Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Klaus F. Rabe MD, PhD Christian Albrecht University Kiel & LungenClinic Grosshansdorf (MEMBERS OF THE GERMAN CENTER FOR LUNG RESEARCH)
")
2
WAS IST COPD ?

3
Hansel TT, Lancet 2009

4
Anteil der Patienten mit COPD die nie selber geraucht haben....
25-30% The Lancet 347:733-43; 2009

5
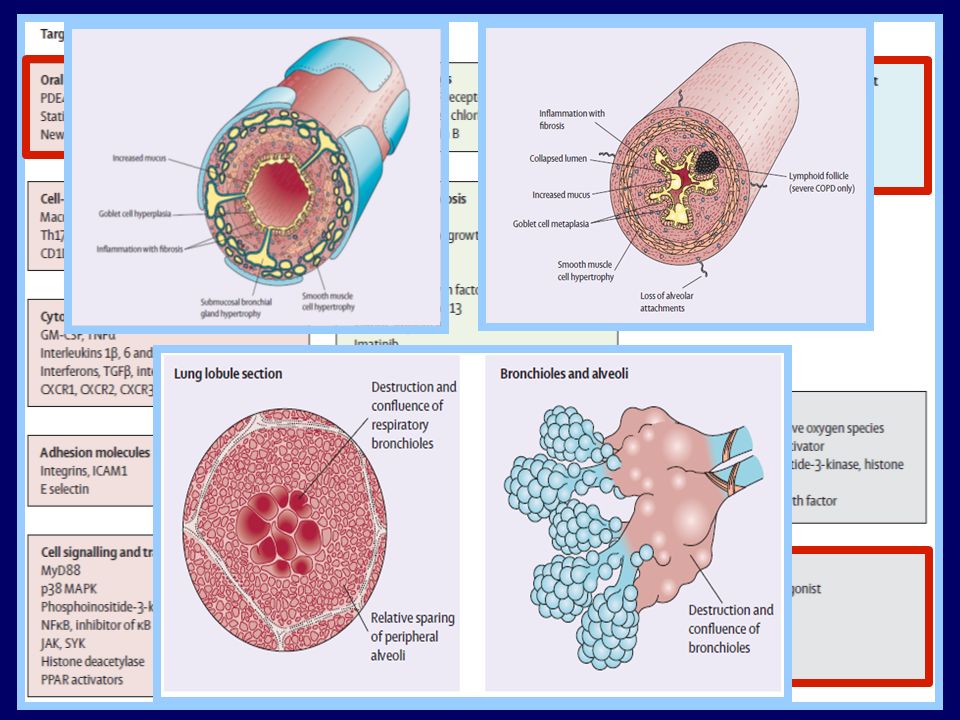
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Bronchitis Bronchiolitis Hansel TT, Lancet 2009

6
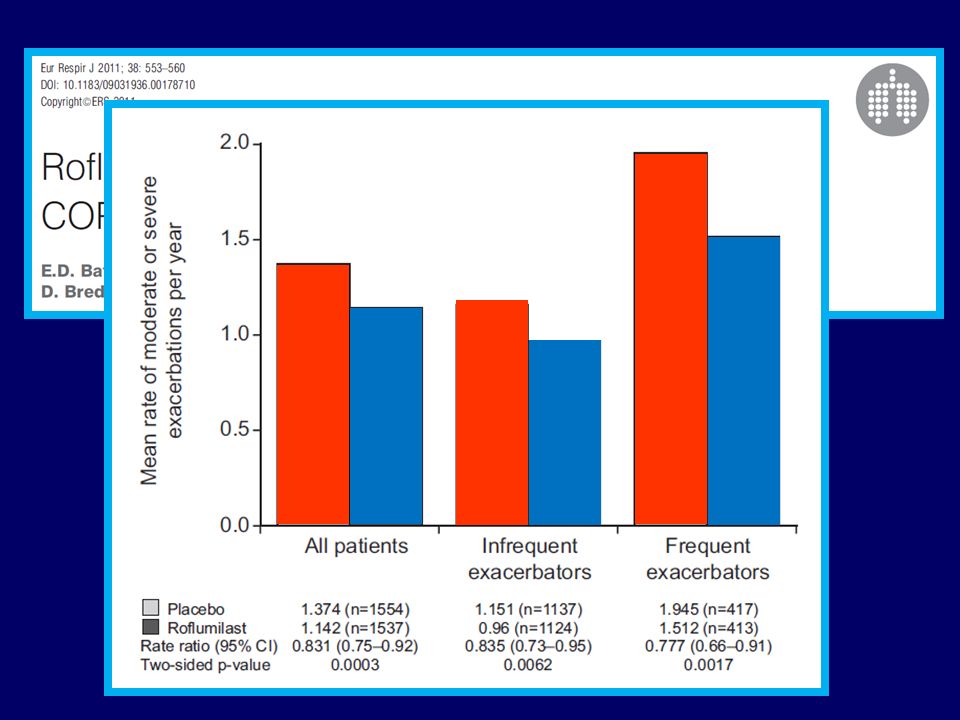
Martinez FJ, Calverley PMA, Goehring UM, et al. COPD7 2010;
EFFECT OF ROFLUMILAST ON EXACERBATIONS IN PATIENTS WITH CHRONIC COUGH AND SPUTUM Speaker notes A post-hoc analysis of pooled data from the two early phase III clinical studies was performed to identify subgroups of patients who received the most benefit from roflumilast treatment. Among the variables analysed, the presence of chronic bronchitis (symptoms of chronic cough and sputum) was found to correlate with a greater reduction in exacerbation rate compared with the absence of these symptoms. Overall, patients with chronic bronchitis experienced a 26.2% reduction in exacerbations compared with 1.1% reduction in patients with emphysema only and no chronic bronchitis. Reference Martinez FJ, Calverley PMA, Goehring UM, et al. Defining patient populations in COPD: Experience with roflumilast. COPD7 2010; poster 12. Available at: Martinez FJ, Calverley PMA, Goehring UM, et al. COPD7 2010;
 was found to correlate with a greater reduction in exacerbation rate compared with the absence of these symptoms. Overall, patients with chronic bronchitis experienced a 26.2% reduction in exacerbations compared with 1.1% reduction in patients with emphysema only and no chronic bronchitis. Reference. Martinez FJ, Calverley PMA, Goehring UM, et al. Defining patient populations in COPD: Experience with roflumilast. COPD7 2010; poster 12. Available at: Martinez FJ, Calverley PMA, Goehring UM, et al. COPD7 2010;")
7
WAS IST EINE SCHWERE COPD ?

8
Richens JL et al., Resp Res 2009;10:29-46
Activity of COPD... Richens JL et al., Resp Res 2009;10:29-46

9
Johnston AK et al., Thorax 2008;63:599-605
Wohin geht die COPD Forschung: Neue Ansätze für zukünftige Therapien...? 0.3 0.2 0.1 GOLD 3 or 4 Restricted GOLD 2 Risk of cardiovascular event GOLD 0 GOLD 1 Normal 2 4 6 8 10 12 14 Years of follow-up Johnston AK et al., Thorax 2008;63:

10
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? A slowly progessive cardiovascular disease which is masked through pulmonary effects...? Rutten and Hoes. Eur J Heart Fail 2012: 14:348-50

11
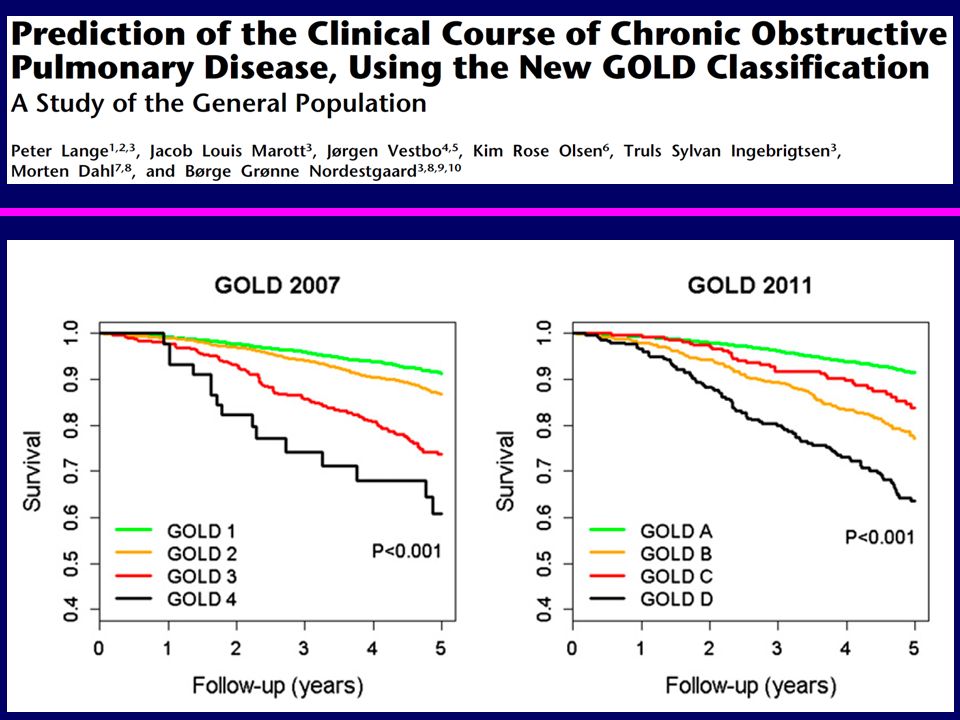
(C) (D) (B) (A) Risk Risk Symptoms
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD 4 (C) (D) > 2 3 (Exacerbation history) Risk (GOLD Classification of Airflow Limitation) Risk 2 (A) (B) 1 1 mMRC 0-1 CAT < 10 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score))
 (D) > (Exacerbation history) Risk. (GOLD Classification of Airflow Limitation) Risk. 2. (A) (B) mMRC 0-1. CAT < 10. mMRC > 2. CAT > 10. Symptoms. (mMRC or CAT score))")
16
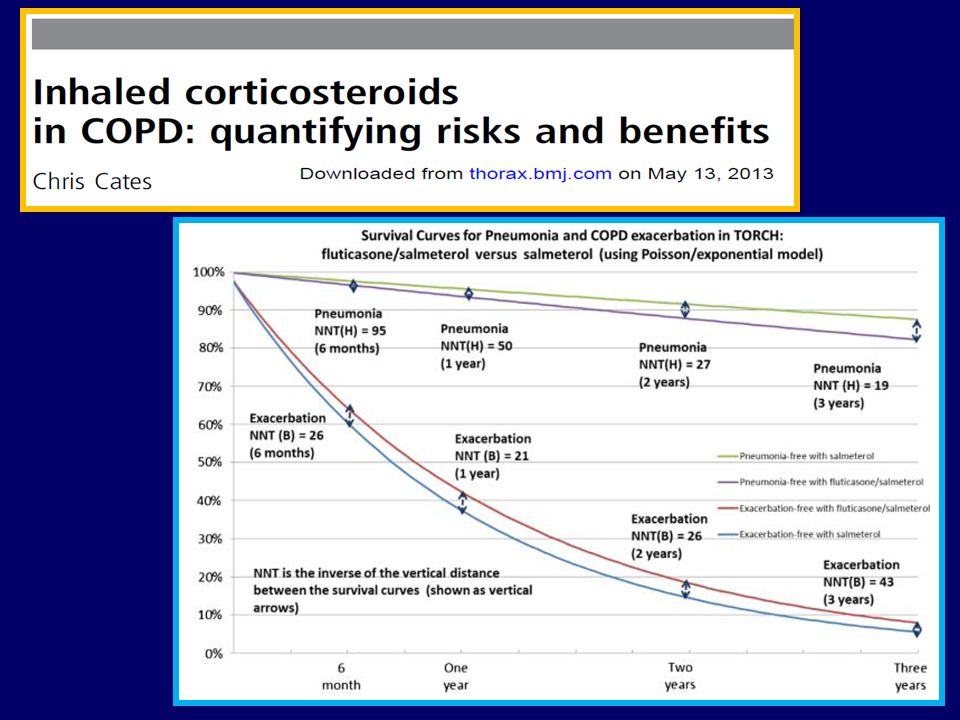
BRAUCHEN WIR INHALIERBARE
CORTICOSTEROIDE IN DER COPD?

17
Hogg, J. C. et al. N Engl J Med 2004;350:2645-2653
Figure 2. Pathological Findings in Patients with COPD. Panel A shows a collection of bronchial lymphoid tissue with a lymphoid follicle containing a germinal center (GC) surrounded by a rim of darker-staining lymphocytes that extend to the epithelium of both the small airway and alveolar surface (Movat's stain, x6). Panel B shows another follicle, in which the germinal center stains strongly for B cells (x6), and Panel C shows a serial section of the same airway stained for CD4 cells, which are scattered around the edge of the follicle and in the airway wall (x6.5). Panel D shows an airway that has been extensively remodeled by connective-tissue deposition in the subepithelial and adventitial compartments of the airway wall. The arrow points to the smooth muscle that separates the subepithelial from the adventitial compartments (Movat's stain, x6). Hogg, J. C. et al. N Engl J Med 2004;350:
 surrounded by a rim of darker-staining lymphocytes that extend to the epithelium of both the small airway and alveolar surface (Movat s stain, x6). Panel B shows another follicle, in which the germinal center stains strongly for B cells (x6), and Panel C shows a serial section of the same airway stained for CD4 cells, which are scattered around the edge of the follicle and in the airway wall (x6.5). Panel D shows an airway that has been extensively remodeled by connective-tissue deposition in the subepithelial and adventitial compartments of the airway wall. The arrow points to the smooth muscle that separates the subepithelial from the adventitial compartments (Movat s stain, x6). Hogg, J. C. et al. N Engl J Med 2004;350:")
18
TORCH: All-cause Mortality at 3 Years
HR 0.825, p=0.052 17.5% risk reduction Probability of death (%) 18 16 Placebo 15.2% 14 SFC % 12 10 2.6% absolute reduction 8 6 4 The survival status of 6111/6112 patients was established. One subject in the SFC arm with survival status unknown at 3 years was treated as censored at 2 years (113 weeks) (the last time point at which survival status was known). The difference in all-cause mortality between SFC and placebo was analysed by the log-rank test (stratified by smoking status) and presented as a Kaplan-Meier plot and calculated hazard ratios. The log-rank test is a popular method for comparing the survival of groups that takes into account the whole follow-up period. It was used to test the null hypothesis that there was no difference between treatment groups in the probability of an event (death) at any time point. The unadjusted hazard ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.820, p= This p value must be compared to a significance level of p=0.04 because of the interim analyses. The adjusted Hazard Ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.825, indicating a 17.5% reduction in the risk of death from any cause (p=0.052). The absolute risk reduction with SFC was 2.6% compared with placebo. Although the difference between SFC and placebo was on the edge of the pre-specified p-value of 0.05, it is debatable whether this modest reduction in confidence about the significance of the mortality data invalidates the conclusions. The number of deaths in this 4-limb trial was substantial (875 in the ITT population in total, 193 on SFC and 231 on placebo), although still less than anticipated (the study was powered assuming 440 deaths for SFC and placebo in total, whereas we actually had 424). We powered the study assuming a 17% placebo mortality rate over 3 years whereas our placebo rate was only 15.2%). This, together with the impact of the interim analyses, may explain the observed significance level for the primary outcome. Reference Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): 2 12 24 36 48 60 72 84 96 108 120 132 144 156 Time to death (weeks) Number alive 1524 1533 1464 1487 1399 1426 1293 1339 Calverley et al NEJM 2007
 Placebo 15.2% 14. SFC 12.6% % absolute reduction The survival status of 6111/6112 patients was established. One subject in the SFC arm with survival status unknown at 3 years was treated as censored at 2 years (113 weeks) (the last time point at which survival status was known). The difference in all-cause mortality between SFC and placebo was analysed by the log-rank test (stratified by smoking status) and presented as a Kaplan-Meier plot and calculated hazard ratios. The log-rank test is a popular method for comparing the survival of groups that takes into account the whole follow-up period. It was used to test the null hypothesis that there was no difference between treatment groups in the probability of an event (death) at any time point. The unadjusted hazard ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.820, p= This p value must be compared to a significance level of p=0.04 because of the interim analyses. The adjusted Hazard Ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.825, indicating a 17.5% reduction in the risk of death from any cause (p=0.052). The absolute risk reduction with SFC was 2.6% compared with placebo. Although the difference between SFC and placebo was on the edge of the pre-specified p-value of 0.05, it is debatable whether this modest reduction in confidence about the significance of the mortality data invalidates the conclusions. The number of deaths in this 4-limb trial was substantial (875 in the ITT population in total, 193 on SFC and 231 on placebo), although still less than anticipated (the study was powered assuming 440 deaths for SFC and placebo in total, whereas we actually had 424). We powered the study assuming a 17% placebo mortality rate over 3 years whereas our placebo rate was only 15.2%). This, together with the impact of the interim analyses, may explain the observed significance level for the primary outcome. Reference. Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): Time to death (weeks) Number. alive Calverley et al NEJM")
19
RATE OF MODERATE AND SEVERE EXACERBATIONS
Mean number of exacerbations/year 25% reduction 1.2 1.13 0.97* 1 0.93* 0.85*†‡ 0.8 0.6 0.4 Moderate exacerbations are defined as those which require treatment with systemic corticosteroids and/or antibiotics; severe exacerbations are defined as those which require hospitalisation. The exacerbation rate was calculated as the total number of moderate and/or severe exacerbations experienced by a patient during the treatment period. The number of exacerbations was analysed using a generalised linear model, assuming the Negative Binomial distribution, with time on treatment as an offset variable. The model included adjustments for the effects of smoking status, age, gender, baseline FEV1, number of exacerbations reported in the 12 months prior to screening, and region.1 SFC significantly lowered the rate of moderate/severe exacerbations compared with placebo (25% reduction, p < 0.001), SALM (12% reduction, p = 0.002) and FP (9% reduction, p = 0.024). SALM and FP also had significantly lower exacerbation rates than placebo (15%, p < and 18%, p < 0.001, respectively).1 SFC reduced the rate of moderate-to-severe exacerbations to a much greater extent than placebo or either of the component monotherapies.1 Exacerbations and hospitalisations predict the risk of dying from COPD over 5 years.2 Reference Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): & Online Supplement Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. 0.2 Placebo SALM FP SFC Treatment Calverley et al. NEJM 2007 *p < vs placebo; †p = vs SALM; ‡p = vs FP
, SALM (12% reduction, p = 0.002) and FP (9% reduction, p = 0.024). SALM and FP also had significantly lower exacerbation rates than placebo (15%, p < and 18%, p < 0.001, respectively).1. SFC reduced the rate of moderate-to-severe exacerbations to a much greater extent than placebo or either of the component monotherapies.1. Exacerbations and hospitalisations predict the risk of dying from COPD over 5 years.2. Reference. Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): & Online Supplement. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925– Placebo. SALM. FP. SFC. Treatment. Calverley et al. NEJM *p < vs placebo; †p = vs SALM; ‡p = vs FP.")
20
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Price D, et al. Prim Care Respir J. 2013; 22: Drummond MD, et al. JAMA. 2008;300: Lapi F, et al. Eur Respir J. doi: / Williamson PA, et al. Eur Respir J. Eur Respir J. 2011; 37:

23
Lancet RM 2013 Interpretation: -Addition of fluticasone furoate to vilanterol was associated with a decreased rate of moderate and severe exacerbations of COPD in patients with a history of exacerbation, but was also associated with an increased pneumonia risk.

24
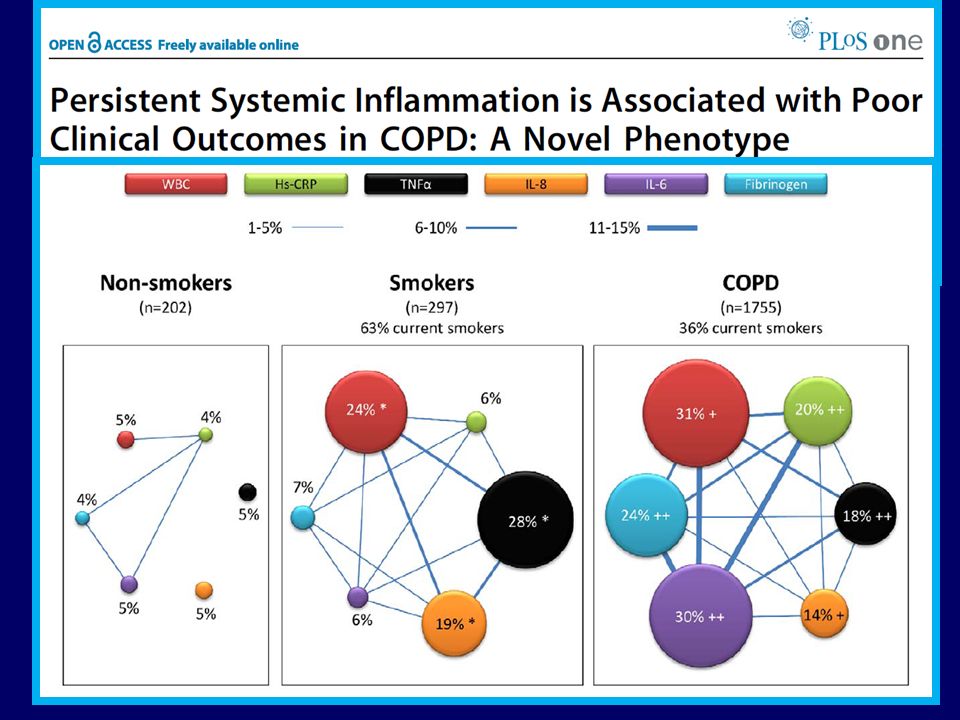
PHÄNOTYPEN DER COPD

25
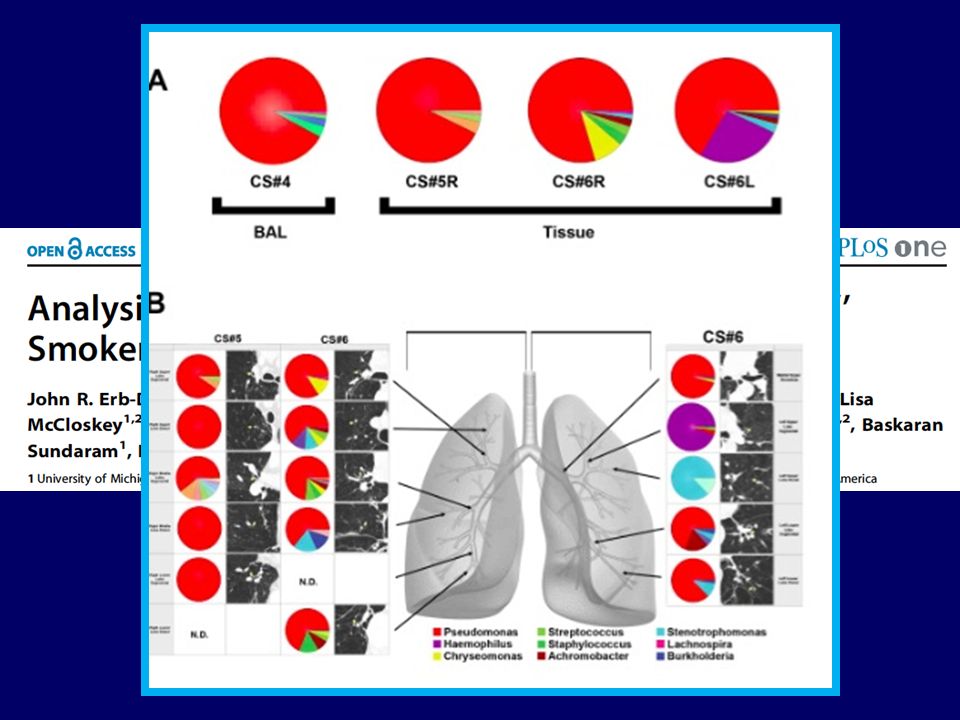
COPD PHÄNOTYPEN Chronische Bronchitis Emphysem Reversibilität...
Exacerbation frequency phenotypes Lower airway bacterial colonisation Fast Decliners in FEV1 Early symptoms Co-Morbiditäten Alpha-1 Antitrypsin Mangel– genetische Phänotypen Bronchiektasen...

28
DAUERTHERAPIE MIT ANTIBIOTIKA ?

31
MACROLIDE (AZITHROMYCIN) STUDY
PROPORTION OF PARTICIPANTS FREE OF ACUTE EXACERBATIONS OF COPD Figure 2. Proportion of Participants Free from Acute Exacerbations of Chronic Obstructive Pulmonary Disease (COPD) for 1 Year, According to Study Group. The analyses were based on the participants who were randomly assigned to the group minus those who did not return for any follow-up assessment — 558 participants in the azithromycin group, of whom 317 (57%) had an acute exacerbation, and 559 in the placebo group, of whom 380 (68%) had an acute exacerbation. Albert RK et al. N Engl J Med 2011;365:
 for 1 Year, According to Study Group. The analyses were based on the participants who were randomly assigned to the group minus those who did not return for any follow-up assessment — 558 participants in the azithromycin group, of whom 317 (57%) had an acute exacerbation, and 559 in the placebo group, of whom 380 (68%) had an acute exacerbation. Albert RK et al. N Engl J Med 2011;365:")
32
COMORBIDITÄTEN DER COPD

33
Young RP et al., Eur Respir J 2007;30:616-622
Wohin geht die COPD Forschung: Neue Ansätze für zukünftige Therapien...? CV mortality Overall mortality 2 4 6 8 10 20 30 40 50 60 70 80 heavy smoker moderate smoker ex- smoker non-smoker current smoker ex-smoker never smoker Odds ratio Mortality rate % <65 >100 <50 >100 FEV1 % pred FEV1 height adjusted Young RP et al., Eur Respir J 2007;30:

37
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? The New Drugs for COPD… Statins… ACE inhibitors ? Beta-blockers ? + “COPD drugs”

38
Van Gestel YRBM et al., Am J Cardiol 2008;102:192-196
Statin Therapy and Mortality: Peripheral Arterial Disease With Associated COPD 50 75 100 25 No COPD / Statins No COPD / no Statins Survival (%) COPD / Statins COPD / no Statins 2 4 6 8 10 Number at risk No COPD Mild COPD Moderate COPD Severe COPD Follow-up (years) 1545 476 961 327 1223 348 667 208 1018 224 505 107 824 154 345 60 610 106 229 39 433 55 145 18 Van Gestel YRBM et al., Am J Cardiol 2008;102:
 COPD / Statins. COPD / no Statins Number at risk. No COPD. Mild COPD. Moderate COPD. Severe COPD. Follow-up (years) Van Gestel YRBM et al., Am J Cardiol 2008;102:")
40
Roflumilast 500 mcg, od, p.o. + Roflumilast 250 mcg, od p.o.
Wohin geht die COPD Forschung: Neue Ansätze für zukünftige Therapien...? 3/31/2017 9:51 AM 0.04 Roflumilast 500 mcg, od, p.o. + Roflumilast 250 mcg, od p.o. placebo, od, p.o. 0.03 Probability of event 0.02 0.01 0.00 30 60 90 120 150 180 210 240 270 300 330 360 390 Days post-randomisation White WB, et al. Chest 2013 *MACE : CV death, non-fatal MI, non-fatal stroke SAFETY (BU)
")
41
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Troosters T, et al. Respir Med. 2010; 104(7): 1005–1011.
: 1005–1011.")
42
Prediction of Mortality in COPD: Measurements Beyond Lung Function
Waschki et al Chest 2011

43
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Atherogenic Dyslipidemia Triglycerides HDL cholesterol Cholesterol/HDL cholesterol ratio "Normal" LDL cholesterol but apo B Small, dense LDL and HDL Postprandial hyperlipidemia Inflammation Insulin Resistance Insulin resistance Hyperinsulinemia Hyperglycemia Type 2 diabetes New Markers of CHD Risk: What to Look for, What to Target? The metabolic syndrome has been defined by the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) as a cluster of atherothrombotic, inflammatory abnormalities that increase the risk of type 2 diabetes and cardiovascular disease. It is most frequently found in patients with abdominal obesity and insulin resistance. However, this definition that describes a constellation of risk factors has been confused with the 5 clinical criteria proposed by NCEP ATP III that identify individuals who are likely to be characterized by these clustering atherothrombotic, inflammatory abnormalities. Reference: Adapted from Després JP, Pascot A, Lemieux I, et al. Obesity management: a priority in the primary and secondary prevention of cardiovascular disease. In: Medeiros-Neto G, Halpern A, Bouchard C, eds. Progress in Obesity Research: 9. France: John Libbey Eurotext; 2003:29-35. Thin fibrous cap Lipid Core Thrombotic State PAI-1 Fibrinogen Coronary Atherosclerosis Unstable Plaque Inflammatory State Leptin CRP Cytokines Risk of Acute Coronary Syndrome Abdominal Obesity Metabolic Risk Factors Adapted from Després JP, et al. Progress in Obesity Research: 9; 2003:29-35.
 as a cluster of atherothrombotic, inflammatory abnormalities that increase the risk of type 2 diabetes and cardiovascular disease. It is most frequently found in patients with abdominal obesity and insulin resistance. However, this definition that describes a constellation of risk factors has been confused with the 5 clinical criteria proposed by NCEP ATP III that identify individuals who are likely to be characterized by these clustering atherothrombotic, inflammatory abnormalities. Reference: Adapted from Després JP, Pascot A, Lemieux I, et al. Obesity management: a priority in the primary and secondary prevention of cardiovascular disease. In: Medeiros-Neto G, Halpern A, Bouchard C, eds. Progress in Obesity Research: 9. France: John Libbey Eurotext; 2003: Thin fibrous cap. Lipid Core. Thrombotic State. PAI-1. Fibrinogen. Coronary Atherosclerosis Unstable Plaque. Inflammatory State. Leptin. CRP. Cytokines. Risk of Acute Coronary Syndrome. Abdominal Obesity. Metabolic Risk Factors. Adapted from Després JP, et al. Progress in Obesity Research: 9; 2003:")
44
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Wouters et al, Endocrinology 2012

45
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Wouters et al, Endocrinology 2012

46
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Kelly. Science 2012 Based on data from Boström et al. Nature 2012

47
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? n= , follow up = 7 yrs Wen et al. Lancet 2011; 378:

48
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Ouchi et al, Nat Rev Immunol 2011 48

49
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? 49

50
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Transcriptional (PPARɣ) Co-activator Irisin Handschin and Spiegelman. Nature 2008
 Co-activator. Irisin. Handschin and Spiegelman. Nature")
51
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...?

52
Wohin geht die COPD Forschung:
Neue Ansätze für zukünftige Therapien...? Klaus F. Rabe MD, PhD Christian Albrecht University Kiel & LungenClinic Grosshansdorf (MEMBERS OF THE GERMAN CENTER FOR LUNG RESEARCH)
")
Ähnliche Präsentationen









 in Germany elective subject for medical students during.>")


 At RHIC: T ch = 160 ± 10 MeV B = 25 ± 5 MeV 2) S = 1. The hadronic system is thermalized.>")





 bei Herzinsuffizienz>")


