Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Etiology of Cannabis-Related Disorders Hans-Ulrich Wittchen* Institute of Clinical Psychology and Psychotherapy Technische Universität Dresden Max-Planck-Institute of Psychiatry * Speaker BMBF-Addiction Research Network ASAT Das Forschungsvorhaben „Vulnerabilitäts- und Protektionsfaktoren bei Frühstadien von Substanzmissbrauch und Abhängigkeit“ (EDSP und ANEPSA-Verbunddaten) sowie das Anschlussvorhaben wurden gefördert vom Bundesministerium für Bildung und Forschung (BMBF) Förderkennzeichen: BMBF 01 EB 9405/6 und 01 EB 9901/6 als Teilpojekte des BMBF Suchtforschungsverbunds ASAT gefördert.
 sowie das Anschlussvorhaben wurden gefördert vom Bundesministerium für Bildung und Forschung (BMBF) Förderkennzeichen: BMBF 01 EB 9405/6 und 01 EB 9901/6 als Teilpojekte des BMBF Suchtforschungsverbunds ASAT gefördert.")
2
Why are we interested in the etiology of CUD? Prevalence and incidence Cannabis use can result in dependence syndromes (Nocon et al JPR 2002) Increased neuropsychological and psychopathological risks (Henquet et al 2004, Perkonigg et al 2006, Wittchen et al 2006) Negative effects on development and social functioning (von Niekerk et al 2002) Increased risk for other drug use disorders („gateway drug“ von Niekerk et al 2002) To understand and describe its development in order to: predict onset of problematic and use disorders, to prevent effectively use and transitions to CUD and to design appropriate strategies for early interventions and effective therapy and rehabilitation
 Increased neuropsychological and psychopathological risks (Henquet et al 2004, Perkonigg et al 2006, Wittchen et al 2006) Negative effects on development and social functioning (von Niekerk et al 2002) Increased risk for other drug use disorders („gateway drug von Niekerk et al 2002) To understand and describe its development in order to: predict onset of problematic and use disorders, to prevent effectively use and transitions to CUD and to design appropriate strategies for early interventions and effective therapy and rehabilitation.")
3
Critical issues There is a wide spectrum of „cannabis-related disorders“ (CUD) The heterogeneity of CUDs implies heterogenous „etiologies“ (even for dependence) Even restricting CUD to „dependence“ it is unlikely to find…… One single etiological model simple (causal) etiological pathways It is more likely to find highly complex vulnerability – stress/risk models
 The heterogeneity of CUDs implies heterogenous „etiologies (even for dependence) Even restricting CUD to „dependence it is unlikely to find…… One single etiological model simple (causal) etiological pathways It is more likely to find highly complex vulnerability – stress/risk models")
4
Problem resolved! Vulnerability factors + Increased incidence of cannabis- related disorders = time Exposition with drug increasing availability Easier access permissiveness Life style Potency of drug Acute effects Chronic effects Distal & proximal risk- factors … partially!

5
Why only a partial resolution? Sampling and design of etiological studies Diffusion of constructs and variables Lack of integration of research findings Lack of appropriate vulnerability and risks modeling Lack on research on mediators and moderators Lack of clinically useful predictive models

6
Problem 1: Etiological research results are dependent on sampling frames Community/general population or fractions thereof Drug Use Experience (lifetime user) Current Users Problematic Drug Users* SUD ( Substance Abuse/ and Dependence) Persons in contact with services For treatment and intervention *Problem drug use: i.e social or physical harm
 Current Users Problematic Drug Users* SUD ( Substance Abuse/ and Dependence) Persons in contact with services For treatment and intervention *Problem drug use: i.e social or physical harm")
7
Problem 2 - An incomplete summary of factors Sociodemographic factors: - Adoescent age - male - Low socio-economic status - Urbanicity Developmental: - birth complications - neglect - Divorce/separation/death - bonding - traumatic, critical life events - Genetic/family genetic: - genes - Anxiety and depressive disorders - bipolar disorders - substance use disorders - other (somatoform, personality dis, etc) Familiar factors: - Rejection - emotional warmth and overprotection - family styple and attitudes - substance use Intrapersonel factors: - behavioral inhibition - conduct disorders - antisocial Personlyity dis. - self-esteem, confidence - regulation of cognition and affect - impulsivity - daily hazzles Interpersonel factors: - peer group - social network and support - interpersonel life events– and conditions Mental disorders - conduct and dissocial disorders - ADHD - anxiety disorders - mood diosrders - nicotine dependence Substance-related factors - access and availability - type and frequency of consumption - potency

8
Cannabis-related disorders: Developmental course and influencing factors progression into higher use categories, abuse, dependence, Polysubstance use fluctuating use persistent use factors influencing onset factors influencing course first usecourse remission/cessation Early vulnerability-/risk-factors age extent risk Later/proximal factors Variables and factors that themselves are not associated (do not produce) negative outcomes Variables and factors that are significantly associated with the outcome
 negative outcomes Variables and factors that are significantly associated with the outcome")
9
Vulnerability factors + Increased incidence of cannabis- related disorders = time Exposition with drug increasing availability Easier access permissiveness Life style Potency of drug Acute effects Chronic effects Distal & proximal risk- factors Problem 3: Broadening our models Moderators and mediators No use first use Experimental use Regular use abuse Dependent use

10
A mediator (B) explains how and why another variable (A) affects the outcome (O) (Variable A influences B directly) A O B A moderator (A) specifies on whom/under what condition another variables (B) will operate to produce the outcome (O) (Variable A affect the relationship between B and O) ABO high familiar genetic liability Experimental use of cannabis/access Regular/problematic use or SUD ABO Early childhood trauma/neglect low self-esteem to refuse cannabis offer Cannabis use disorder A O B Mediators and moderators (Kraemer et al., 2001)
 explains how and why another variable (A) affects the outcome (O) (Variable A influences B directly) A O B A moderator (A) specifies on whom/under what condition another variables (B) will operate to produce the outcome (O) (Variable A affect the relationship between B and O) ABO high familiar genetic liability Experimental use of cannabis/access Regular/problematic use or SUD ABO Early childhood trauma/neglect low self-esteem to refuse cannabis offer Cannabis use disorder A O B Mediators and moderators (Kraemer et al., 2001)")
11
Cannabis-related disorders: Developmental course and influencing factors progression into higher use categories, abuse, dependence, Polysubstance use fluctuating use persistent use factors influencing onset factors influencing course first usecourse remission/cessation Early vulnerability-/risk-factors Gender, genetic factors Family genetic factors Temperament, personality Early mental disorders Early life events Socialisation Availability/drug use setting age examples for moderating risk factors extent risk Later/proximal factors Qunatity/frequency, concommittant use Mental disorders Family factors Self consciousness, self efficacy Life events, Peer group Availability/drug setting Dissocial behavior Wittchen 2002

12
Unresolved questions Why do (young) people engage in experimental cannabis use, and some not, in spite of similar exposition? Why some people change to regular use or stop? Why some progress to cannabis abuse or dependence SUDs? Why some maintain regular use or even stop after long periods of use? What makes people to develop and change specific patterns of substance use? How do family-genetic factors, neurobiological, psychopathology, social- psychological factors influence transitions (change process)? Research need: mechanisms of change ( mediators) Research need: mechanisms of action of intervening factors (moderators) Bühringer et al in press IJMPR
. Research need: mechanisms of change ( mediators) Research need: mechanisms of action of intervening factors (moderators) Bühringer et al in press IJMPR.")
13
Temporal structure and vulnerability and risk factors: Core lessons and a few examples The high risk period for onset of use and disorders is limited to the time period 15-25 The risk factors and vulnerability-risk interactions for firsts onset of use, regular use and CUD vary by outcome and over time

14
N = 3021; EDSP, T0 – T3 Incidence of Substance Use up to age 34 (EDSP, N=3021) Standardized cumulative incidence Wittchen et al in press DAD
 Standardized cumulative incidence Wittchen et al in press DAD")
15
N = 3021; EDSP, T0 – T3 Incidence patterns of Cannabis Use and Disorders up to age 34 Standardized cumulative incidence Wittchen et al in press DAD

16
Example for modeling Incidence of CUD by parental disorders 11,1% OR: 2,0* 10,5% OR: 1,9* 6,2% Strongly increased risk if parents are affected Wittchen et al in press DAD

17
What predicts progression to problematic and dependent cannabis use? (proportional odds model) Zimmermann et al 2004 DAD
 Zimmermann et al 2004 DAD.")
18
Onset regular use of cannabis Baseline predictors age > 21 female Easy access/availability Peers use-pressures Low self control (high impulsivity) Behavioral Inhibition (internalizing dis) Externalizing problems High self-esteem Family climate Parental disorders Life events/adverse events High daily hassles Regular use of nicotine Zimmermann et al 2004 DAD
 Behavioral Inhibition (internalizing dis) Externalizing problems High self-esteem Family climate Parental disorders Life events/adverse events High daily hassles Regular use of nicotine Zimmermann et al 2004 DAD")
19
Onset cannabis use disorders Predictors for CUD age > 21 female High frequency of use Easy access/availability Peers use-pressures Low self control (high impulsivity) Behavioral Inhibition (internalizing dis) Externalizing problems High self-esteem Family climate Parental disorders Life events/adverse events High daily hassles Other substance use/disorders Regular use of nicotine Zimmermann et al 2004 DAD
 Behavioral Inhibition (internalizing dis) Externalizing problems High self-esteem Family climate Parental disorders Life events/adverse events High daily hassles Other substance use/disorders Regular use of nicotine Zimmermann et al 2004 DAD")
20
Many human dimensions increase the risk for onset and progression CU/CUD: Family genetic factors and climate (Lieb et al., 2003) Conduct and other externalizing syndromes (Fergusson et al 2002; Costello 2003) Various anxiety and depressive (internalizing) disorders (Behrendt et al 2006) Adverse events and childhood trauma (Wittchen & Jacobi, 2005) More proximal factors: access and availability, social network, peers and support, self-esteem, coping skills (von Niekerk et al., 2002) Substance-related factors (access, quantity-frequency, potency) (Zimmermann et al 2004) Complex gene x environment interactions and neurobiological linkages of psychological and psychopathological factors But their relative contribution varies over time (Wittchen & Costello 2007): initiation strongly influenced by proximal (accidental) factors, transition to CUD more strongly by the persons existing vulnerabilities Vulnerability and risk factors for onset and course
 Conduct and other externalizing syndromes (Fergusson et al 2002; Costello 2003) Various anxiety and depressive (internalizing) disorders (Behrendt et al 2006) Adverse events and childhood trauma (Wittchen & Jacobi, 2005) More proximal factors: access and availability, social network, peers and support, self-esteem, coping skills (von Niekerk et al., 2002) Substance-related factors (access, quantity-frequency, potency) (Zimmermann et al 2004) Complex gene x environment interactions and neurobiological linkages of psychological and psychopathological factors But their relative contribution varies over time (Wittchen & Costello 2007): initiation strongly influenced by proximal (accidental) factors, transition to CUD more strongly by the persons existing vulnerabilities Vulnerability and risk factors for onset and course")
21
Stopping cannabis use: Probability of stable stopping up to age 34 (prospective analyses 10 years, N = 2466) Wittchen et al al in press % among baseline users with no 12-month use 10 years later Note! The vast majority stopped without formal help from the substance services Adolescent baseline status

22
Why do some people stop substance use without formal support, others not? Why do some people relapse after treatment, others not? Why do some people never change, even after intensive formal interventions? Why do we find in many studies major behaviour changes before the onset of formal treatment? Need to search for mechanisms of change (mediators) How do internal (e. g. neurobiological variations, psychological dispositions) or external factors (e. g. social-psychological context, therapeutic climate) interact with natural or treatment based changes in SUDs? Need to search for mechanisms of action of intervening factors (moderators) Cessation: Unresolved questions
 How do internal (e. g. neurobiological variations, psychological dispositions) or external factors (e. g. social-psychological context, therapeutic climate) interact with natural or treatment based changes in SUDs. Need to search for mechanisms of action of intervening factors (moderators) Cessation: Unresolved questions.")
23
People develop CUD, reduce or stop SUDs in a highly complex (individual) pattern We know a lot about the acute and chronic effects of cannabis on neurobiological systems, emotions, motivation, cognitions and behaviour, And we know a lot about the wide variety of factors involved in the onset and the progression to CUD But we are not yet able to integrate the findings to derive coherent and powerful interventions We know that formal broad preventive and therapeutic interventions and “natural” context conditions may affect cessation/reduction: But - We don’t know how the interaction of formal treatment and social context variables affect treatment outcome We need to better understand mechanisms of change in order to better shape preventive and therapeutic interventions as well as social conditions which support these changes Conclusions
 pattern We know a lot about the acute and chronic effects of cannabis on neurobiological systems, emotions, motivation, cognitions and behaviour, And we know a lot about the wide variety of factors involved in the onset and the progression to CUD But we are not yet able to integrate the findings to derive coherent and powerful interventions We know that formal broad preventive and therapeutic interventions and natural context conditions may affect cessation/reduction: But - We don’t know how the interaction of formal treatment and social context variables affect treatment outcome We need to better understand mechanisms of change in order to better shape preventive and therapeutic interventions as well as social conditions which support these changes Conclusions")
24
How to proceed with research? A change in the research agenda is needed! (Willenbring; NIAAA MOBC Research Initiative, 2006) To examine mechanisms of change is a necessary condition of progress in the field To broaden the view on mediators and moderators of change beyond formal interventions: The social context of “natural” behaviour change and of formal interventions To integrate our knowledge about vulnerability and risk interactions with neglected knowledge from other scientific fields like cognitive, affective and social neurobiology and neuropsychology, animal model research, social psychology and systems theory To utilise a broader range of research tools beyond RCT´s Similar need for reorientation in research on onset and course!
 To examine mechanisms of change is a necessary condition of progress in the field To broaden the view on mediators and moderators of change beyond formal interventions: The social context of natural behaviour change and of formal interventions To integrate our knowledge about vulnerability and risk interactions with neglected knowledge from other scientific fields like cognitive, affective and social neurobiology and neuropsychology, animal model research, social psychology and systems theory To utilise a broader range of research tools beyond RCT´s Similar need for reorientation in research on onset and course!.")
26
Cannabiskonsum, -missbrauch und -abhängigkeit: Stabilität über die Zeit (prospektive Analysen, N = 2466) Sydow et al., 2001 Baseline Status Final outcome (T2) status (%):
 Sydow et al., 2001 Baseline Status Final outcome (T2) status (%):")
27
Fazit – 5 Jahre später erhebliche Inzidenzsteigerung für Cannabis- und Stimulantien- /Halluzinogengebrauch (um 45-83%) vor allem bei Jüngeren! Hohe Konsum- und Störungsstabilität - spontaner Ausstieg ist selten, wann immer wiederholter und regelmäßiger Gebrauch starke Zunahme regelmäßig schwergradiger und abhängiger User Dies erscheint unvereinbar mit der Hypothese von Substanzkonsum als „vorübergehender Sozialisationskrise“! Gravierender Anstieg für „polysubstance“ Gebrauch und -störungen Erhebliche Verringerung des Geschlechtsunterschieds Spontanverlauf Frauen schlechter (Spontanverlauf, Abhängigkeitsstabilität!) Rauchen und Cannabis “gateway drugs” für Einstieg, Ecstasy für Progression zu Kokain und Halluzinogenen
 Rauchen und Cannabis gateway drugs für Einstieg, Ecstasy für Progression zu Kokain und Halluzinogenen.")
28
Illegale Drogen - Der Verlauf über 5 Jahre: Wie häufig sind spontane Remissionen? Mehr als 2/3 aller mit baseline (T0) Missbrauch oder Abhängigkeit sind weiterhin regelmäßige Konsumenten oder erfüllen Missbrauchs- oder Abhängigkeitskriterien zu T2
 Missbrauch oder Abhängigkeit sind weiterhin regelmäßige Konsumenten oder erfüllen Missbrauchs- oder Abhängigkeitskriterien zu T2.")
29
No drug use First try repeated use regular use /mild regular use /heavy prob. harmful use prob. dependence p high p low poly-substance use discontinuation p high p low Diagnostic sta- tus probability Discontinuation & polysubstance use probability Risk factors for continued use, drug problems & diagnosis Protective factors for discontinuation and no use family genetic age, gender schooling social class urbanicity self esteem coping, life skills behavioral inhib. licit drug use drug peers, availability integration early use use other drugs control/expect. no fam. genetic burden low develop. risks no childhood disorder good life skills low availability low BI good social integr. stable personality late 1st exposure high self-esteem high control t Conceptual framework for transitions in EDSP

30
Ablehnung Emotionale Wärme Overprotection OR 1 1.3* 1.4* Beginn von Störungen aufgr. von Cannabis (T1+T2) Beginn regelmäßiger Cannabiskonsum (T1+T2) Beginn Konsum illegaler Subst. (außer Cann.; T1+T2) Beginn Störungen aufgr. illeg. Subst. (außer Cann.; T1+T2) Erziehungsstil der Eltern (FEE; T0) und der Beginn des Konsums bzw. von Störungen aufgrund von illegalen Substanzen während des Follow-Ups (T1+T2) 1 Standardisierte ORs bei quantitativen Unabhängigen Variablen: OR entspricht Risikosteigerung bei Erhöhung des Wertes der UV um 1. erhoben zu T0: Lit.: ANEPSA-Sonderbericht
 Beginn regelmäßiger Cannabiskonsum (T1+T2) Beginn Konsum illegaler Subst. (außer Cann.; T1+T2) Beginn Störungen aufgr. illeg. Subst. (außer Cann.; T1+T2) Erziehungsstil der Eltern (FEE; T0) und der Beginn des Konsums bzw. von Störungen aufgrund von illegalen Substanzen während des Follow-Ups (T1+T2) 1 Standardisierte ORs bei quantitativen Unabhängigen Variablen: OR entspricht Risikosteigerung bei Erhöhung des Wertes der UV um 1. erhoben zu T0: Lit.: ANEPSA-Sonderbericht.")
31
Beispiel Vulnerabilität: Die Rolle psychischer Störungen Haben vorangehende psychische Störungen einen Einfluss? Deviantes Verhalten und Hyperaktivitätsstörungen Angst- und depressive Störungen Trauma-bezogene Störungen Andere Substanzstörungen Spielt Erziehungsstil eine Rolle? Temperament und behavioral inhibition

32
Erhebliche erhöhte psychische Morbiditätsraten bei Ecstasy- und anderen Drogenkonsumenten %

33
Jugendliche mit Ecstasykonsum und psychischen Störungen: Was beginnt früher? Konsum Ecstasy:

34
XTC und komorbide psychische Störungen (DSM-IV): Prospektive Befunde 1995 1999 Probanden ohne XTC-KonsumProbanden ohne psychische Störung DX psych - Dx psych. +XTC -XTC + 22.2%32.2% Dx psych. + 3.8%5.8% XTC + OR = 1.9* OR = 2.4* Schuetz et al., in press

35
BI in der Kindheit OR 1 1.5* 1.3* Beginn von Störungen aufgr. von Cannabis (T1+T2) Beginn regelmäßiger Cannabiskonsum (T1+T2) Beginn Konsum illegaler Subst. (außer Cann.; T1+T2) Beginn Störungen aufgr. illeg. Subst. (außer Cann.; T1+T2) Behavioral Inhibition in der Kindheit (BI, T0) und der Beginn des Konsums bzw. von Störungen aufgrund von illegalen Substanzen während des Follow-Up (T1+T2) 1 Standardisierte ORs bei quantitativen Unabhängigen Variablen: OR entspricht Risikosteigerung bei Erhöhung des Wertes der UV um 1. 1.2* erhoben zu T0: Lit.: ANEPSA-Sonderbericht
 Beginn regelmäßiger Cannabiskonsum (T1+T2) Beginn Konsum illegaler Subst. (außer Cann.; T1+T2) Beginn Störungen aufgr. illeg. Subst. (außer Cann.; T1+T2) Behavioral Inhibition in der Kindheit (BI, T0) und der Beginn des Konsums bzw. von Störungen aufgrund von illegalen Substanzen während des Follow-Up (T1+T2) 1 Standardisierte ORs bei quantitativen Unabhängigen Variablen: OR entspricht Risikosteigerung bei Erhöhung des Wertes der UV um * erhoben zu T0: Lit.: ANEPSA-Sonderbericht.")
36
Cannabiskonsum bei Personen ohne und mit verschiedenen psychischen Störungen (lifetime, T0) kum. lifetime-Cannabiskonsum in % (T0+T1) Ohne die spez. Störung Mit Angststörung Mit Depression Mit Alkoholstörung Mit irgendeiner anderen Störung jemals regelmäßig jemals regelmäßig jemals regelmäßig jemals regelmäßig Cannabis- konsum Höfler et al., 1999
 Ohne die spez. Störung Mit Angststörung Mit Depression Mit Alkoholstörung Mit irgendeiner anderen Störung jemals regelmäßig jemals regelmäßig jemals regelmäßig jemals regelmäßig Cannabis- konsum Höfler et al.,")
37
Angststörungen und andere psych. Störungen als Risikofaktoren für nachfolgende Substanzstörungen Soziale Ängste: Risikofaktoren für Progression zu Nikotinabhängigkeit – aber nicht Gebrauch (Sonntag et al., 2000) Soziale Phobie und Panik: Risikofaktoren für Alkoholprobleme (Zimmermann et al., submitted) Angst- und depressive Störungen: Risikofaktor für den Beginn von Störungen aufgrund illegaler Substanzen Ecstasy-Konsumenten: Hohe Belastung durch psychische Störungen, wobei diese überwiegend bereits vor dem Konsum vorlagen (von Sydow et al., 2002) – Progression zu Störungen! Nikotin- und Alkoholabhängigkeit: Risikofaktor für Konsum und Progression von Störungen
 Soziale Phobie und Panik: Risikofaktoren für Alkoholprobleme (Zimmermann et al., submitted) Angst- und depressive Störungen: Risikofaktor für den Beginn von Störungen aufgrund illegaler Substanzen Ecstasy-Konsumenten: Hohe Belastung durch psychische Störungen, wobei diese überwiegend bereits vor dem Konsum vorlagen (von Sydow et al., 2002) – Progression zu Störungen. Nikotin- und Alkoholabhängigkeit: Risikofaktor für Konsum und Progression von Störungen.")
38
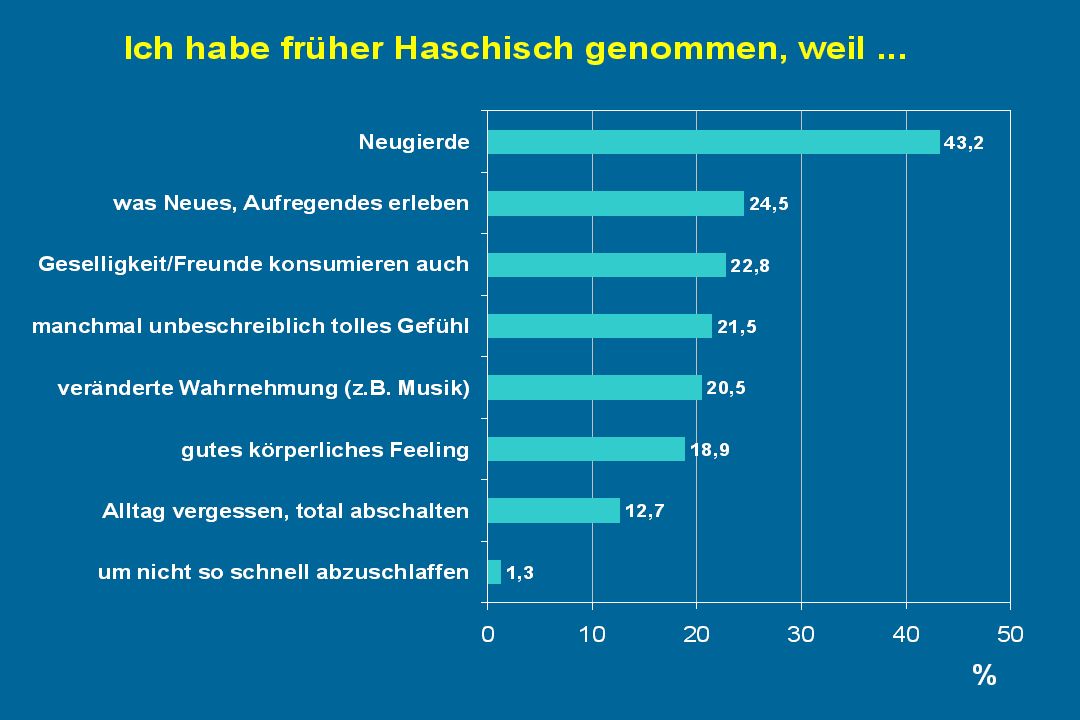
Die Motivation für Drogeneinnahme ändert sich in Abhängigkeit von Frequenz und Stadium

39
Die Motivation für den Ausstieg ist substanzspezifisch unterschiedlich!

40
Pure and multiple substance use disorders for each diagnostic group among those with dis X how many (%) also have disorder Y weighted %, because of multiple disorder numbers sum up to more than 100%
 also have disorder Y weighted %, because of multiple disorder numbers sum up to more than 100%")
41
Bereits bei Jugendlichen und jungen Erwachsenen: hohe Komorbidität von Missbrauch/Abhängigkeit psychotroper Substanzen N = 2548; gewichtete Daten; cum. T0/T1/T2 Daten der EDSP Studie; % in Diagonalen: Anteil an Personen mit „reinen“ Substanzstörungen, d.h. Missbrauch/Abhängigkeit alleine von der jeweiligen Substanz(klasse)
.")
42
Überblick: Wie viele haben insgesamt bis zum 3. Erhebungszeitpunkt der Untersuchung (2000) die Kriterien einer Substanzstörung erfüllt?
 die Kriterien einer Substanzstörung erfüllt .")
43
Erstauftretensalter des Konsums illegaler Drogen nach elterlicher Alkoholbelastung Lieb et al., 2001

44
Elterliche Alkoholbelastung und die Entwicklung von Suchtproblemen bei ihren Kindern kum. Lebenszeitprävalenz in % (T0+T1+T2) CUMOR=2.0* OR=2.1* gelegentlicher Konsum Missbrauch oder Abhängigkeit regelmäßiger Konsum Elterliche Alkohol- belastung: Nein Ja Lieb et al., 2001
 CUMOR=2.0* OR=2.1* gelegentlicher Konsum Missbrauch oder Abhängigkeit regelmäßiger Konsum Elterliche Alkohol- belastung: Nein Ja Lieb et al.,")
Ähnliche Präsentationen











 e.V. www.barrierefrei- kommunizieren.de Blended Learning for people with disabilities.>")


 András Bárdossy IWS Universität Stuttgart.>")


 The dependence of convection-related parameters on surface and.>")

 but young men are no.>")
