Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Dr. R. Herwig Urologische Klinik AKH Wien
Urologie Dr. R. Herwig Urologische Klinik AKH Wien

2
Wozu Urologie? 10% alle Patienten in einer allgemeinärztlichen Ordination haben urologische Erkrankungen Tumore im urologischen Bereich gehören zu den häufigsten Tumorerkrankungen Urologische Erkrankungen können frühe Warnhinweise auf Allgemeinerkrankungen geben

3
Womit beschäftigt sich Urologie
Niere (Steinerkrankungen) Ableitende Harnwege (Pyelon, Harnleiter, Blase, Prostata, Harnröhre) Penis Hoden Hormone Neurogene Steuerung der Miktion Tumore in diesem Bereich
 Ableitende Harnwege (Pyelon, Harnleiter, Blase, Prostata, Harnröhre) Penis. Hoden. Hormone. Neurogene Steuerung der Miktion. Tumore in diesem Bereich.")
4
Lernziele Urologie Anatomie / Physiologie
Häufige Pathologie der Organe Steinerkrankungen Prostataerkrankungen (BPH/Prostata-Ca) Tumore Andrologie
 Tumore. Andrologie.")
5
Steinerkrankungen

6
Steinerkrankungen Häufigkeit 4% aller Patienten
Vielschichtige prärenale, renale und postrenale Ursachen Zusätzliche Ursachen Erbliche Veranlagung Konstitution Streß Bewegungsarmut Ernährung Medikamente Klimatische, geografische, rassische Unterschiede Multifaktorielle Genese

7
Steinerkrankungen Epidemiologie
Inzidenz ca. 0,4% der über 18-jährigen Prävalenz 4% Männer und Frauen gleich häufig Harnsteinleiden im Kindesalter 2% Knaben im Verhältnis 3:2 häufiger Rezidivrisiko ohne medikamentöse Prophylaxe ca. 50%

8
Steinerkrankungen Formale Genese
Kristallines material mit etwa 2,5% organischer Grundsubstanz (Matrix) Auskristallisation bei Überschreitung des Löslichkeitsproduktes Kann durch andere Substanzen im Urin gefördert oder gehemmt (Inhibitoren) werden.
 Auskristallisation bei Überschreitung des Löslichkeitsproduktes. Kann durch andere Substanzen im Urin gefördert oder gehemmt (Inhibitoren) werden.")
9
Fixierte Harnsteinbildung
Interstitium der Nierenpapillen deutlich höhere Konzentrationen von Kalzium und Oxalsäure Nachweisbare Kalziumsalzniederschläge im Papillenbereich (Rendal-Plaque) Entstehung fixierter Kalziumoxalat / -phosphatsteine Zellnekrose und Abstoßung=> Kelchsteine
 Entstehung fixierter Kalziumoxalat / -phosphatsteine. Zellnekrose und Abstoßung=> Kelchsteine.")
10
Freie Harnsteinbildung
Harnübersättigung ist so ausgeprägt, dass die Kristallbildung sehr schnell abläuft Uratverstopfung Harnsäuresteine Zystinsteine Infektsteine Durch langes verbleiben im Harntrakt Kelchdivertikel Blasensteine bei Restharn

11
Steinarten Kalziumoxalat 70% Kalziumphosphat 10%
Magnesiumammoniumphosphat 5% Harnsäure % Zystin %

12
Pro / Contra Lithogene Substanzen Inhibitoren Kalzium Oxalsäure
Harnsäure Phosphat Zystin Inhibitoren Zitrat Magnesium

13
Zitrat Kalzium komplexieren
Zitrat ist eine Tricarboxy-Säure, wenn sie vollständig ionisiert bei einem pH 6.5 und 37°C vorliegt. Hat eine Wertigkeit von minus 3

14
Kalziumhaltige Steine
Allgemein Balaststoffreiche, gemischte Kost, Trinkmenge 2-3 l/Tag Negativ Positiv Kalziumhaltige Steine Oxalathaltige Steine Infektsteine Harnsäuresteine Zystinsteine Milch und Milchprodukte, kalziumreiche Mineralwässer Rhabarber, Spinat, Kakaoprodukte, schwarzer Tee Alkalisierende Mineralwässer Innereien, säuernde Mineralwässer, Alkohol Säuernde Mineralwässer Kalziumarme Minaralwässer Flüssigkeitszufuhr säuernde Minaralwässer Zitrussäfte, alkalisierende Mineralwässer Zitrussäfte, alkalisierende Mineralwässer

15
Ausscheidung: Kalzium
Renale Hyperkalzurie (renales Kalziumleck) Absorptive Hyperkalzurie (Kalziumzufuhr) Resorptive Hyperkalzurie (HPT) Idiopatische Hyperkalzurie (20%)
 Absorptive Hyperkalzurie (Kalziumzufuhr) Resorptive Hyperkalzurie (HPT) Idiopatische Hyperkalzurie (20%)")
16
Ausscheidung: Oxalsäure
90% aus endogenen Quellen (Glycin) 0,5 mmol Oxalsäure/Tag Ursachen Kurzdarmsyndrom, entzündliche Darmerkrankungen Primäre Hyperoxalurie
 0,5 mmol Oxalsäure/Tag. Ursachen. Kurzdarmsyndrom, entzündliche Darmerkrankungen. Primäre Hyperoxalurie.")
17
Ausscheidung: Harnsäure
Harnsäurekristalle als Kristallisationskern für Kalziumhaltige Steine Phosphate (am Steinaufbau beteiligt, HPT) Inhibitoren (saure Mucopolysaccaride, Magnesium, Zitrat) hemmende Wirkung
 Inhibitoren (saure Mucopolysaccaride, Magnesium, Zitrat) hemmende Wirkung.")
18
Phosphathaltige Steine
Stark bis schwach schattengebend pH-Verschiebung HPT, RTA Immobilisationsosteoporose Infektsteine Proteus, Providentia, Klebsielle, Pseudomonas, Serratia, Mycoplasmen Ausguß-, Korallensteine

19
Phosphathaltige Steine
Antibiotische Langzeitbehandlung Steinentfernung Mixtura solvens [NH4Cl] L-Methionin

20
Harnsäuresteine Nicht schattengebend (Schwacher Kalziummantel) Gicht
Maligne Erkrankungen Radio-, Chemotherapie Fasten

21
Harnsäuresteine Urinneutralisierung
Senkung der Harnsäurekonzentration (Allopurinol) Zitrussaft (stark basische Na/K-Salze einer schwachen Säure) Na-K-Zitratgemisch (Uralyt U)
 Zitrussaft (stark basische Na/K-Salze einer schwachen Säure) Na-K-Zitratgemisch (Uralyt U)")
22
Zystinsteine Angeborene rezessiv vererbte Erkrankung
Hohe Inzidenz im Kindesalter Lebenslange Therapie Schwach schattengebend (milchglasartig) Zystin, Ornithin, Lysin, Arginin (ZOLA)
 Zystin, Ornithin, Lysin, Arginin (ZOLA)")
23
Zystin The pH dependence of the solubility of cystine. (Modified from Dent CE, Senior B. Studies on the treatment of cystinuria. Br J Urol 1955;27:317, with permisison.)
")
24
Zystinsteine Vermehrte Flüssigkeitsaufnahme Urinalkalisierung
Vitamin C D-Penicillamin Α-Mercaptopropionylglycin (MPG)
")
25
Der urologische Situs A: Niere(n) B: Harnleiter C: Blase Nebenniere
LK-Stationen Prostata Blasensphinkter Penis Hoden/Skrotum

26
Mögliche Schmerzursachen im linken Unterbauch durch urologische Erkrankungen
Steinleiden Angeborene Erkrankungen Entzündliche Erkrankungen Tumorerkrankungen

27
Steinleiden Nierensteine Harnleitersteine Meist asymptomatisch
Ventil-/Nierenbeckensteine Harnleitersteine Je nach Lokalisation Schmerzen in der Flanke, im Mittel-, Unterbauch, in der Leiste, Hoden, Penisspitze oder Perineum

28
Diagnostik Anamnese Körperliche Untersuchung Urinanalyse
Mikrohämaturie Urin-pH Blutuntersuchung Kreatinin Leukozytose Thrombozytopenie Temperatur

29
Laboruntersuchungen Serum Urin pH Kalzium Urinstatus, -sediment
Urinkultur Kalzium Kreatinin Harnsäure

30
Steinleiden Diagnostik: Urinanalyse Ultraschall
Infekt? Mikrohämaturie? Ultraschall Hydronephrose Lokalisation RI Jet in die Blase Urogramm (symptomfrei/Kreatinin)
")
31
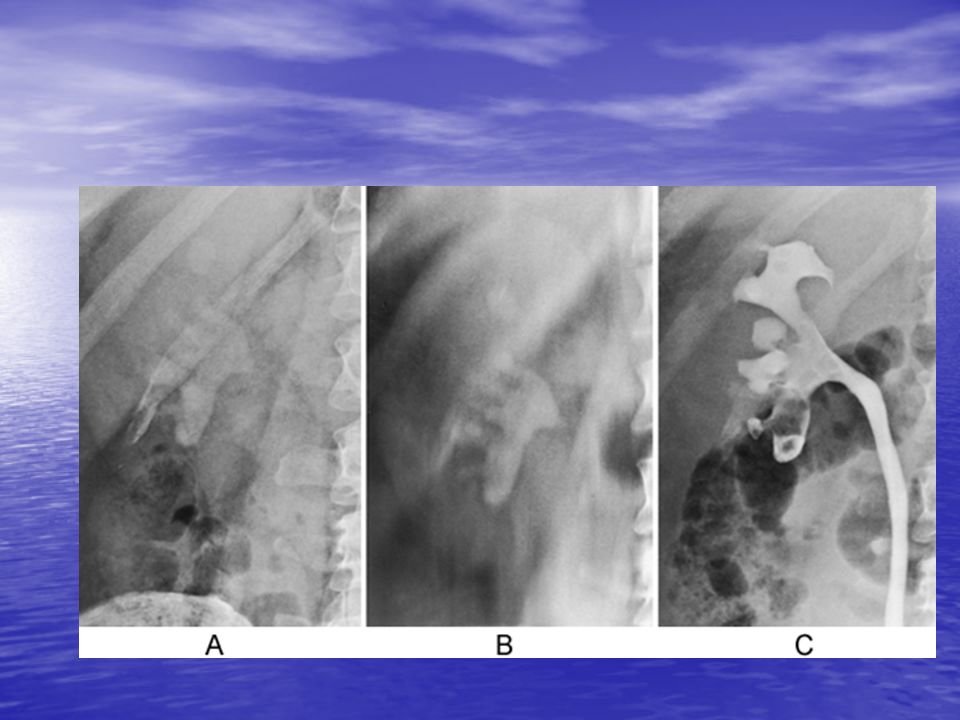
Therapie (nach Lokalisation und Steinart):
Erstbehandlung bei Koliken (Schmerztherapie) Splinteinlage (Überbrückung) ESWL Uretero-Renoskopie (URS) Percutane Nephro-Litholapraxie (PNL) Lysetherapie (z.B. Uralyt U)
 Splinteinlage (Überbrückung) ESWL. Uretero-Renoskopie (URS) Percutane Nephro-Litholapraxie (PNL) Lysetherapie (z.B. Uralyt U)")
32
ESWL

33
Hereditäre Erkrankungen
Nierenbeckenabgangsstenose Hufeisenniere mit Nephrolithiasis / PN Reflux / Megaureter Implantationsenge in die Blase

34
Steinerkrankungen Urinary SS alone does not explain the presence of stone disease in some individuals and its absence in others. Urine commonly is supersaturated for stone salts, especially calcium oxalate (110, 270). Small urinary crystals often are passed by individuals who have never formed a stone (271, 359). One explanation for this apparent paradox is the presence of crystallization inhibitors in urine (100)..
. Small urinary crystals often are passed by individuals who have never formed a stone (271, 359). One explanation for this apparent paradox is the presence of crystallization inhibitors in urine (100)..")
35
Inhibitors of crystal growth and aggregation have been isolated from human urine, and inhibitors of nucleation may exist (272, 280); inhibitors of crystal growth have received the most attention (101). Inhibitors usually are classified according to their ability to inhibit the growth of calcium phosphate or calcium oxalate. Pyrophosphate, citrate, and magnesium are known inhibitors of calcium phosphate crystal growth. Pyrophosphate and citrate also inhibit calcium oxalate crystal growth (299), but most of the calcium oxalate crystal growth inhibition in urine is provided by larger-molecular-weight polyanions: glycosaminoglycans and RNA fragments (21, 37, 197, 293). Heparin, although not found in urine, is a potent inhibitor of in vitro calcium oxalate crystal growth
, but most of the calcium oxalate crystal growth inhibition in urine is provided by larger-molecular-weight polyanions: glycosaminoglycans and RNA fragments (21, 37, 197, 293). Heparin, although not found in urine, is a potent inhibitor of in vitro calcium oxalate crystal growth.")
36
Acidic glycoproteins have been isolated from human urine and human kidney tissue culture medium (141, 212, 213). Evidence shows that patients with calcium oxalate nephrolithiasis have intrinsically abnormal acidic glycoproteins (210). These glycoproteins from healthy persons contain g-carboxyglutamic acid and are strong inhibitors of calcium oxalate crystal growth at low concentrations (10 to 7 M). Glycoprotein crystal growth inhibitor from patients does not contain g-carboxyglutamic acid and is a functionally poor inhibitor.
. These glycoproteins from healthy persons contain g-carboxyglutamic acid and are strong inhibitors of calcium oxalate crystal growth at low concentrations (10 to 7 M). Glycoprotein crystal growth inhibitor from patients does not contain g-carboxyglutamic acid and is a functionally poor inhibitor.")
37
Patients who form stones appear to excrete more lipids or acid phospholipids than normal individuals. Urinary excretion of glycolipid, cholesterol, and cholesterol esters also was higher in stone-formers (154). The greater excretion of lipids may reflect sloughing of tubular cells in response to a challenge by oxalate or calcium oxalate crystals. Acid phospholipids from cellular membranes may be involved with crystal nucleation and retention.
. The greater excretion of lipids may reflect sloughing of tubular cells in response to a challenge by oxalate or calcium oxalate crystals. Acid phospholipids from cellular membranes may be involved with crystal nucleation and retention.")
38
Citrate is filtered at the glomerulus and reabsorbed primarily in the proximal tubule (309). The ability of renal mitochondria to metabolize citrate by means of the tricarboxylic acid cycle is thought to control the renal clearance of citrate. Metabolic acidosis increases the entry of citrate into the matrix space of mitochondria and decreases the exit of citrate from mitochondria, thereby allowing mitochondrial oxidation of citrate. Cytoplasmic citrate levels decline, reabsorption of citrate from tubular fluid is enhanced, and less citrate appears in the final urine. Metabolic alkalosis has an opposite effect.

39
The luminal membrane of the proximal tubules (brush border membrane) is equipped with a Na+-gradient–dependent transport system that is highly specific for intermediates of the tricarboxylic acid cycle, including citrate (157). Metabolic acidosis caused by dietary acid loading increases the intrinsic capacity of proximal tubular brush border membrane to transport citrate from the tubular lumen into the cell interior (143). A corresponding decrease in urinary citrate excretion was seen. A dramatic increase in urinary citrate excretion was seen with dietary alkali loading (with NaHCO3), but brush border membrane transport of citrate was unchanged. These studies demonstrate that urinary citrate excretion is exquisitely sensitive to manipulation of systemic acid–base balance through effects on renal cellular function.
. A corresponding decrease in urinary citrate excretion was seen. A dramatic increase in urinary citrate excretion was seen with dietary alkali loading (with NaHCO3), but brush border membrane transport of citrate was unchanged. These studies demonstrate that urinary citrate excretion is exquisitely sensitive to manipulation of systemic acid–base balance through effects on renal cellular function..")
40
Urine from patients with recurrent calcium oxalate nephrolithiasis tends to have greater calcium oxalate SS and lower inhibitor levels than urine from healthy individuals (76, 271), but considerable overlap exists. It is impossible to predict consistently on the basis of SS or inhibition alone who will and who will not recurrently form calcium oxalate stones. A combination of these two factors, the saturation-inhibition index, has discriminated between healthy individuals and patients with recurrent stone formation (269). The saturation-inhibition index is a mathematic combination of relative calcium oxalate and inhibition of crystal growth and aggregation (as measured by the change in particle-size distribution in an in vitro crystal growth system). Patients with the greatest saturation-inhibition indexes had the highest recurrence rates. Because SS and inhibition are difficult to measure, this method has not had widespread clinical application.
. The saturation-inhibition index is a mathematic combination of relative calcium oxalate and inhibition of crystal growth and aggregation (as measured by the change in particle-size distribution in an in vitro crystal growth system). Patients with the greatest saturation-inhibition indexes had the highest recurrence rates. Because SS and inhibition are difficult to measure, this method has not had widespread clinical application..")
41
The concept of urinary risk factors is an extension of the saturation-inhibition index. This concept attempts to account for the multifactoral nature of calcium urolithiasis by considering six factors (236, 266, 267): urine volume, urine pH, urinary excretion of oxalate, uric acid, calcium, and alcian blue precipitable polyanions (a measure of acid mucopolysaccharides or large-molecular-weight inhibitors). Although no solitary abnormality may distinguish a stone-former, clear discrimination can be made by the presence of several risk factors. A low urine volume has the greatest risk, followed by a high urinary oxalate excretion. A high urine pH or uric acid excretion is associated with a higher probability of forming stones. Hypercalciuria is the least important risk factor.
: urine volume, urine pH, urinary excretion of oxalate, uric acid, calcium, and alcian blue precipitable polyanions (a measure of acid mucopolysaccharides or large-molecular-weight inhibitors). Although no solitary abnormality may distinguish a stone-former, clear discrimination can be made by the presence of several risk factors. A low urine volume has the greatest risk, followed by a high urinary oxalate excretion. A high urine pH or uric acid excretion is associated with a higher probability of forming stones. Hypercalciuria is the least important risk factor..")
42
Freshly voided urine samples from most healthy persons intermittently contain small crystals (usually calcium oxalate dihydrate), but only 5% to 10% of such persons will ever develop an actual kidney stone. These crystals probably form in the papillary collecting ducts and are flushed out with the urine before they grow large enough to become lodged in the lumen. Anatomic abnormalities or adherence to the epithelium may prevent these particles from leaving the kidney. This increased particle retention permits the crystals to grow larger, further reducing the likelihood that they will be passed spontaneously (35). This condition could easily predispose an individual to the formation of kidney stones. An attractive hypothesis is that patients with stone disease may have an increased particle retention time, possibly resulting from an abnormal tendency for small crystals to adhere to the epithelial lining of the upper urinary tract.
. This condition could easily predispose an individual to the formation of kidney stones. An attractive hypothesis is that patients with stone disease may have an increased particle retention time, possibly resulting from an abnormal tendency for small crystals to adhere to the epithelial lining of the upper urinary tract..")
43
Two theoretical mechanisms have been proposed for crystal retention: free particle or fixed particle. The free particle mechanism assumes that nucleation and initial crystal growth occur in the tubular lumen. The crystalline particles grow with such sufficient rapidity that they become trapped in the papillary collecting ducts, where they grow to form a macroscopic stone (350). Estimates of calcium oxalate crystal growth rates in the distal tubule have cast doubt on the ability of these crystals to grow rapidly enough to occlude the lumen before they are washed out of the collecting ducts (97). Some investigations have suggested that rapid aggregation of small crystals would permit free particle trapping to occur.
. Estimates of calcium oxalate crystal growth rates in the distal tubule have cast doubt on the ability of these crystals to grow rapidly enough to occlude the lumen before they are washed out of the collecting ducts (97). Some investigations have suggested that rapid aggregation of small crystals would permit free particle trapping to occur..")
46
In the United States and in other technologically developed countries, urolithiasis commonly occurs as upper tract stones. Bladder stones are more common in less-developed countries (7). Epidemiologic data suggest that climate, geography, and diet are important factors in the pathogenesis of urolithiasis (261). The best-known example of this influence is the apparent existence of ‘‘stone belts.” These are geographic areas that are associated with a high prevalence of stone formation (134). A questionnaire survey of hospitals estimated that, during 1952, 0.95 persons per 1,000 population were admitted to a hospital with a diagnosis of urinary calculi (26). A rate of 1.93 per 1,000 population in South Carolina and 0.43 per 1,000 in Missouri provided evidence of geographic variability. Each of the southeastern states had a high rate of urinary calculi. A more recent study found that 1.64 persons per 1,000 population were admitted to a hospital with the diagnosis of urolithiasis, an increase of 75% over the 22-year period (303). High rates were again found in the southeastern states, especially in the Carolinas (North Carolina, 3.0 per 1,000 population; South Carolina, 2.7 per 1,000 population), but the differences were not statistically significant.
. Epidemiologic data suggest that climate, geography, and diet are important factors in the pathogenesis of urolithiasis (261). The best-known example of this influence is the apparent existence of ‘‘stone belts. These are geographic areas that are associated with a high prevalence of stone formation (134). A questionnaire survey of hospitals estimated that, during 1952, 0.95 persons per 1,000 population were admitted to a hospital with a diagnosis of urinary calculi (26). A rate of 1.93 per 1,000 population in South Carolina and 0.43 per 1,000 in Missouri provided evidence of geographic variability. Each of the southeastern states had a high rate of urinary calculi. A more recent study found that 1.64 persons per 1,000 population were admitted to a hospital with the diagnosis of urolithiasis, an increase of 75% over the 22-year period (303). High rates were again found in the southeastern states, especially in the Carolinas (North Carolina, 3.0 per 1,000 population; South Carolina, 2.7 per 1,000 population), but the differences were not statistically significant..")
47
Normal pregnancy causes hypercalciuria, but pregnancy is not a stone-forming condition (57, 182). Abnormal crystalluria is not seen in pregnant patients, and more frequent stone production is not seen in stone-formers who become pregnant. A prospective study of 11 women revealed no change in urine volume (183). Although citrate excretion increased during pregnancy, this increase was not proportional to the increase in urinary calcium. Citrate failed to increase in parallel with calcium excretion, even though the urine pH rose. SS for calcium oxalate and brushite was as high in pregnancy as in patients with proven calcium nephrolithiasis. One explanation for the lack of clinical stone formation is the relatively short duration of pregnancy. Another explanation is an increase of protective mechanisms, such as crystal growth inhibition. Nephrocalcin excretion may increase during pregnancy.
. Although citrate excretion increased during pregnancy, this increase was not proportional to the increase in urinary calcium. Citrate failed to increase in parallel with calcium excretion, even though the urine pH rose. SS for calcium oxalate and brushite was as high in pregnancy as in patients with proven calcium nephrolithiasis. One explanation for the lack of clinical stone formation is the relatively short duration of pregnancy. Another explanation is an increase of protective mechanisms, such as crystal growth inhibition. Nephrocalcin excretion may increase during pregnancy..")
49
TABLE 8.2. CAUSES OF UROLITHIASIS
Renal tubular syndromes Renal tubular acidosis Cystinuria Hypercalcemic disorders Primary hyperparathyroidism Immobilization Milk-alkali syndrome Sarcoidosis Hypervitaminosis D Neoplastic diseases Cushing's syndrome Hyperthyroidism Uric acid lithiasis Idiopathic Gout Low urine output states Myeloproliferative diseases Enzyme disorders Primary hyperoxaluria Xanthinuria 2,8-Dihydroxyadeninuria Secondary urolithiasis Enteric hyperoxaluria Infection Obstruction Medullary sponge kidney Urinary diversion Drugs Idiopathic calcium urolithiasis Hypercalciuria Normocalciuria

50
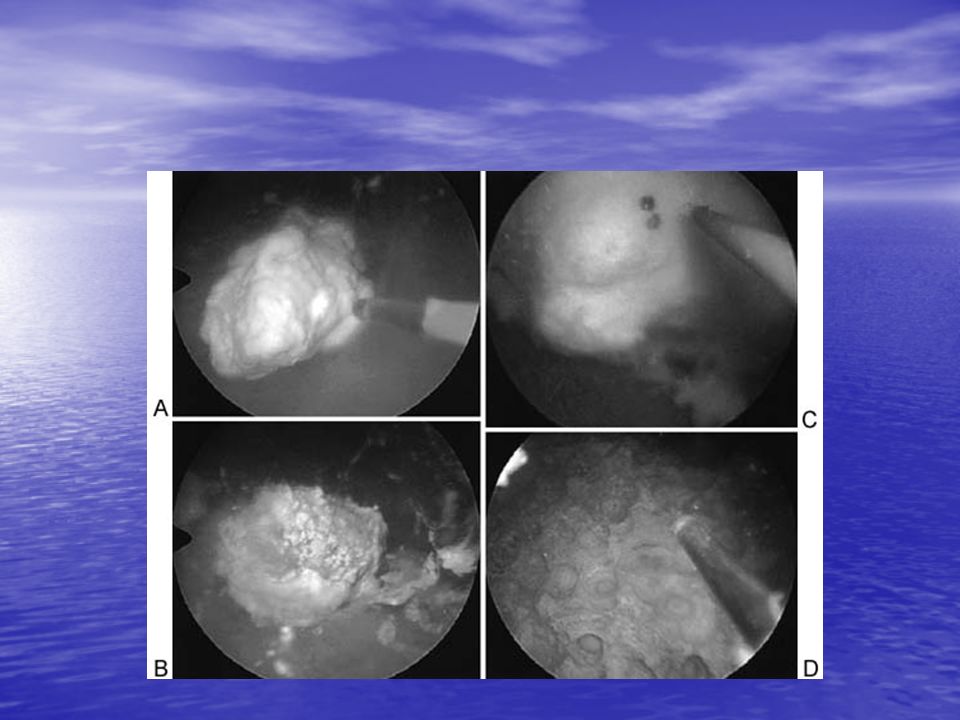
More support exists for the second theory, a fixed particle mechanism
More support exists for the second theory, a fixed particle mechanism. Rats with magnesium deficiency develop nephrocalcinosis and stone formation (219). Small stones were found attached to normal-appearing tubular epithelium near the bend of Henle's loop. This intranephronic calculosis may have occurred by crystal nucleation on the luminal membrane or attachment of a passing crystalline particle. Carr (38) suggested that crystals floating in the renal pelvis could be trapped in forniceal lymphatic vessels and grow to macroscopic size. Papillary tip stones could originate from crystals that had become attached to the epithelial lining of the distal collecting ducts and had grown out of the lumen to form a papillary cup (351). Randall's plaques (254) are macroscopic subepithelial deposits of calcium crystals. Although older studies found a poor correlation between the incidence of stone disease and the incidence of Randall's plaques, it was still hypothesized that the epithelium over the plaque could erode, and a calyceal stone could develop from crystal growth on the plaque (252). More recent studies of Randall's plaques have found that they are not just subepithelial deposits (326); they appear to extend deep into the papilla and are intimately associated with collecting tubules and vasa recta. These same investigators found that papillary plaques were more common in patients with calcium oxalate and calcium phosphate stones than in patients without a history of stone disease (180). Endoscopic examinations found that most patients with calcium stone disease had Randall's plaques.
. Small stones were found attached to normal-appearing tubular epithelium near the bend of Henle s loop. This intranephronic calculosis may have occurred by crystal nucleation on the luminal membrane or attachment of a passing crystalline particle. Carr (38) suggested that crystals floating in the renal pelvis could be trapped in forniceal lymphatic vessels and grow to macroscopic size. Papillary tip stones could originate from crystals that had become attached to the epithelial lining of the distal collecting ducts and had grown out of the lumen to form a papillary cup (351). Randall s plaques (254) are macroscopic subepithelial deposits of calcium crystals. Although older studies found a poor correlation between the incidence of stone disease and the incidence of Randall s plaques, it was still hypothesized that the epithelium over the plaque could erode, and a calyceal stone could develop from crystal growth on the plaque (252). More recent studies of Randall s plaques have found that they are not just subepithelial deposits (326); they appear to extend deep into the papilla and are intimately associated with collecting tubules and vasa recta. These same investigators found that papillary plaques were more common in patients with calcium oxalate and calcium phosphate stones than in patients without a history of stone disease (180). Endoscopic examinations found that most patients with calcium stone disease had Randall s plaques.")
51
The attachment of crystals to the kidney epithelium may involve a specific molecular interaction between stone crystals and the epithelial membrane. Rat renal inner-papillary collecting tubule cells have been isolated in primary cultures and used as a model for the study of crystal-membrane interactions (358). Riese and colleagues (258) developed a mathematic model of the binding of calcium oxalate crystals to these cells. This binding is location specific, saturable, and inhibitable. Calcium oxalate crystal binding appears to be related to cell membrane polarity (259). This binding is enhanced if a monolayer of cultured cells is depolarized by disrupting the normal intercellular tight junctions. These results suggest that the crystals preferentially attach to a basolateral cell membrane component. Renal epithelial cells also can endocytose calcium monohydrate crystals (175). Other studies continue to confirm the ability of calcium oxalate monohydrate crystals to specifically bind to cultured renal epithelial cells (22, 163, 176).
. Riese and colleagues (258) developed a mathematic model of the binding of calcium oxalate crystals to these cells. This binding is location specific, saturable, and inhibitable. Calcium oxalate crystal binding appears to be related to cell membrane polarity (259). This binding is enhanced if a monolayer of cultured cells is depolarized by disrupting the normal intercellular tight junctions. These results suggest that the crystals preferentially attach to a basolateral cell membrane component. Renal epithelial cells also can endocytose calcium monohydrate crystals (175). Other studies continue to confirm the ability of calcium oxalate monohydrate crystals to specifically bind to cultured renal epithelial cells (22, 163, 176)..")
52
The most provocative hypothesis regarding stone formation involves nanobacteria (147). Nanobacteria are sterile-filterable, Gram-negative, atypical bacteria that have been detected in bovine and human blood. They produce carbonate apatite on their cell walls and could potentially act as nidi for the precipitation of other stone salts, such as calcium oxalate. The smallest apatite units in kidney stones resemble the site and morphology of nanobacteria by scanning electron microscopy (48). One investigator has isolated nanobacteria from more than 90% of nonstruvite kidney stones.
. One investigator has isolated nanobacteria from more than 90% of nonstruvite kidney stones..")
53
Other investigators believe that the presence of matrix in urinary stones is serendipitous (99). Nonspecific physical adsorption of organic compounds on growing crystals may account for at least some of the matrix found in calculi (169). Electron microscopic examination of calcium oxalate crystals incubated with g-globulin or albumin has revealed an amorphous coat of material covering the crystals (146). This continuous coat is consistent with simple adsorption. Few studies have attempted to isolate and precisely identify the chemical composition of matrix. The best known investigations found similarities between urinary mucoproteins and matrix material that was extracted from renal stones with ethylenediaminetetra-acetic acid (EDTA). A mucoprotein material, matrix substance A, was identified in urine from patients with recurrent stone disease (27). This organic compound constituted approximately 85% of the total organic matrix of kidney stones. One-third of matrix substance A was carbohydrate and two-thirds was protein. Aspartic and glutamic acids were the most common amino acids found in the protein component. The carbohydrate component contained galactose, mannose, methylpentose, glucosamine, and galactosamine (24). Studies of dialyzed ultrafiltrates of matrix also found aspartic and glutamic acids. Alkaline hydrolysis revealed the presence of g-carboxyglutamic acid (174). Proteins containing this amino acid have a strong affinity for calcium ions. Urinary stone protein, or uropontin, is an aspartic acid–rich glycoprotein that is found in stone matrix (161). It binds calcium and has the same structure as osteopontin, which is found in bone and other mineralized tissue (36). Increased staining of distal renal tubular cells for this glycoprotein is seen in rats that have been induced to form stones by the administration of glyoxylic acid (160). Uropontin also has been isolated from urine and is a potent inhibitor of the nucleation, growth, and aggregation of calcium oxalate crystals and the binding of these crystals to renal epithelial cells (202). Uropontin concentration in urine appears to vary inversely with urine volume. Its ability to prevent calcium oxalate crystallization would increase as urinary concentration increases.
. A mucoprotein material, matrix substance A, was identified in urine from patients with recurrent stone disease (27). This organic compound constituted approximately 85% of the total organic matrix of kidney stones. One-third of matrix substance A was carbohydrate and two-thirds was protein. Aspartic and glutamic acids were the most common amino acids found in the protein component. The carbohydrate component contained galactose, mannose, methylpentose, glucosamine, and galactosamine (24). Studies of dialyzed ultrafiltrates of matrix also found aspartic and glutamic acids. Alkaline hydrolysis revealed the presence of g-carboxyglutamic acid (174). Proteins containing this amino acid have a strong affinity for calcium ions. Urinary stone protein, or uropontin, is an aspartic acid–rich glycoprotein that is found in stone matrix (161). It binds calcium and has the same structure as osteopontin, which is found in bone and other mineralized tissue (36). Increased staining of distal renal tubular cells for this glycoprotein is seen in rats that have been induced to form stones by the administration of glyoxylic acid (160). Uropontin also has been isolated from urine and is a potent inhibitor of the nucleation, growth, and aggregation of calcium oxalate crystals and the binding of these crystals to renal epithelial cells (202). Uropontin concentration in urine appears to vary inversely with urine volume. Its ability to prevent calcium oxalate crystallization would increase as urinary concentration increases.")
54
Steinerkrankungen Mit wenigen Ausnahmen (Auflösung von Harnsäure und Cystinsteinen), ist das Ziel der medizinischen Behandlung die Verhinderung der Neubildung oder Wachstum alter Steine. Diese Prophylaxe sollte effektiv und kontinuierlich erfolgen. Die Patienten sollten verstehen, das die Verhinderung der Steinneubildung eventuell eine lebenslange Behandlung beinhaltet.
, ist das Ziel der medizinischen Behandlung die Verhinderung der Neubildung oder Wachstum alter Steine. Diese Prophylaxe sollte effektiv und kontinuierlich erfolgen. Die Patienten sollten verstehen, das die Verhinderung der Steinneubildung eventuell eine lebenslange Behandlung beinhaltet.")
55
Steinerkrankungen Die Behandlung der Urolithiasis ist auf zwei Prinzipien aufgebaut: Eine Reduktion der Steinmasse (Elimination), und Eine Steigerung der inhibitorischen Aktivität Das letztere kann erreicht werden durch Seigerung der Quantität der Inhibitoren, der inhibitorischen Potenz oder in der Verringerung der Promotoraktivität.

56
Steinerkrankungen The purpose of a high fluid intake is to lower urinary SS. The dilution reduces ionic strength, complexation, and the concentration of inhibitors, but these side effects are more than offset by the reduction of SS. It is impossible for <stone> formation to occur in urine that is undersaturated for the particular <stone> salt. All patients with renal calculi should be counseled to increase their fluid intake.

57
An 8-ounce glass of fluid should be consumed hourly while awake, and 8 to 16 ounces of fluid should be consumed if the patient is up at night. Approximately half of the fluid should be water. The patient should produce at least 2,500 mL of urine per 24 hours. The fluid intake should be consistent.

59
A liberal intake of fluids during the day but poor intake during the night does not uniformly lower SS, especially after a heavy evening meal. Patients can use a container of known volume to inexpensively monitor their 24-hour urine output. A fixed numeric goal is helpful because most patients are poor estimators of their fluid intake and urine output.

Ähnliche Präsentationen







 Natural Sources SNAP11.>")










 Trackball. Joystick.>")

