonisation oder Kontamination. Fast alle sind asymptomatisch. Nur sehr selten ist eine Pilztherapie indiziert Fig. 1 Kaplan–Meier estimates of the proportions of candiduria-free patients (b) as a function of time between their ICU admissions and infection onset. Proportions are shown bysolid lines,anddotted linesindicate 95% CI Bougnoux M-E et al. Intensive Care Med 2008;34:292
 as a function of time between their ICU admissions and infection onset. Proportions. are shown bysolid lines,anddotted linesindicate 95% CI. Bougnoux M-E et al. Intensive Care Med 2008;34:292.")
52
Charakteristika der Candidurischen Patienten
Bougnoux M-E et al. Intensive Care Med 2008;34:292

53
Candidurie und Candida HWI
In contrast to that which occurs in adults in the medical and surgical ICU settings, candiduria in the critically ill newborn very often reflects candidemia or disseminated candi-diasis and in addition may be accompanied by obstructing, urinary tract fungus ball formation. In a majority of episodes in adult patients in the critical care setting, candiduria represents colonization or contamination of the specimen cultured rather than infection and most patients are asymptomatic. Rarely is antifungal therapy required. Sobel J. et al. Clin Infect Dis 2011;52(Suppl 6):S433
:S433.")
54
IDSA Guidelines zum Management der Candidiasis
Pappas et al. CID 2009;48:503

55
Speziesverteilung bei Candida Isolaten aus Blutkulturen
Isolates n % C. albicans 675 61.9 C. glabrata 191 17.5 C. tropicalis 64 5.9 C. parapsilosis 59 5.4 C. dubliniensis 33 3 C. krusei 22 2 C. lusitaniae 12 1.1 C. kefyr 8 0.7 C. pelliculosa 6 0.6 C. guilliermondii 9 0.8 C. famata 4 0.4 C. norvegensis 0.3 C. inconspicua 0.2 C. rugosa Total 1090 C. Orasch et al. for the Funginos group, ECCMID 2010 55

56
Candidämien in der Schweiz
1.01 P=0.004 0.49 0.38 The incidence of candidemia significantly increased from 0.38 episodes/10’000 patient-days in 1991 (0.43/10’000 in university and 0.21/10’000 in non-university hospitals) to 0.49/10’000 in 2000, (0.57/10’000 and 0.35/10’000, respectively) and 1.01/10’000 in 2010, p=0.004 (1.37/10’000 and 0.79/10’000) (see figure) C. Orasch et al. for FUNGINOS; ECCMID 2013
 to 0.49/10’000 in 2000, (0.57/10’000 and 0.35/10’000, respectively) and 1.01/10’000 in 2010, p=0.004 (1.37/10’000 and 0.79/10’000) (see figure) C. Orasch et al. for FUNGINOS; ECCMID")
57
20-Year Evolution of Candida sp. (n = 2659)
8% 5% 2% 5% 15% n = 543 n = 594 n = 846 n = 676 64% C. albicans : 64% Uni 69% Uni-affiliated C. albicans : 60% Uni 66% Uni-affiliated Within the 20 years of the study, a total of 2659 Candida isolates were tested. Overall C. albicans was the most common species accounting for more than 60%, followed by C. glabrata accounting for about 15%, and C.tropicalis with 6%. The species distribution stayed similar in the different time periods from 1991 to 2010 Other species were C. dubliniensis C. lusitaniae C. kefyr C. pelliculosa C. guilliermondii C. famata C. norvegensis C. inconspicua C. rugosa Or unknown species – which was the reason why in more than 10% of Candida were in this section (show orange)
")
58
Candida Isolate aus Blutkulturen CH 2004 – 2009 (n = 1090)
% Anteil empfindlicher Isolate / Zahl resistenter Isolate O148 Six-year prospective candidemia survey from the fungal infection network of Switzerland (FUNGINOS) − Candida species distribution and antifungal susceptibility according to recent EUCAST and old vs. new CLSI clinical breakpoints C.E. Orasch*, O. Marchetti, C. Durussel, C. Guyaz, M. Ochsner, J. Bille and the Microbiological and Clinical FUNGINOS Investigators Objective: Changing Candida spp. distribution and emerging cross- resistance to azoles and multiresistance to azoles and echinocandins is increasingly reported in Europe and North America. To analyse the species distribution of Candida blood isolates prospectively collected during 2004−9 from 27 hospitals (7 university, 20 affiliated) of the FUNGINOS network and to compare the antifungal susceptibility according to the clinical breakpoints (bp) defined by EUCAST in Europe and CLSI in North America. Methods: Candida isolates were identified in the FUNGINOS mycology reference lab and tested for susceptiblity to fluconazole (F), voriconazole (V) and caspofungin (C) by microtitre broth dilution method with the Sensititre® YeastOne™ test panel. Clinical bp were: (i) EUCAST 2010/ CLSI 2008 = old for F and V, (ii) CLSI 2011 = new for F, V, C. Results: 1090 Candida blood isolates were tested: 675 (61.9%) C. albicans, 191 (17.5%) C. glabrata, 64 (5.9%) C. tropicalis, 59 (5.4%) C. parapsilosis, 33 (3%) C. dubliniensis, 22 (2%) C. krusei and 46 (4.2%) rare Candida spp. No change in Candida species distribution occurred during 2004−9. The table shows the percentages of susceptibility and numbers of non-susceptible isolates for each Candida species according to the different bp ( g/ml). Eight isolates (4 C. tropicalis,3 C. albicans,1 C. parapsilosis) showed a cross-resistance to azoles (F and V) according to EUCAST bp vs. 2 isolates (C. albicans) according to old and new CLSI bp. One C. tropicalis isolate was tested multi-resistant according to EUCAST bp (MIC F: 2 g/ml, V: 0.25 g/ml, C: 16 g/ml) vs. none according to old and new CLSI bp. Conclusions: In Switzerland the majority of Candida blood isolates were C. albicans (61.9%), followed by C. glabrata (17.5%). C. albicans was susceptible to all antifungals independently of the applied bp, whereas the proportion of fluconazole-susceptible C. tropicalis and C. parapsilosis was lower with the EUCAST and new CLSI vs. the old CLSI bp. Applying the EUCAST bp for voriconazole lowered the proportion of susceptible C. tropicalis and C. parapsilosis isolates vs. old and new CLSI bp. As expected, all Candida isolates were susceptible to caspofungin, except in C. krusei and C. parapsilosis. Only 4 isolates were cross-resistant to azoles and 1 C. tropicalis was multiresistant to azoles and caspofungin. The impact of recent EUCAST and CLSI breakpoints for predicting clinical response to therapy remains to be investigated. Orasch et al. ECCMID 2011;O148
 − Candida. species distribution and antifungal susceptibility according. to recent EUCAST and old vs. new CLSI clinical breakpoints. C.E. Orasch*, O. Marchetti, C. Durussel, C. Guyaz, M. Ochsner, J. Bille and the Microbiological and Clinical FUNGINOS Investigators. Objective: Changing Candida spp. distribution and emerging cross- resistance to azoles and multiresistance to azoles and echinocandins. is increasingly reported in Europe and North America. To analyse the. species distribution of Candida blood isolates prospectively collected. during 2004−9 from 27 hospitals (7 university, 20 affiliated) of the. FUNGINOS network and to compare the antifungal susceptibility. according to the clinical breakpoints (bp) defined by EUCAST in Europe. and CLSI in North America. Methods: Candida isolates were identified in the FUNGINOS mycology. reference lab and tested for susceptiblity to fluconazole (F), voriconazole. (V) and caspofungin (C) by microtitre broth dilution method with the. Sensititre® YeastOne™ test panel. Clinical bp were: (i) EUCAST 2010/ CLSI 2008 = old for F and V, (ii) CLSI 2011 = new for F, V, C. Results: 1090 Candida blood isolates were tested: 675 (61.9%) C. albicans, 191 (17.5%) C. glabrata, 64 (5.9%) C. tropicalis, 59 (5.4%) C. parapsilosis, 33 (3%) C. dubliniensis, 22 (2%) C. krusei and 46 (4.2%) rare Candida spp. No change in Candida species distribution occurred. during 2004−9. The table shows the percentages of susceptibility and. numbers of non-susceptible isolates for each Candida species according. to the different bp ( g/ml). Eight isolates (4 C. tropicalis,3 C. albicans,1 C. parapsilosis) showed. a cross-resistance to azoles (F and V) according to EUCAST bp vs. 2 isolates (C. albicans) according to old and new CLSI bp. One. C. tropicalis isolate was tested multi-resistant according to EUCAST. bp (MIC F: 2 g/ml, V: 0.25 g/ml, C: 16 g/ml) vs. none according to. old and new CLSI bp. Conclusions: In Switzerland the majority of Candida blood isolates were. C. albicans (61.9%), followed by C. glabrata (17.5%). C. albicans was. susceptible to all antifungals independently of the applied bp, whereas the. proportion of fluconazole-susceptible C. tropicalis and C. parapsilosis. was lower with the EUCAST and new CLSI vs. the old CLSI bp. Applying the EUCAST bp for voriconazole lowered the proportion. of susceptible C. tropicalis and C. parapsilosis isolates vs. old and. new CLSI bp. As expected, all Candida isolates were susceptible to. caspofungin, except in C. krusei and C. parapsilosis. Only 4 isolates were. cross-resistant to azoles and 1 C. tropicalis was multiresistant to azoles. and caspofungin. The impact of recent EUCAST and CLSI breakpoints. for predicting clinical response to therapy remains to be investigated. Orasch et al. ECCMID 2011;O148.")
59
Empirische Behandlung der Candidiasis
Flückiger U., Marchetti O. et al SMW 2006;136:447

60
Rezidivierende Harnwegsinfekte bei wiederholten Re-Infektionen mit identischem E.coli
Seit 1982 bekannt, aktuell zunehmende Häufigkeit mit Harnwegsinfekten alle 8 Wochen (Dysurie, Pollakisurie). Pyelonephritis vor 30 Jahren Symptome: Dysurie, Pollakisurie und allgemeinem Krankheitsgefühlohne Fieber. v.a. morgentlich übelriechenden, trüben Urin. Antibiotika: Nitrofurantoin, Ofloxacin, Fosfomycin, Augmentin und Ciprofloxacin. Bactrim: schwerer anaphylaktischer Schock, Nitrofurantoin: Exanthem, Ofloxacin: Malaise. Keine Pathologie der ableitenden Harnwege
. Pyelonephritis vor 30 Jahren Symptome: Dysurie, Pollakisurie und allgemeinem Krankheitsgefühlohne Fieber. v.a. morgentlich übelriechenden, trüben Urin. Antibiotika: Nitrofurantoin, Ofloxacin, Fosfomycin, Augmentin und Ciprofloxacin. Bactrim: schwerer anaphylaktischer Schock, Nitrofurantoin: Exanthem, Ofloxacin: Malaise. Keine Pathologie der ableitenden Harnwege")
61
Vor ca. 5 Wochen habe sie erneut einen Harnwegsinfekt aquiriert
Vor ca. 5 Wochen habe sie erneut einen Harnwegsinfekt aquiriert. Die Urinstix zeigten sich bland. Im Urikult wuchsen jedoch zwei verschiedene E. coli und ein Enterococcus sp. mit doch beträchtlichen Resistenzen v.a. auf per os zu gebende Antibiotika. Seitdem versucht die Patientin eine symptomatische Therapie mit Ibuprofen und Pracetamol. Bei zunehmendem Leidensdruck mit Dysurie und abdomienellen Schmerzen stellt sich die Patientin nun vor. Klinisch zeigte sich eine mässige Druckdolenz über der Blase, jedoch keine Nierenklopfschmerz. Fieber besteht nicht (36.2°C). Die Patientin wurde laut eigenen Angaben im Jahr 2014 gynäkologisch untersucht, die Kontrolle fiel unauffällig aus. Eine Oestrogentherapie im Rahmen der Menopause wird fortgeführt. Es besthet eine ausgeprägte Resistenzentwicklung des aktuellen E. coli Keims, der die Zystitis verursacht. Bei Allergie auf Nitrofurantoin und Bactrim aktuell nur i.v. Therapie mit Ertapenem möglich. Bitte um allergologische Abklärung und ggf. Desensibilisierung von Bactrim und/oder Nitrofurantoin. Besten Dank
. Die Patientin wurde laut eigenen Angaben im Jahr 2014 gynäkologisch untersucht, die Kontrolle fiel unauffällig aus. Eine Oestrogentherapie im Rahmen der Menopause wird fortgeführt. Es besthet eine ausgeprägte Resistenzentwicklung des aktuellen E. coli Keims, der die Zystitis verursacht. Bei Allergie auf Nitrofurantoin und Bactrim aktuell nur i.v. Therapie mit Ertapenem möglich. Bitte um allergologische Abklärung und ggf. Desensibilisierung von Bactrim und/oder Nitrofurantoin. Besten Dank")
63
Ben-Ami R. et al Clinical Infectious Diseases 2009; 49:682–90

64
Behandlungsalternativen
Fosfomycin – Monuril. p.o. für HWI mit breitem Erregerspektrum inkl. ESBL E . coli und Klebsiella. 1 x 3 g nüchtern, am besten abends nach Blasenentleerung; (3 Dosen alle 3 Tage bei komplizierten HWI) Neuner Antimicrob Agents and Chmother 2012;56:5744
 Neuner Antimicrob Agents and Chmother 2012;56:5744.")
65
Fosfomycin Behandlungserfolg gegen Erreger von HWI
Neuner Antimicrob Agents and Chmother 2012;56:5744

66
Schweizer Behandlungsempfehlungen, Unkomplizierte Zystitis
Hasse et al, in press Slide courtesy of Barbara Hasse, USZ

67
Schweizer Behandlungsempfehlungen, Pyelonephritis
Hasse et al, in press Slide courtesy of Barbara Hasse, USZ

68
Behandlungsalternativen
Nitrofurantoin – Furadantin 2 x 100 mg/Tag x 5 Tage mit dem Essen oder nach dem Essen. KI bei CrCl <50 für HWI mit Gram + Kokken (inkl. MRSA und Enterokokken), E. coli, Salmonellen Trimethoprim/Sulfamethoxazol - Bactrim160/800 2 x 1/Tag Ertapenem – Invanz 1 x 1 g/Tag i.v. über 30 min für 5 Tage
, E. coli, Salmonellen Trimethoprim/Sulfamethoxazol - Bactrim160/800 2 x 1/Tag Ertapenem – Invanz 1 x 1 g/Tag i.v. über 30 min für 5 Tage")
69
Behandlung: ganz, ganz kurz
ASB Zystitis Pyelonephritis Abszess Urosepsis Zunehmender Schweregrad Nil Nitro Fosfo Bactrim Cipro Bactrim Cipro Ceftriaxon Bactrim Ceftriaxon (oder IV Alternative) Cipro (& evtl Drainage) Ceftriaxon (o. IV Alternative) Cipro Erklären, dass es für ASB sowie unkompl HWI und Katheter-assoziierte HWI Guidelines gibt. Für andere nicht. Gupta et al, CID Hooton et al, CID 2010;50:625.
 Cipro. (& evtl Drainage) Ceftriaxon. (o. IV Alternative) Cipro. Erklären, dass es für ASB sowie unkompl HWI und Katheter-assoziierte HWI Guidelines gibt. Für andere nicht. Gupta et al, CID Hooton et al, CID 2010;50:625.")
Ähnliche Präsentationen