Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Leitlinien aus fachärztlicher Sicht
Gerd Rettig-Stürmer Klinik für Innere Medizin Knappschaftskrankenhaus Sulzbach Akademisches Lehrkrankenhaus der Universität des Saarlandes Prof. Dr. jur. Robert Francke, Universität Bremen, bei der 6. Leitlinienkonferenz der AWMF berichtete, sind aus der Sicht der Juristen Leitlinien generelle und abstrakte Regeln für ärztliche Tätigkeiten im Sinne von komplexen Aussagen für klar definierte Behandlungssituationen. Leitlinien sind deshalb nicht nur ausschließlich ein System von naturwissenschaftlichen Eigengesetzlichkeiten und Handlungsempfehlungen, sondern sie haben auch stets normativen und wertenden Charakter. Leitlinien treffen deshalb Handlungsempfehlungen und Ableitungen aus empirischen, wissenschaftlich gesicherten Grundlagen. Sie basieren in der Regel auf Wirksamkeitsbeurteilungen sowie auf Risikoabwägungen und Nutzenkalkülen. Allerdings müssen wirtschaftliche Überlegungen stets hinter der medizinischen Zielsetzung zurückstehen. Leitlinien bedeuten die Festlegung von Orientierungsmarken und Handlungskorridoren, die ein "gutes ärztliches Handeln" nach dem jeweils anerkannten aktuellen Stand der medizinischen Wissenschaft ermöglichen sollen. Prinzipiell sollen und dürfen nach dem Verständnis der Fachgesellschaften bei der Entwicklung von Leitlinien wirtschaftliche Überlegungen nicht inhaltliche Aspekte dominieren. Leitlinien sollen die Entscheidung des Arztes unterstützen, mithin Handlungsalternativen und einen begrenzten Handlungsspielraum aufzeigen und vorgeben, aber keine Festlegung nach Standards programmieren. Nach Darlegung von Prof. Dr. jur. Dieter Hart, Universität Bremen, dienen Leitlinien auch und in erster Linie der Qualitätssicherung des ärztlichen Handelns und mithin auch dem Patientenschutz. "Sie sind institutionelle Festsetzungen von methodischen und sachlichen Standards ärztlichen Handelns, die in einem geordneten Verfahren zustande gekommen sind."

2
Medizinische Leitlinien
Systematisch entwickelte Entscheidungshilfen über die angemessene ärztliche Vorgehensweise bei speziellen gesundheitlichen Problemen („Systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances“) Institute of Medicine. Clinical practice guidelines. Directions for a new program. Washington, DC: National Academy Press; 1990 Medizinische Leitlinien sind "systematisch entwickelte Hilfen zur Entscheidungsfindung über die angemessene ärztliche Vorgehensweise bei speziellen gesundheitlichen Problemen" und damit eine Orientierungshilfe im Sinne von "Handlungs- und Entscheidungsoptionen", von der in begründeten Fällen abgewichen werden kann oder sogar muss. Sie sind systematisch entwickelte und wissenschaftlich begründete und praxisorientierte Handlungsempfehlungen. Ihr Hauptzweck ist die Darstellung des fachlichen Entwicklungsstandes einer Profession (state of art). Sie geben den Angehörigen dieser Profession Orientierung im Sinne von Entscheidungs- und Handlungsoptionen, von denen in begründeten Fällen abgewichen werden kann oder sogar muss. Die Umsetzung liegt also im Ermessensspielraum des Arztes oder der Ärztin bei der fallspezifischen Betrachtung, ebenso sind im Einzelfall die Präferenzen der Patienten in die Entscheidungsfindung einzubeziehen. Bei einer evidenz- und konsensbasierten Leitlinie handelt es sich um den nach einem definierten, transparent gemachten Vorgehen erzielten Konsens multidisziplinärer Expertengruppen zu bestimmten Vorgehensweisen in der Medizin unter Berücksichtigung der besten verfügbaren "Evidenz". Grundlage dieses Konsenses ist die systematische Recherche und Analyse der wissenschaftlichen "Evidenz" aus Klinik und Praxis. L sind rechtlich nicht bindend und haben daher weder haftungsbegründende noch haftungsbefreiende Wirkung
 Institute of Medicine. Clinical practice guidelines. Directions for a new program. Washington, DC: National Academy Press; Medizinische Leitlinien sind systematisch entwickelte Hilfen zur Entscheidungsfindung über die angemessene ärztliche Vorgehensweise bei speziellen gesundheitlichen Problemen und damit eine Orientierungshilfe im Sinne von Handlungs- und Entscheidungsoptionen , von der in begründeten Fällen abgewichen werden kann oder sogar muss. Sie sind systematisch entwickelte und wissenschaftlich begründete und praxisorientierte Handlungsempfehlungen. Ihr Hauptzweck ist die Darstellung des fachlichen Entwicklungsstandes einer Profession (state of art). Sie geben den Angehörigen dieser Profession Orientierung im Sinne von Entscheidungs- und Handlungsoptionen, von denen in begründeten Fällen abgewichen werden kann oder sogar muss. Die Umsetzung liegt also im Ermessensspielraum des Arztes oder der Ärztin bei der fallspezifischen Betrachtung, ebenso sind im Einzelfall die Präferenzen der Patienten in die Entscheidungsfindung einzubeziehen. Bei einer evidenz- und konsensbasierten Leitlinie handelt es sich um den nach einem definierten, transparent gemachten Vorgehen erzielten Konsens multidisziplinärer Expertengruppen zu bestimmten Vorgehensweisen in der Medizin unter Berücksichtigung der besten verfügbaren Evidenz . Grundlage dieses Konsenses ist die systematische Recherche und Analyse der wissenschaftlichen Evidenz aus Klinik und Praxis. L sind rechtlich nicht bindend und haben daher weder haftungsbegründende noch haftungsbefreiende Wirkung.")
3
Desirable attributes of clinical practice guidelines (CPG)
Validity, reliability and reproducibility, clinical applicability, clinical flexibility, clarity, documentation, development by a multidisciplinary process, and plans for review. Eigenschaften erfüllen: Gültigkeit, Stichhaltigkeit, Verläßlichkeit Externe Qualitätssicherung Institute of Medicine. Guidelines for Clinical Practice: From Development to Use. Washington, DC: National Academy Pr; 1992.

4
Medizinische Leitlinien
Orientierungshilfe im Sinne von "Handlungs- und Entscheidungskorridoren“ auf der Basis des aktuellen Wissensstandards („state of the art“) Versuch, die steigende Informationsflut unter Zuhilfe-nahme von Expertenmeinungen zu einem praktikablen Format zu destillieren Wissenschaftlich begründet, praxisorientiert Instrument, Entscheidungen der medizinischen Versorg-ung auf rationale Basis zu stellen . Versuch, to distill large body of medical knowledge into a convenient readily usable format. Loke overviews they gather, appraise and combine evidence. Giudelines, however, must go beyond overviews in attempting to address all the issues relevant to a clinical decision and all the values that might sway a clinical recommendation. Like decision analysis they refine clinical questions and balance trade-offs. G differ from d in relying more on qualitative reasoning and in emphasizing a particular clinical context. Reflect value judgments about relative importance of various health and economic outcomes in specific clinical situation. Hoher Anspruch, Qualitätsstandards erforderlich. Aktuell max 20% der Erkrankungen durch Leitlinien angedeckt
 Versuch, die steigende Informationsflut unter Zuhilfe-nahme von Expertenmeinungen zu einem praktikablen Format zu destillieren. Wissenschaftlich begründet, praxisorientiert. Instrument, Entscheidungen der medizinischen Versorg-ung auf rationale Basis zu stellen . Versuch, to distill large body of medical knowledge into a convenient readily usable format. Loke overviews they gather, appraise and combine evidence. Giudelines, however, must go beyond overviews in attempting to address all the issues relevant to a clinical decision and all the values that might sway a clinical recommendation. Like decision analysis they refine clinical questions and balance trade-offs. G differ from d in relying more on qualitative reasoning and in emphasizing a particular clinical context. Reflect value judgments about relative importance of various health and economic outcomes in specific clinical situation. Hoher Anspruch, Qualitätsstandards erforderlich. Aktuell max 20% der Erkrankungen durch Leitlinien angedeckt.")
5
Qualitative Bewertung Leitlinie Empfehlungen
Übersicht Entscheidungsanalyse sammelt Daten quantifiziert Optionen Qualitative Bewertung Wie eine Übersicht trägt die Leitlinie das wiss Material zusammen, geht aber darüberhinaus, indem sie alle für eine klinische Entscheidung notwendigen Argumente also auch zB ökonomische Aspekte einbezieht. Wie bei einer klinischen Entscheidungsanalyse müssen pro und contra nach den verfügbaren Daten quantitativ gegeneinander abgewogen, darüberhinaus aber auch für den Einzelfall qualitativ bewertet werden. Dies impliziert die Notwendigkeit, nicht nur über medizinische sondern auch über ethische, ökonomische und soziologische Werte zu urteilen, ein außerordentlich hoher Anspruch, der entsprechend hohe Qualitätsstandards für die Verfassung von Leitlinien voraussetzt. Dazu gehört naturgemäß eine ausreichende Datenlage; ist diese noch unzureichend, läßt sich oft wenigstens ein C entstehen, aus dem dann Voschläge abgeleitet werden können. Die formale Leitlinie spricht dagegen Empfehlungen aus Loke overviews they gather, appraise and combine evidence. Giudelines, however, must go beyond overviews in attempting to address all the issues relevant to a clinical decision and all the values that might sway a clinical recommendation. Like decision analysis they refine clinical questions and balance trade-offs. G differ from d in relying more on qualitative reasoning and in emphasizing a particular clinical context. Reflect value judgments about relative importance of various health and economic outcomes in specific clinical situation. Hoher Anspruch, Qualitätsstandards erforderlich. Consensus statement: vorläufig, wenn Daten nicht ausreichen, um formale Leitlinie zu formulieren: suggestions vs recommendations Consensus-Papier Vorschläge Leitlinie Empfehlungen

6
Medizinische Leitlinien (2)
Leitlinien haben also normativen und wertenden Cha-rakter, indem sie Handlungsalternativen und einen be-grenzten Handlungsspielraum aufzeigen und vorgeben. Bedeuten dennoch keine Programmierung nach festge-legten Standards. Die Umsetzung liegt im Ermessensspielraum des Arztes bei der fallspezifischen Betrachtung unter Einbeziehung der Präferenzen des Patienten. Leitlinien sind rechtlich nicht bindend und haben daher weder haftungsbegründende noch haftungsbefreiende Wirkung. Versuch, to distill large body of medical knowledge into a convenient readily usable format. Loke overviews they gather, appraise and combine evidence. Giudelines, however, must go beyond overviews in attempting to address all the issues relevant to a clinical decision and all the values that might sway a clinical recommendation. Like decision analysis they refine clinical questions and balance trade-offs. G differ from d in relying more on qualitative reasoning and in emphasizing a particular clinical context. Reflect value judgments about relative importance of various health and economic outcomes in specific clinical situation. Hoher Anspruch, Qualitätsstandards erforderlich. Aktuell max 20% der Erkrankungen durch Leitlinien angedeckt Hoffe, nicht unseren juristischen Experten vorzugreifen, indem ich meiner Überzeugung Ausdruck gebe, daß…..

7
Empfehlungen der Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften
Guter Gesellschaft, darf mich ausdrücklich auf… beziehen, denen diese Formulierung wörtlich entnommen ist

8
Leitlinie Übersicht Entscheidungsanalyse
sammelt Daten quantifiziert Optionen Leitlinie Bewertet qualitativ Individuell: Ermessensspielraum erforderlich Durch „Evidenzgrade“ exemplifiziert Daher: keine rechtliche Verpflichtung Loke overviews they gather, appraise and combine evidence. Giudelines, however, must go beyond overviews in attempting to address all the issues relevant to a clinical decision and all the values that might sway a clinical recommendation. Like decision analysis they refine clinical questions and balance trade-offs. G differ from d in relying more on qualitative reasoning and in emphasizing a particular clinical context. Reflect value judgments about relative importance of various health and economic outcomes in specific clinical situation. Hoher Anspruch, Qualitätsstandards erforderlich.

9
Hierarchie Gesetze, Verordnungen Richtlinien müssen Leitlinien sollen
Empfehlungen können beachtet werden Es gibt eine allgemein anerkannte Hierarchie und systematische Abgrenzung zwischen Gesetzen, Verordnungen, Richtlinien, Leitlinien und Empfehlungen. Gesetze, Verordnungen und (offizielle) Richtlinien, die auf gesetzlichen Grundlagen basieren, müssen beachtet werden, Leitlinien sollen beachtet und Empfehlungen können beachtet werden. Allerdings erhielten zum 1. Januar 2000 medizinische Leitlinien durch ihre Verankerung im SGB V gegenüber der früheren Rechtslage einen mehr justiziablen, rechtsvollzugsverbindlichen Stellenwert. Infolge des rasch voranschreitenden medizinischen und technischen Fortschritts und der raschen Erneuerung und Überholung des aktuellen Wissensstandes müssen Leitlinien ständig fachgerecht angepasst und aktualisiert werden. Sie müssen mit einem relativ kurzfristigen, den Anwendern bekannt zu gebenden Verfalldatum versehen sein. Experten veranschlagen die Dauer der Gültigkeit von Leitlinien auf zwei Jahre; schließlich wird im Durchschnitt alle fünf Jahre das medizinische Wissen durch die neueren Entwicklungen überholt.
 Richtlinien, die auf gesetzlichen Grundlagen basieren, müssen beachtet werden, Leitlinien sollen beachtet und Empfehlungen können beachtet werden. Allerdings erhielten zum 1. Januar 2000 medizinische Leitlinien durch ihre Verankerung im SGB V gegenüber der früheren Rechtslage einen mehr justiziablen, rechtsvollzugsverbindlichen Stellenwert. Infolge des rasch voranschreitenden medizinischen und technischen Fortschritts und der raschen Erneuerung und Überholung des aktuellen Wissensstandes müssen Leitlinien ständig fachgerecht angepasst und aktualisiert werden. Sie müssen mit einem relativ kurzfristigen, den Anwendern bekannt zu gebenden Verfalldatum versehen sein. Experten veranschlagen die Dauer der Gültigkeit von Leitlinien auf zwei Jahre; schließlich wird im Durchschnitt alle fünf Jahre das medizinische Wissen durch die neueren Entwicklungen überholt.")
10
Califf RM, De Mets DL. Circulation 2002;106:1172-1175
Optimal Aufbau am linken Rand der Pyramide Califf RM, De Mets DL. Circulation 2002;106:

11
Sinn von medizinischen Leitlinien
Qualitätsverbesserung für den individuellen Patienten Verbesserung der medizinischen Versorgung der Bevölkerung Vermeidung Über-Unter-Fehlversorgung Kostenbegrenzung Liegedauer Diagnostik Rationelle Therapie Resourcenverbrauch

12
Nutzen nicht einheitlich, da Definition von Qualität verschieden
Patient Arzt (Krankenhaus- vs. niedergelassener, Gebiets- vs Allgemeinarzt, versch. Fachrichtungen) Krankenhausträger Kostenträger Öffentliches Gesundheitswesen, Politik (IQWiG) Gesellschaft, Öffentlichkeit, Medien (Forschende) Pharmaindustrie Versch Parteien im Ges wesen durchaus verschiedene Auffassungen von Qualität und verbinden damit untersch Ansprüche, Forderungen an Leitlinien zB Insulin, Ca-Antag, AZM-Steuerung, Sortis
 Krankenhausträger. Kostenträger. Öffentliches Gesundheitswesen, Politik (IQWiG) Gesellschaft, Öffentlichkeit, Medien. (Forschende) Pharmaindustrie. Versch Parteien im Ges wesen durchaus verschiedene Auffassungen von Qualität und verbinden damit untersch Ansprüche, Forderungen an Leitlinien. zB Insulin, Ca-Antag, AZM-Steuerung, Sortis.")
13
Patient - Nutzen Steigerung der Qualität der medizinischen Versorgung
Vereinheitlichung der Versorgung Wissenschaftlicher Fortschritt schneller in die Praxis umsetzbar Bessere Möglichkeiten der Information, Auswahl, kriti-scher Wertung durch vielfältige Mediennutzung Stärkere Einflußnahme auf Politik über Mißstände, Unterversorgung, Ungerechtigkeiten, Wahrung der Interessen von Minderheiten

14
Medizinische Leistungsträger: Nutzen
Steigerung der Qualität der medizinischen Versorgung Fördert Sicherheit der Entscheidung durch rasche autorisierte Information Fördert kritische Bestandsaufnahme des Wissens-standes, Steuerungsfunktion Basis für Rechtfertigung gegenüber Politik, Verwaltung, Kostenträgern Schutz bei juristischen Auseinandersetzungen Basis für professionelle Weiterbildung Fördert kritische Bestandsaufnahme des Wissensstandes: wo ist Evidenz schwach, wo Verbesserungen,

15
Kostenträger und Öffentliches Gesundheitswesen: Nutzen
Verbesserte Effizienz der Versorgung Erhöhte Transparenz Bessere Steuerbarkeit Kostenbegrenzung durch Rationalisierung Positives Bild in der öffentlichen Meinung Transparenz: besser zu kontrollieren, auch der Geldströme Liegedauer, Prozeduren, amb Operationen, Doppeldiagnostik, Rationalisierung

16
Merkmale qualitativ hochstehender Leitlinien
Fachliche Kompetenz eines repräsentativen Berater-gremiums Repräsentative Darstellung der wissenschaftlichen Belege Qualitative Wertung für praktische Entscheidungsfindung Umfassende, erschöpfende Darstellung von quantitativem Nutzen, Risiko, praktische Voraussetzungen, Praktikabili-tät, Kosten (-effektivität), Patientenpräferenzen Aktualität Imprimatur renommierter Fachgesellschaften Externe Qualitätskontrolle Vorsuasstzung für solcherlei erwarteten Nutzen: Qualität
, Patientenpräferenzen. Aktualität. Imprimatur renommierter Fachgesellschaften. Externe Qualitätskontrolle. Vorsuasstzung für solcherlei erwarteten Nutzen: Qualität.")
17
AWMF Auswahl des Leitlinienthemas Prioritärer Versorgungsaspekt
Leitlinienführungsgruppe Autoren, Verantwortliche Logische Analyse des Versorgungsablaufs, der Entscheidungsprozesse Formulierung der ersten Statements Leitlinienführungsgruppe bildet den Rahmen Leitliniengruppe Beteiligung aller relevanten Professionen und Betroffenen Erster Konsensusprozess über die ersten Statements: Eckpunkte der Leitlinie EbM-Gruppe Paare: Kliniker+ Methodiker Evidenzbasierte Medizin Systematische Recherche und Bewertung der Literatur Outcome-Analyse Ermittlung relevanter Endpunkte, qualitative Analyse Leitlinienführungsgruppe und EbM-Gruppe Entscheidungsanalyse Quantitativer Vergleich der Endpunkte: Kosten, Nutzen, Risiko Leitliniengruppe Beteiligung aller relevanten Professionen und Betroffenen Zweiter Konsensusprozess über die veränderten Statements und den Gesamttext Externe Begutachtung, Pilottestung Leitlinienführungsgruppe Autoren, Verantwortliche Finale Formulierung der Leitlinie Kurzversion, Langversion, Patientenversion, Methodikreport Disseminierung, Implementierung, Evaluation

18
Ergebnisse bei angemessener Befolgung von qualitativ hochstehenden Leitlinien
Wenn solche Vorausstzungen erfüllt, auch gute Ergebnisse

19
Adherence to guidelines is a predictor of outcome in chronic heart failure
Befolgung Figure 1 Kaplan–Meier curve of cardiovascular hospitalizations according to GAI3 tertiles. See Supplementary material online for a colour version of this figure. TI - Adherence to guidelines is a predictor of outcome in chronic heart failure: the MAHLER survey. AU - Komajda M; Lapuerta P; Hermans N; Gonzalez-Juanatey JR; van Veldhuisen DJ; Erdmann E; Tavazzi L; Poole-Wilson P; Le Pen C SO - Eur Heart J Aug;26(16): Epub 2005 Apr 12. AIMS: The impact on outcome of the implementation of European guidelines for the treatment of chronic heart failure (CHF) has not been evaluated. We investigated the consequences of adherence to care by cardiologists on the rate of CHF and cardiovascular (CV) hospitalizations and time to CV hospitalization. METHODS AND RESULTS: We constructed class adherence indicators for angiotensin-converting enzyme (ACE)-inhibitors, beta-blockers, spironolactone, diuretics, and cardiac glycosides and GAIs (GAI3 adherence to first three classes of heart failure medication, GAI5 adherence to five classes). In the study, 1410 evaluable patients (mean age 69, 69% males, New York Heart Association (NYHA) II: 64%, III: 34%, IV: 2%) were enrolled and followed up for 6 months by 150 randomly selected cardiologists/cardiology departments from six European countries (France, Germany, Italy, The Netherlands, Spain, and UK). Overall, adherence to treatment guidelines was 60 (GAI3) and 63% (GAI5) and was better for ACE-I (88%) or diuretics (82%) than for cardiac glycosides (52%), beta-blockers (58%), and spironolactone (36%). In the three tertiles of the population defined by a decreasing mean adherence score value, CHF and CV hospitalization rates were, respectively, 6.7, 9.7, and 14.7% and 11.2, 15.9, and 20.6% (P<0.002 and P<0.001, respectively). Global adherence indicator GAI3 was an independent predictor of time to CV hospitalization in a multi-variable model together with NYHA Class, history of CHF hospitalization, ischaemic aetiology, diabetes mellitus, and hypertension. CONCLUSION: We demonstrate that adherence of physicians to treatment guidelines is a strong predictor of fewer CV hospitalizations in actual practice. There is a need to develop further quality improvement programmes in this condition. Komajda M et al. Eur Heart J 2005;26:
: Epub 2005 Apr 12. AIMS: The impact on outcome of the implementation of European guidelines for the treatment of chronic heart failure (CHF) has not been evaluated. We investigated the consequences of adherence to care by cardiologists on the rate of CHF and cardiovascular (CV) hospitalizations and time to CV hospitalization. METHODS AND RESULTS: We constructed class adherence indicators for angiotensin-converting enzyme (ACE)-inhibitors, beta-blockers, spironolactone, diuretics, and cardiac glycosides and GAIs (GAI3 adherence to first three classes of heart failure medication, GAI5 adherence to five classes). In the study, 1410 evaluable patients (mean age 69, 69% males, New York Heart Association (NYHA) II: 64%, III: 34%, IV: 2%) were enrolled and followed up for 6 months by 150 randomly selected cardiologists/cardiology departments from six European countries (France, Germany, Italy, The Netherlands, Spain, and UK). Overall, adherence to treatment guidelines was 60 (GAI3) and 63% (GAI5) and was better for ACE-I (88%) or diuretics (82%) than for cardiac glycosides (52%), beta-blockers (58%), and spironolactone (36%). In the three tertiles of the population defined by a decreasing mean adherence score value, CHF and CV hospitalization rates were, respectively, 6.7, 9.7, and 14.7% and 11.2, 15.9, and 20.6% (P<0.002 and P<0.001, respectively). Global adherence indicator GAI3 was an independent predictor of time to CV hospitalization in a multi-variable model together with NYHA Class, history of CHF hospitalization, ischaemic aetiology, diabetes mellitus, and hypertension. CONCLUSION: We demonstrate that adherence of physicians to treatment guidelines is a strong predictor of fewer CV hospitalizations in actual practice. There is a need to develop further quality improvement programmes in this condition. Komajda M et al. Eur Heart J 2005;26:")
20
Association Between Hospital Process Performance and Outcomes Among Patients With Acute Coronary Syndromes igure 2. Association Between Hospital Composite Guideline Adherence Rate and In-Hospital MortalityNSTE ACS indicates non–ST-segment elevation acute coronary syndrome; NSTEMI, non–ST-segment elevation myocardial infarction. Three hundred fifty hospitals are grouped by composite guideline adherence into quartiles. The left plot shows risk-adjusted mortality rates for overall patients with NSTE ACS for that quartile, and the right plot shows risk-adjusted mortality rates for the NSTEMI subgroup. Standard error bars are also included for each group. All results were adjusted for age, sex, race, body mass index, patient insurance status, admission electrocardiograph (ST depression, transient ST elevation), admission cardiac marker status, presenting signs of heart failure, initial heart rate and systolic blood pressure, history of hypertension, diabetes mellitus, hypercholesterolemia, renal insufficiency, prior myocardial infarction, prior percutaneous coronary intervention, prior coronary artery bypass graft surgery, prior congestive heart failure, prior stroke, current/recent smoker, and family history of coronary disease Peterson ED et al. JAMA 2006;295:
, admission cardiac marker status, presenting signs of heart failure, initial heart rate and systolic blood pressure, history of hypertension, diabetes mellitus, hypercholesterolemia, renal insufficiency, prior myocardial infarction, prior percutaneous coronary intervention, prior coronary artery bypass graft surgery, prior congestive heart failure, prior stroke, current/recent smoker, and family history of coronary disease. Peterson ED et al. JAMA 2006;295:")
21
Association Between Hospital Process Performance and Outcomes Among Patients With Acute Coronary Syndromes: CRUSADE Figure 2 Link between American College of Cardiology/American Heart Association guideline adherence (hospital composite quality quartiles) and in-hospital mortality. Every 10% increase in guideline adherence was associated with a 10% reduction in in-hospital mortality (adapted from Peterson et al. [31]). *Adjusted for age, gender, body mass index, race, insurance status, family history of coronary disease, hypertension, diabetes, smoking, hypercholesterolemia, prior myocardial infarction/percutaneous coronary intervention/coronary bypass surgery/congestive heart failure/stroke, renal insufficiency, blood pressure, heart rate, ST-segment shift, and positive cardiac biomarkers. Context Selected care processes are increasingly being used to measure hospital quality; however, data regarding the association between hospital process performance and outcomes are limited. Objectives To evaluate contemporary care practices consistent with the American College of Cardiology/American Heart Association (ACC/AHA) guideline recommendations, to examine how hospital performance varied among centers, to identify characteristics predictive of higher guideline adherence, and to assess whether hospitals' overall composite guideline adherence was associated with observed and risk-adjusted in-hospital mortality rates. Design, Setting, and Participants An observational analysis of hospital care in 350 academic and nonacademic US centers of 64 775 patients enrolled in the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines) National Quality Improvement Initiative between January 1, 2001, and September 30, 2003, presenting with chest pain and positive electrocardiographic changes or cardiac biomarkers consistent with non–ST-segment elevation acute coronary syndrome (ACS). Main Outcome Measures Use of 9 ACC/AHA class I guideline-recommended treatments and the correlation among hospitals' use of individual care processes as well as overall composite adherence rates. Results Overall, the 9 ACC/AHA guideline-recommended treatments were adhered to in 74% of eligible instances. There was modest correlation in hospital performance among the individual ACS process metrics. However, composite adherence performance varied widely (median [interquartile range] composite adherence scores from lowest to highest hospital quartiles, 63% [59%-66%] vs 82% [80%-84%]). Composite guideline adherence rate was significantly associated with in-hospital mortality, with observed mortality rates decreasing from 6.31% for the lowest adherence quartile to 4.15% for the highest adherence quartile (P<.001). After risk adjustment, every 10% increase in composite adherence at a hospital was associated with an analogous 10% decrease in its patients' likelihood of in-hospital mortality (adjusted odds ratio, 0.90; 95% confidence interval, ; P<.001). Conclusion A significant association between care process and outcomes was found, supporting the use of broad, guideline-based performance metrics as a means of assessing and helping improve hospital quality. Peterson ED et al. JAMA 2006;295:
 and in-hospital mortality. Every 10% increase in guideline adherence was associated with a 10% reduction in in-hospital mortality (adapted from Peterson et al. [31]). *Adjusted for age, gender, body mass index, race, insurance status, family history of coronary disease, hypertension, diabetes, smoking, hypercholesterolemia, prior myocardial infarction/percutaneous coronary intervention/coronary bypass surgery/congestive heart failure/stroke, renal insufficiency, blood pressure, heart rate, ST-segment shift, and positive cardiac biomarkers. Context Selected care processes are increasingly being used to measure hospital quality; however, data regarding the association between hospital process performance and outcomes are limited. Objectives To evaluate contemporary care practices consistent with the American College of Cardiology/American Heart Association (ACC/AHA) guideline recommendations, to examine how hospital performance varied among centers, to identify characteristics predictive of higher guideline adherence, and to assess whether hospitals overall composite guideline adherence was associated with observed and risk-adjusted in-hospital mortality rates. Design, Setting, and Participants An observational analysis of hospital care in 350 academic and nonacademic US centers of patients enrolled in the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines) National Quality Improvement Initiative between January 1, 2001, and September 30, 2003, presenting with chest pain and positive electrocardiographic changes or cardiac biomarkers consistent with non–ST-segment elevation acute coronary syndrome (ACS). Main Outcome Measures Use of 9 ACC/AHA class I guideline-recommended treatments and the correlation among hospitals use of individual care processes as well as overall composite adherence rates. Results Overall, the 9 ACC/AHA guideline-recommended treatments were adhered to in 74% of eligible instances. There was modest correlation in hospital performance among the individual ACS process metrics. However, composite adherence performance varied widely (median [interquartile range] composite adherence scores from lowest to highest hospital quartiles, 63% [59%-66%] vs 82% [80%-84%]). Composite guideline adherence rate was significantly associated with in-hospital mortality, with observed mortality rates decreasing from 6.31% for the lowest adherence quartile to 4.15% for the highest adherence quartile (P<.001). After risk adjustment, every 10% increase in composite adherence at a hospital was associated with an analogous 10% decrease in its patients likelihood of in-hospital mortality (adjusted odds ratio, 0.90; 95% confidence interval, ; P<.001). Conclusion A significant association between care process and outcomes was found, supporting the use of broad, guideline-based performance metrics as a means of assessing and helping improve hospital quality. Peterson ED et al. JAMA 2006;295:")
22
Secondary prevention: combination evidence-based therapies reduce mortality to 1 year following myocardial infarction independent of renal function Figure 3 Combination evidence-based therapies reduce mortality to 1 year following myocardial infarction independent of renal function. Patients receiving multiple clinical practice guideline-adherent medications (antiplatelet agents, beta-blockers, lipid-lowering agents, angiotensin-converting enzyme inhibitors) enjoy incremental survival benefit. Adapted from Tay et al. (62). GFR = glomerular filtration rate; CI = confidence interval. Tay et al. from: Peterson ED et al. JAMA 2006;295:
 enjoy incremental survival benefit. Adapted from Tay et al. (62). GFR = glomerular filtration rate; CI = confidence interval. Tay et al. from: Peterson ED et al. JAMA 2006;295:")
23
Implementation of an evidence-based "standard operating procedure" and outcome in septic shock.
Jan – Aug Sept Aug 2003 Patient No Dobutamine use 2/30 12/30 Glucose <150 mg/dl day 4 13/25 26/28 Hydrocortisone 13/30 30/30 rcAPC 0/30 7/30 Mortality 53% 27% Andere Beispiele: Mamma-Ca, Lymphome, Kortgen A et al. Crit Care Med 2006;34:

24
Umsetzung in der Realität ?

25
Frequency Distribution of Sites' Composite Adherence Score
The bars display the number of hospitals with a given composite adherence score (N = 350 hospitals Peterson ED et al. JAMA 2006;295:

26
Umfrage unter Pat mit Überprüfung ihrer Krankenblätter
Background We have little systematic information about the extent to which standard processes involved in health care — a key element of quality — are delivered in the United States. Methods We telephoned a random sample of adults living in 12 metropolitan areas in the United States and asked them about selected health care experiences. We also received written consent to copy their medical records for the most recent two-year period and used this information to evaluate performance on 439 indicators of quality of care for 30 acute and chronic conditions as well as preventive care. We then constructed aggregate scores. Results Participants received 54.9 percent (95 percent confidence interval, 54.3 to 55.5) of recommended care. We found little difference among the proportion of recommended preventive care provided (54.9 percent), the proportion of recommended acute care provided (53.5 percent), and the proportion of recommended care provided for chronic conditions (56.1 percent). Among different medical functions, adherence to the processes involved in care ranged from 52.2 percent for screening to 58.5 percent for follow-up care. Quality varied substantially according to the particular medical condition, ranging from 78.7 percent of recommended care (95 percent confidence interval, 73.3 to 84.2) for senile cataract to 10.5 percent of recommended care (95 percent confidence interval, 6.8 to 14.6) for alcohol dependence. Conclusions The deficits we have identified in adherence to recommended processes for basic care pose serious threats to the health of the American public. Strategies to reduce these deficits in care are warranted.
 of recommended care. We found little difference among the proportion of recommended preventive care provided (54.9 percent), the proportion of recommended acute care provided (53.5 percent), and the proportion of recommended care provided for chronic conditions (56.1 percent). Among different medical functions, adherence to the processes involved in care ranged from 52.2 percent for screening to 58.5 percent for follow-up care. Quality varied substantially according to the particular medical condition, ranging from 78.7 percent of recommended care (95 percent confidence interval, 73.3 to 84.2) for senile cataract to 10.5 percent of recommended care (95 percent confidence interval, 6.8 to 14.6) for alcohol dependence. Conclusions The deficits we have identified in adherence to recommended processes for basic care pose serious threats to the health of the American public. Strategies to reduce these deficits in care are warranted.")
27
McGlynn EA et al. NEJM 2003;348:1635-1645

28
McGlynn EA et al. NEJM 2003;348:1635-1645

29
In Deutschland sind nur 7-22 % der Hypertoniker kontrolliert
Patienten mit bekanntem, behandeltem und kontrolliertem Blutdruck in Deutschland (%) Bevölkerungs-repräsentative Querschnittsstudie, 1997–2001; n= 3304) Männer Frauen BBK+ BBK+ Unbek. BBK- Unbek. Wie eine große Metaanalyse gezeigt hat, haben wir in Deutschland im internationalen Vergleich die höchste Hypertonie-Prävalenz – hier sind wir Weltmeister. Doch bei der medikamentösen Therapie stehen wir ganz hinten, was sicher mehrere Ursachen hat. BBK- BB- BB- BBK + bekannt, behandelt, kontrolliert BBK - bekannt, behandelt, nicht kontrolliert BB bekannt, nicht behandelt Löwel H et al. Dtsch Med Wschr 2006; 131:
 Bevölkerungs-repräsentative Querschnittsstudie, 1997–2001; n= 3304) Männer. Frauen. BBK+ BBK+ Unbek. BBK- Unbek. Wie eine große Metaanalyse gezeigt hat, haben wir in Deutschland im internationalen Vergleich die höchste Hypertonie-Prävalenz – hier sind wir Weltmeister. Doch bei der medikamentösen Therapie stehen wir ganz hinten, was sicher mehrere Ursachen hat. BBK- BB- BB- BBK + bekannt, behandelt, kontrolliert. BBK - bekannt, behandelt, nicht kontrolliert. BB - bekannt, nicht behandelt. Löwel H et al. Dtsch Med Wschr 2006; 131:")
30
Inadequate Control of Hypertension in US Adults With Cardiovascular Disease Comorbidities in Background Cardiovascular risks associated with hypertension (HTN) and the importance of its control are well established; however, the prevalence and adequacy of its treatment and control in persons with cardiovascular comorbidities (CVCs) are uncertain. Methods To examine the prevalence, treatment, and control of HTN among US adults with and without CVCs, we analyzed data from adults at least 18 years of age (n = 4646, N [projected sample size] = 192.4 million) in the National Health and Nutrition Examination Survey , a nationally representative cross-sectional survey of the noninstitutionalized civilian US population. Prevalence, treatment, and control rates of HTN in patients with CVCs vs those without, including coronary artery disease, congestive heart failure, stroke, chronic kidney disease, peripheral artery disease, and diabetes mellitus, and distance to blood pressure goal in those whose HTN was not controlled were the main outcomes. Results The overall prevalence rate of HTN was 31.4% (n = 1671, N = 60.5 million), ranging from 23.1% in those without CVCs to 51.8% to 81.8% in those with CVCs (P < .01). Despite HTN treatment rates for diabetes mellitus, stroke, heart failure, and coronary artery disease that are higher (83.4%-89.3%) than the rates of those without these conditions (66.5%) (P < .01), control rates for treatment remained poor (23.2%-49.3%) (P < .001 to P = .048). Isolated systolic HTN was the most common hypertensive subtype in those with CVCs ( 63.5%) with systolic blood pressure averaging at least 20 mm Hg from goal. Conclusions Nearly three-fourths of adults with CVCs have HTN. Poor control rates of systolic HTN remain a principal problem that further compromises their already high cardiovascular disease risk. Wong ND et al. Arch Intern Med 2007;167:
 and the importance of its control are well established; however, the prevalence and adequacy of its treatment and control in persons with cardiovascular comorbidities (CVCs) are uncertain. Methods To examine the prevalence, treatment, and control of HTN among US adults with and without CVCs, we analyzed data from adults at least 18 years of age (n = 4646, N [projected sample size] = million) in the National Health and Nutrition Examination Survey , a nationally representative cross-sectional survey of the noninstitutionalized civilian US population. Prevalence, treatment, and control rates of HTN in patients with CVCs vs those without, including coronary artery disease, congestive heart failure, stroke, chronic kidney disease, peripheral artery disease, and diabetes mellitus, and distance to blood pressure goal in those whose HTN was not controlled were the main outcomes. Results The overall prevalence rate of HTN was 31.4% (n = 1671, N = 60.5 million), ranging from 23.1% in those without CVCs to 51.8% to 81.8% in those with CVCs (P < .01). Despite HTN treatment rates for diabetes mellitus, stroke, heart failure, and coronary artery disease that are higher (83.4%-89.3%) than the rates of those without these conditions (66.5%) (P < .01), control rates for treatment remained poor (23.2%-49.3%) (P < .001 to P = .048). Isolated systolic HTN was the most common hypertensive subtype in those with CVCs ( 63.5%) with systolic blood pressure averaging at least 20 mm Hg from goal. Conclusions Nearly three-fourths of adults with CVCs have HTN. Poor control rates of systolic HTN remain a principal problem that further compromises their already high cardiovascular disease risk. Wong ND et al. Arch Intern Med 2007;167:")
31
The EuroHeart Failure Survey programme - a survey on the quality of care among patients with heart failure in Europe Part 2: treatment Rate of prescription of the major heart failure medication in the overall population (%) ACE inhibitors 61.8 (40–85.1) Angiotensin II receptor antagonists 4.5 (1.9–14) Antithrombotic therapy (any) 77.6 (57.7–92.7) Aspirin 29.1 (27.1–73.0) Beta-Blockers 36.9 (10.0–65.8) Calcium channel blockers 21.2 (9.8–33.4) Cardiac glycosides 35.7 (17.3–53.5) Diuretics 86.9 (64.2–96.4) IV inotropic agents 7.2 (0.5–19.5) Nitrates 32.1 (6.3–70.6) Spironolactone 20.5 (5.7–58.5) Eur Heart J 2003;24:
 ACE inhibitors (40–85.1) Angiotensin II receptor antagonists. 4.5 (1.9–14) Antithrombotic therapy (any) 77.6 (57.7–92.7) Aspirin (27.1–73.0) Beta-Blockers (10.0–65.8) Calcium channel blockers (9.8–33.4) Cardiac glycosides (17.3–53.5) Diuretics (64.2–96.4) IV inotropic agents. 7.2 (0.5–19.5) Nitrates (6.3–70.6) Spironolactone (5.7–58.5) Eur Heart J 2003;24:")
32
The EuroHeart Failure Survey programme - a survey on the quality of care among patients with heart failure in Europe Part 2: treatment Daily dosage of the principal diuretics, ACE inhibitors and beta-blockers used Diuretics (mgday–1) ACE inhibitors (mgday–1) Beta-blockers (mgday–1) Furosemide 86.4±75.2 Captopril 57.6±37.1 Metoprolol 74.9±43.3 Spironolactone 48.3±27.8 Enalapril 14.3±9.1 Atenolol 46.9±27.9 Toresamide 37.7±47.6 Lisinopril 12.3±7.8 Carvedilol 17.6±16.6 Amiloride 14.2±12.7 Ramipril 5.1±3 Bisoprolol 4.7±2.6 Perindopril 3.1±1 Eur Heart J 2003;24:
 ACE inhibitors (mgday–1) Beta-blockers (mgday–1) Furosemide. 86.4±75.2. Captopril. 57.6±37.1. Metoprolol. 74.9±43.3. Spironolactone. 48.3±27.8. Enalapril. 14.3±9.1. Atenolol. 46.9±27.9. Toresamide. 37.7±47.6. Lisinopril. 12.3±7.8. Carvedilol. 17.6±16.6. Amiloride. 14.2±12.7. Ramipril. 5.1±3. Bisoprolol. 4.7±2.6. Perindopril. 3.1±1. Eur Heart J 2003;24:")
33
The EuroHeart Failure Survey programme - a survey on the quality of care among patients with heart failure in Europe Part 2: treatment Eur Heart J 2003;24:

34
The EuroHeart Failure Survey programme - a survey on the quality of care among patients with heart failure in Europe Part 2: treatment Eur Heart J 2003;24:

35
The EuroHeart Failure Survey programme - a survey on the quality of care among patients with heart failure in Europe Part 2: treatment Beta-blockers Respiratory/pulmonary disease 0.35 (0.30 to 0.40) Speciality at admission (Cardiology vs GIM, for being Cardiology) 2.69 (2.37 to 3.31) IHD 2.63 (2.32 to 2.99) Age group (>70) 0.55 (0.49 to 0.61) Gender (being male) 1.16 (1.05 to 1.29) Factor Eur Heart J 2003;24:
 Speciality at admission (Cardiology vs GIM, for being Cardiology) 2.69 (2.37 to 3.31) IHD (2.32 to 2.99) Age group (>70) 0.55 (0.49 to 0.61) Gender (being male) 1.16 (1.05 to 1.29) Factor. Eur Heart J 2003;24:")
36
Was ist das Problem ?

37
Zwölf Arzneien in neunzehn Dosen
Hat die Medizin die betagten Menschen noch immer nicht auf der Rechnung ? Leitlinien stiften bisher mehr Verwirrung als klare Anweisungen für die behandelnden Ärzte FAZ, 12. Feb. 2008

38
Clinical Practice Guidelines and Quality of Care for Older Patients With Multiple Comorbid Diseases
Implications for Pay for Performance Cynthia M. Boyd, MD, MPH; Jonathan Darer, MD, MPH; Chad Boult, MD, MPH, MBA; Linda P. Fried, MD, MPH; Lisa Boult, MD, MPH, MA; Albert W. Wu, MD, MPH JAMA. 2005;294: ABSTRACT Context Clinical practice guidelines (CPGs) have been developed to improve the quality of health care for many chronic conditions. Pay-for-performance initiatives assess physician adherence to interventions that may reflect CPG recommendations. Objective To evaluate the applicability of CPGs to the care of older individuals with several comorbid diseases. Data Sources The National Health Interview Survey and a nationally representative sample of Medicare beneficiaries (to identify the most prevalent chronic diseases in this population); the National Guideline Clearinghouse (for locating evidence-based CPGs for each chronic disease). Study Selection Of the 15 most common chronic diseases, we selected hypertension, chronic heart failure, stable angina, atrial fibrillation, hypercholesterolemia, diabetes mellitus, osteoarthritis, chronic obstructive pulmonary disease, and osteoporosis, which are usually managed in primary care, choosing CPGs promulgated by national and international medical organizations for each. Data Extraction Two investigators independently assessed whether each CPG addressed older patients with multiple comorbid diseases, goals of treatment, interactions between recommendations, burden to patients and caregivers, patient preferences, life expectancy, and quality of life. Differences were resolved by consensus. For a hypothetical 79-year-old woman with chronic obstructive pulmonary disease, type 2 diabetes, osteoporosis, hypertension, and osteoarthritis, we aggregated the recommendations from the relevant CPGs. Data Synthesis Most CPGs did not modify or discuss the applicability of their recommendations for older patients with multiple comorbidities. Most also did not comment on burden, short- and long-term goals, and the quality of the underlying scientific evidence, nor give guidance for incorporating patient preferences into treatment plans. If the relevant CPGs were followed, the hypothetical patient would be prescribed 12 medications (costing her $406 per month) and a complicated nonpharmacological regimen. Adverse interactions between drugs and diseases could result. Conclusions This review suggests that adhering to current CPGs in caring for an older person with several comorbidities may have undesirable effects. Basing standards for quality of care and pay for performance on existing CPGs could lead to inappropriate judgment of the care provided to older individuals with complex comorbidities and could create perverse incentives that emphasize the wrong aspects of care for this population and diminish the quality of their care. Developing measures of the quality of the care needed by older patients with complex comorbidities is critical to improving their care. Boyd CM et al. JAMA 2005;294: ;
 have been developed to improve the quality of health care for many chronic conditions. Pay-for-performance initiatives assess physician adherence to interventions that may reflect CPG recommendations. Objective To evaluate the applicability of CPGs to the care of older individuals with several comorbid diseases. Data Sources The National Health Interview Survey and a nationally representative sample of Medicare beneficiaries (to identify the most prevalent chronic diseases in this population); the National Guideline Clearinghouse (for locating evidence-based CPGs for each chronic disease). Study Selection Of the 15 most common chronic diseases, we selected hypertension, chronic heart failure, stable angina, atrial fibrillation, hypercholesterolemia, diabetes mellitus, osteoarthritis, chronic obstructive pulmonary disease, and osteoporosis, which are usually managed in primary care, choosing CPGs promulgated by national and international medical organizations for each. Data Extraction Two investigators independently assessed whether each CPG addressed older patients with multiple comorbid diseases, goals of treatment, interactions between recommendations, burden to patients and caregivers, patient preferences, life expectancy, and quality of life. Differences were resolved by consensus. For a hypothetical 79-year-old woman with chronic obstructive pulmonary disease, type 2 diabetes, osteoporosis, hypertension, and osteoarthritis, we aggregated the recommendations from the relevant CPGs. Data Synthesis Most CPGs did not modify or discuss the applicability of their recommendations for older patients with multiple comorbidities. Most also did not comment on burden, short- and long-term goals, and the quality of the underlying scientific evidence, nor give guidance for incorporating patient preferences into treatment plans. If the relevant CPGs were followed, the hypothetical patient would be prescribed 12 medications (costing her $406 per month) and a complicated nonpharmacological regimen. Adverse interactions between drugs and diseases could result. Conclusions This review suggests that adhering to current CPGs in caring for an older person with several comorbidities may have undesirable effects. Basing standards for quality of care and pay for performance on existing CPGs could lead to inappropriate judgment of the care provided to older individuals with complex comorbidities and could create perverse incentives that emphasize the wrong aspects of care for this population and diminish the quality of their care. Developing measures of the quality of the care needed by older patients with complex comorbidities is critical to improving their care. Boyd CM et al. JAMA 2005;294: ;")
39
Clinical Practice Guidelines and Quality of Care for Older Patients With Multiple Comorbid Diseases
Boyd CM et al. JAMA 2005;294: ;

40
Clinical Practice Guidelines and Quality of Care for Older Patients With Multiple Comorbid Diseases
his review provides evidence that CPGs do not provide an appropriate, evidence-based foundation for assessing quality of care in older adults with several chronic diseases. Although CPGs provide detailed guidance for managing single diseases, they fail to address the needs of older patients with complex comorbid illness. While some recommend interventions for specific pairs of diseases, CPGs rarely address treatment of patients with 3 or more chronic diseases—a group that includes half of the population older than 65 years.1 When we developed a treatment plan for a hypothetical patient using a conservative regimen created in accordance with CPGs, she was treated with multiple medications with high complexity, with the attendant risks of medication errors, adverse drug events, drug interactions, and hospitalization.4, The recommended regimens may present the patient with an unsustainable treatment burden, making independent self-management and adherence difficult.12-13,50-51,61-63 It is evident that CPGs, designed largely by specialty-dominated committees for managing single diseases, provide clinicians little guidance about caring for older patients with multiple chronic diseases. The use of single-disease CPGs as a basis for evaluating the quality of care and determining physician reimbursement through pay-for-performance measures could create inappropriate incentives in the care of older adults with multiple diseases.7-8 Payment to physicians in pay-for-performance programs is frequently based in part on their meeting quality-of-care standards created for single diseases according to a calculated rate of adherence to the standard within an eligible population While these standards are not explicitly taken directly from CPGs, they are often derived from CPG recommendations. The Medicare Payment Advisory Commission recommended that Medicare adopt pay for performance for physician reimbursement.66 The Commission suggests a trial period during which physician reimbursement would be based on adoption of information technology measures, with feedback to individual physicians on performance on condition-specific claims-based process measures, followed by a "date certain" when condition-specific claims-based process measures would be included in physician pay for performance.66 Medicare initiatives and demonstrations incorporating pay for performance are becoming increasingly common.67 The CPGs are not designed for use in quality assessment, so transforming CPGs into performance standards and applying these standards to the care of older patients with complex comorbidity is problematic.8 These guidelines are recommendations based on varying levels of evidence and assume application of clinical judgment and patient preferences, both of which would be difficult to measure in a pay-for-performance scheme.15, 17-18,30, 33, Quality indicators must balance scientific evidence against what is practical and feasible to measure rather than what is a higher priority (eg, assessing yearly screening for retinopathy rather than aggressive blood pressure control in diabetics).56 Many indicators have upper age limits (eg, <75 years), thereby excluding a large percentage of Medicare beneficiaries and removing incentives to focus on these patients. Most indicators do not address burden of comorbid disease. While it would be feasible to omit "sick" patients from computations for reporting purposes, this would remove the pay-for-performance incentive for improving care for such patients.68-69 Assessing physicians on the basis of the care they provide for individual diseases obscures the complexity of treating real, and particularly older, patients with several chronic diseases. Patients in whom single-disease standards cannot or should not be attained, but who are eligible to be in the population base for a given standard may become "medical hot potatoes" if their physician receives lower pay-for-performance scores as a result.70 Current pay-for-performance initiatives can create financial incentives for physicians to focus on certain diseases and younger or healthier Medicare patients. These initiatives perpetuate the single-disease approach to care and fail to reward physicians for addressing the complex issues that confront patients with several chronic diseases. Standards that define quality of patient care regardless of a patient’s health status and preferences by placing emphasis on attaining high rates of adherence to CPGs rather than the more difficult task of weighing burden, risks, and benefits of complex therapies in shared decision making could ultimately undermine quality of care.68, 71 If quality assessment focuses on younger or healthier patients, there is additional risk that these problems will go unnoticed. Quality-of-care standards are needed for older individuals with several chronic diseases. Critical but currently unreimbursed processes of high-quality care for this population include care coordination, patient and caregiver education, empowerment for self-management, and shared decision making that incorporates individual preferences and circumstances. These processes should be incorporated into quality-of-care standards in pay-for-performance initiatives.49, 68, 72 Standards for developing CPGs note the importance of identifying the target population and incorporating quality of life and patient preferences to improve adherence of both physicians and patients.6, 43, 47, The CPGs we examined do not give explicit guidance on how to do this. Providing optimal care, as defined by several CPGs, for the patient with comorbid conditions quickly becomes difficult in terms of cost, medication complexity, and the magnitude of the task. Practicing physicians adjust CPG recommendations for individual patients, judging risks and reacting to patient preferences, but best practices for making these adjustments remain undefined.61, 75 Coexisting diseases may increase or decrease the benefit of an intervention for a target disease.49 Future CPGs that address how to incorporate quality of life and the risks, benefits, and burden of recommended treatments for older adults with comorbidity would be more useful than currently existing CPGs, but training physicians to use CPGs while incorporating these principles is also critical.8 The guidelines could address common comorbidities, but more obscure comorbidities would be difficult to address. Clinical practice guidelines addressing several combinations of comorbid diseases would be more unwieldy and based on scant evidence. To provide evidence for optimal care of older patients with several chronic diseases, future trials should include older patients with representative comorbidities and should investigate shared decision making among those patients, their caregivers, and physicians.76-77 A few noteworthy efforts address these issues. A recent CPG for older adults with diabetes discusses the quality of evidence and gives practical advice about geriatric syndromes and prioritizing care for older persons with several chronic diseases.78 The Assessing Care of Vulnerable Elders Project proposes quality-of-care markers for chronic diseases and geriatric syndromes in frail older adults and recognizes that goals of care and preferences affect definitions of quality.79 Patient-reported measures of quality of care address access, continuity, coordination, communication, and empowerment for patient and family involvement.80 Some pay-for-performance standards include provision of educational resources and measures of patient experience.64, 81 Our analysis has several limitations. First, we did not attempt to examine all CPGs. Instead, we selected CPGs generated by prominent professional organizations and published in widely read journals, which are likely to have a high impact on clinical practice. There may be less well-known CPGs that provide better guidance for the care of older adults with multiple chronic diseases. Second, in designing the treatment regimen for our hypothetical patient, we used our clinical judgment when the CPGs were not explicit in their recommendations—a task clinicians face daily. While other clinicians might arrive at slightly different regimens, we believe they would have similar complexity. For the present, widely used CPGs offer little guidance to clinicians caring for older patients with several chronic diseases. The use of CPGs as the basis for pay-for-performance initiatives that focus on specific treatments for single diseases may be particularly unsuited to the care of older individuals with multiple chronic diseases. Quality improvement and pay-for-performance initiatives within the Medicare system should be designed to improve the quality of care for older patients with multiple chronic diseases; a critical first step is research to define measures of the quality of care needed by this population, including care coordination, education, empowerment for self-management, and shared decision making based on the individual circumstances of older patients. Boyd CM et al. JAMA 2005;294: ;
.56 Many indicators have upper age limits (eg, <75 years), thereby excluding a large percentage of Medicare beneficiaries and removing incentives to focus on these patients. Most indicators do not address burden of comorbid disease. While it would be feasible to omit sick patients from computations for reporting purposes, this would remove the pay-for-performance incentive for improving care for such patients Assessing physicians on the basis of the care they provide for individual diseases obscures the complexity of treating real, and particularly older, patients with several chronic diseases. Patients in whom single-disease standards cannot or should not be attained, but who are eligible to be in the population base for a given standard may become medical hot potatoes if their physician receives lower pay-for-performance scores as a result.70 Current pay-for-performance initiatives can create financial incentives for physicians to focus on certain diseases and younger or healthier Medicare patients. These initiatives perpetuate the single-disease approach to care and fail to reward physicians for addressing the complex issues that confront patients with several chronic diseases. Standards that define quality of patient care regardless of a patient’s health status and preferences by placing emphasis on attaining high rates of adherence to CPGs rather than the more difficult task of weighing burden, risks, and benefits of complex therapies in shared decision making could ultimately undermine quality of care.68, 71 If quality assessment focuses on younger or healthier patients, there is additional risk that these problems will go unnoticed. Quality-of-care standards are needed for older individuals with several chronic diseases. Critical but currently unreimbursed processes of high-quality care for this population include care coordination, patient and caregiver education, empowerment for self-management, and shared decision making that incorporates individual preferences and circumstances. These processes should be incorporated into quality-of-care standards in pay-for-performance initiatives.49, 68, 72. Standards for developing CPGs note the importance of identifying the target population and incorporating quality of life and patient preferences to improve adherence of both physicians and patients.6, 43, 47, The CPGs we examined do not give explicit guidance on how to do this. Providing optimal care, as defined by several CPGs, for the patient with comorbid conditions quickly becomes difficult in terms of cost, medication complexity, and the magnitude of the task. Practicing physicians adjust CPG recommendations for individual patients, judging risks and reacting to patient preferences, but best practices for making these adjustments remain undefined.61, 75 Coexisting diseases may increase or decrease the benefit of an intervention for a target disease.49 Future CPGs that address how to incorporate quality of life and the risks, benefits, and burden of recommended treatments for older adults with comorbidity would be more useful than currently existing CPGs, but training physicians to use CPGs while incorporating these principles is also critical.8 The guidelines could address common comorbidities, but more obscure comorbidities would be difficult to address. Clinical practice guidelines addressing several combinations of comorbid diseases would be more unwieldy and based on scant evidence. To provide evidence for optimal care of older patients with several chronic diseases, future trials should include older patients with representative comorbidities and should investigate shared decision making among those patients, their caregivers, and physicians A few noteworthy efforts address these issues. A recent CPG for older adults with diabetes discusses the quality of evidence and gives practical advice about geriatric syndromes and prioritizing care for older persons with several chronic diseases.78 The Assessing Care of Vulnerable Elders Project proposes quality-of-care markers for chronic diseases and geriatric syndromes in frail older adults and recognizes that goals of care and preferences affect definitions of quality.79 Patient-reported measures of quality of care address access, continuity, coordination, communication, and empowerment for patient and family involvement.80 Some pay-for-performance standards include provision of educational resources and measures of patient experience.64, 81. Our analysis has several limitations. First, we did not attempt to examine all CPGs. Instead, we selected CPGs generated by prominent professional organizations and published in widely read journals, which are likely to have a high impact on clinical practice. There may be less well-known CPGs that provide better guidance for the care of older adults with multiple chronic diseases. Second, in designing the treatment regimen for our hypothetical patient, we used our clinical judgment when the CPGs were not explicit in their recommendations—a task clinicians face daily. While other clinicians might arrive at slightly different regimens, we believe they would have similar complexity. For the present, widely used CPGs offer little guidance to clinicians caring for older patients with several chronic diseases. The use of CPGs as the basis for pay-for-performance initiatives that focus on specific treatments for single diseases may be particularly unsuited to the care of older individuals with multiple chronic diseases. Quality improvement and pay-for-performance initiatives within the Medicare system should be designed to improve the quality of care for older patients with multiple chronic diseases; a critical first step is research to define measures of the quality of care needed by this population, including care coordination, education, empowerment for self-management, and shared decision making based on the individual circumstances of older patients. Boyd CM et al. JAMA 2005;294: ;")
41
Why Don't Physicians Follow Clinical Practice Guidelines
Why Don't Physicians Follow Clinical Practice Guidelines? A Framework for Improvement Leitlinie nicht bekannt (median) 1-84 (54.5)% 78% d Erhebungen >10% Inhalt nicht bekannt 0-89 (56.5)% 90% Nicht einverstanden 7-85% 95% Fachliche Interpretation Praktikabilität Übersimplifiziert Einschränkung der Therapiefreiheit Störung der Arzt-Patientenbeziehung Unglaubwürdigkeit der Autoren Fehlende Selbstwirksamkeitserwartung 1-65 (13)% 79% Eingeschränkte Ergebniserwartung 8-90 (26)% % Trägheit gegenüber Neuerungen (42)% % Leitlinien schwierig, mühsam, verwirrend 38% Widerstand von Patienten % Zeitmangel, Organisation, Kosten 80% Although counseling may increase a population's quit rate from 3% to only 5%,99 given smoking prevalence even this small change is enormously beneficial.100 However, since physicians see patients individually, they may not discern success at the population level. Overlooking population-level successes can negatively influence outcome expectancy and lead to nonadherence. Seventy-five percent of surveys reporting lack of outcome expectancy, such as those reporting lack of self-efficacy, involved preventive health counseling and education guidelines. Cabana MD et al. JAMA 1999;282:
 1-84 (54.5)% 78% d Erhebungen >10% Inhalt nicht bekannt 0-89 (56.5)% 90% Nicht einverstanden 7-85% 95% Fachliche Interpretation. Praktikabilität. Übersimplifiziert. Einschränkung der Therapiefreiheit. Störung der Arzt-Patientenbeziehung. Unglaubwürdigkeit der Autoren. Fehlende Selbstwirksamkeitserwartung 1-65 (13)% 79% Eingeschränkte Ergebniserwartung 8-90 (26)% 88% Trägheit gegenüber Neuerungen (42)% 100% Leitlinien schwierig, mühsam, verwirrend 38% Widerstand von Patienten 100% Zeitmangel, Organisation, Kosten 80% Although counseling may increase a population s quit rate from 3% to only 5%,99 given smoking prevalence even this small change is enormously beneficial.100 However, since physicians see patients individually, they may not discern success at the population level. Overlooking population-level successes can negatively influence outcome expectancy and lead to nonadherence. Seventy-five percent of surveys reporting lack of outcome expectancy, such as those reporting lack of self-efficacy, involved preventive health counseling and education guidelines. Cabana MD et al. JAMA 1999;282:")
42
Why Don't Physicians Follow Clinical Practice Guidelines
Why Don't Physicians Follow Clinical Practice Guidelines? A Framework for Improvement Sequence of Knowledge Attitudes Behavior Behavior change Barriers to Lack of familiarity Lack of agreement with External barriers Guideline Volume of information specific guidelines Patient factors Adherence Time needed to stay Interpretation of evidence Inability to reconcile informed Applicability to patient patient preferences - Guideline accessability Not cost beneficial with guideline re- - Lack of confidence in commendation guideline developer Guideline factors Lack of agreement with Guideline charac- guidelines in general teristics - „Too cookbook“ Contradictory guide- - Too rigid to apply lines - Biased synthesis - Challenge to autonomy Environmental factors - Not practical Lack of time - Lack of resources Lack of outcome expectancy Organisational con- Lack of self efficacy straints Lack of motivation Lack of reimbursement - Perceived increase in malpractice liability Lack of awareness - Volume of information - Time needed to stay informed - Guideline accessability Context Despite wide promulgation, clinical practice guidelines have had limited effect on changing physician behavior. Little is known about the process and factors involved in changing physician practices in response to guidelines. Objective To review barriers to physician adherence to clinical practice guidelines. Data Sources We searched the MEDLINE, Educational Resources Information Center (ERIC), and HealthSTAR databases (January 1966 to January 1998); bibliographies; textbooks on health behavior or public health; and references supplied by experts to find English-language article titles that describe barriers to guideline adherence. Study Selection Of 5658 articles initially identified, we selected 76 published studies describing at least 1 barrier to adherence to clinical practice guidelines, practice parameters, clinical policies, or national consensus statements. One investigator screened titles to identify candidate articles, then 2 investigators independently reviewed the texts to exclude articles that did not match the criteria. Differences were resolved by consensus with a third investigator. Data Extraction Two investigators organized barriers to adherence into a framework according to their effect on physician knowledge, attitudes, or behavior. This organization was validated by 3 additional investigators. Data Synthesis The 76 articles included 120 different surveys investigating 293 potential barriers to physician guideline adherence, including awareness (n = 46), familiarity (n = 31), agreement (n = 33), self-efficacy (n = 19), outcome expectancy (n = 8), ability to overcome the inertia of previous practice (n = 14), and absence of external barriers to perform recommendations (n = 34). The majority of surveys (70 [58%] of 120) examined only 1 type of barrier. Conclusions Studies on improving physician guideline adherence may not be generalizable, since barriers in one setting may not be present in another. Our review offers a differential diagnosis for why physicians do not follow practice guidelines, as well as a rational approach toward improving guideline adherence and a framework for future research. Cabana MD et al. JAMA 1999;282:
, and HealthSTAR databases (January 1966 to January 1998); bibliographies; textbooks on health behavior or public health; and references supplied by experts to find English-language article titles that describe barriers to guideline adherence. Study Selection Of 5658 articles initially identified, we selected 76 published studies describing at least 1 barrier to adherence to clinical practice guidelines, practice parameters, clinical policies, or national consensus statements. One investigator screened titles to identify candidate articles, then 2 investigators independently reviewed the texts to exclude articles that did not match the criteria. Differences were resolved by consensus with a third investigator. Data Extraction Two investigators organized barriers to adherence into a framework according to their effect on physician knowledge, attitudes, or behavior. This organization was validated by 3 additional investigators. Data Synthesis The 76 articles included 120 different surveys investigating 293 potential barriers to physician guideline adherence, including awareness (n = 46), familiarity (n = 31), agreement (n = 33), self-efficacy (n = 19), outcome expectancy (n = 8), ability to overcome the inertia of previous practice (n = 14), and absence of external barriers to perform recommendations (n = 34). The majority of surveys (70 [58%] of 120) examined only 1 type of barrier. Conclusions Studies on improving physician guideline adherence may not be generalizable, since barriers in one setting may not be present in another. Our review offers a differential diagnosis for why physicians do not follow practice guidelines, as well as a rational approach toward improving guideline adherence and a framework for future research. Cabana MD et al. JAMA 1999;282:")
43
Patient – Gefahren und Nachteile
Falsche Behandlung bei pauschaler und unkritischer Übernahme von Leitlinien Verunsicherung durch mißverständliche simplifizierte Formulierungen Kostensteigerung Fehlsteuerung von Resourcen Kostensteigerung: zB Festpreise, Sortis, Insulinanaloga Fehlsteuerung durch falsche Information: zB Screening, Vogelgrippe, Herzkatheter

44
Antibiotic Timing and Errors in Diagnosing Pneumonia
Background The percentage of patients with community-acquired pneumonia (CAP) whose time to first antibiotic dose (TFAD) is less than 4 hours of presentation to the emergency department (ED) has been made a core quality measure, and public reporting has been instituted. We asked whether these time pressures might also have negative effects on the accuracy of diagnosis of pneumonia. Methods We performed a retrospective review of adult admissions for CAP for 2 periods: group 1, when the core quality measure was a TFAD of less than 8 hours; and group 2, when the TFAD was lowered to less than 4 hours. We examined the accuracy of diagnosis of CAP by ED physicians. Results A total of 548 patients diagnosed as having CAP were studied (255 in group 1 and 293 in group 2). At admission, group 2 patients were 39.0% less likely to meet predefined diagnostic criteria for CAP than were group 1 patients (odds ratio, 0.61; 95% confidence interval, ) (P = .004). At discharge, there was agreement between the ED physician's diagnosis and the predefined criteria for CAP in 62.0% of group 1 and 53.9% of group 2 patients (P = .06) and between the ED physician's admitting diagnosis and that of the discharging physician in 74.5% of group 1 and 66.9% of group 2 patients (P = .05). The mean (SD) TFAD was similar in group 1 (167.0 [118.6] minutes) and group 2 (157.8 [96.3] minutes). Conclusion Reduction in the required TFAD from 8 to 4 hours seems to reduce the accuracy by which ED physicians diagnose pneumonia, while failing to reduce the actual TFAD achieved for patients. INTRODUCTION 8 hrs hrs Time to first antibiotic dose Welker JA et al. Arch Intern Med 2008;168:
 whose time to first antibiotic dose (TFAD) is less than 4 hours of presentation to the emergency department (ED) has been made a core quality measure, and public reporting has been instituted. We asked whether these time pressures might also have negative effects on the accuracy of diagnosis of pneumonia. Methods We performed a retrospective review of adult admissions for CAP for 2 periods: group 1, when the core quality measure was a TFAD of less than 8 hours; and group 2, when the TFAD was lowered to less than 4 hours. We examined the accuracy of diagnosis of CAP by ED physicians. Results A total of 548 patients diagnosed as having CAP were studied (255 in group 1 and 293 in group 2). At admission, group 2 patients were 39.0% less likely to meet predefined diagnostic criteria for CAP than were group 1 patients (odds ratio, 0.61; 95% confidence interval, ) (P = .004). At discharge, there was agreement between the ED physician s diagnosis and the predefined criteria for CAP in 62.0% of group 1 and 53.9% of group 2 patients (P = .06) and between the ED physician s admitting diagnosis and that of the discharging physician in 74.5% of group 1 and 66.9% of group 2 patients (P = .05). The mean (SD) TFAD was similar in group 1 (167.0 [118.6] minutes) and group 2 (157.8 [96.3] minutes). Conclusion Reduction in the required TFAD from 8 to 4 hours seems to reduce the accuracy by which ED physicians diagnose pneumonia, while failing to reduce the actual TFAD achieved for patients. INTRODUCTION. 8 hrs 4 hrs. Time to first antibiotic dose. Welker JA et al. Arch Intern Med 2008;168:")
45
Medizinische Leistungsträger: Gefahren und Nachteile
Qualitätsverlust durch falsche, irreführende, veraltete L. Fehlende Praktikabilität durch unrealistische, praxisferne Vorgaben Widersprüche verschiedener Fachgesellschaften Ausufernde Kosten und Bürokratie Unfaire Beurteilung durch Kostenträger, Behörden Irreführung durch ja/nein - Algorithmen bei komplexen Situationen, simplifiziert durch willkürliche Zahlen Quelle für Kunstfehleranschuldigungen Entzug von Fördergeldern Fehlsteuerung der Forschung --Kosten: Statine --zB QB AAI-Systeme, Verschlüsselung, Leitlinien falsch, unbedacht, Verschlüsselung irreführend, unvollkommen --zB Behandl dauer Monate, Screening alle 6 Monate) Ursache Widersprüche: weak evidence, andere Gesichtspunkte (Chir – Innere, Kanada – US, Resourcen, System, Politik, Werte, aber auch finanzoielle Interessen, Politischer Aktionismus zB Screening)
 Ursache Widersprüche: weak evidence, andere Gesichtspunkte (Chir – Innere, Kanada – US, Resourcen, System, Politik, Werte, aber auch finanzoielle Interessen, Politischer Aktionismus zB Screening)")
46
Öffentliches Gesundheitswesen: Nachteile und Gefahren
Verschwendung, Fehlsteuerung von Geldern Ausufernde Bürokratie Vermehrte Kosten Transparenz: besser zu kontrollieren, auch der Geldströme Liegedauer, Prozeduren, amb Operationen, Doppeldiagnostik, Rationalisierung

47
Lösungsansätze

48
Toward Improved Implementation of Evidence-based Clinical Algorithms: Clinical Practice Guidelines, Clinical Decision Rules, and Clinical Pathways KT = knowledge translation EBCA = EB clinical algorithm Figure 1. Social, cognitive, and motivational factors appear to each serve a role to support organizational factors that enable efficient knowledge translation. KT = knowledge translation; EBCA = evidence-based clinical algorithm. Aknowledge translation (KT) gap exists between the care patients receive and the evidence available to guide the delivery of that care. Thirty percent to 45% of patients do not receive care that is supported by current scientific evidence, and 20%–25% of the care provided may actually be unneeded or even harmful.1Clinical pathways, clinical practice guidelines, and clinical decision rules, which hereafter will be referred to as evidence-based clinical algorithms (EBCAs), are tools that show promise to ameliorate these problems. EBCAs codify available evidence into specific rules and action plans. These "prepackaged" action plans facilitate the delivery of appropriate, efficient, evidence-based care to the bedside of patients suffering the illnesses or injuries for which these EBCAs have been developed. Human factors engineers would tell clinicians that EBCAs can augment clinicians' ability to deliver complicated, multistep treatments consistently, without omitting important steps, while freeing their cognitive abilities and intellect to focus on the situational, contextual, intrapersonal, and intuitive nature of health care delivery. Work is under way to model medical decision-making processes using an aviation and aerospace error management model, but such efforts are still in their infancy Gaddis GM et al. Acad Emerg Med 2007;14:
 gap exists between the care patients receive and the evidence available to guide the delivery of that care. Thirty percent to 45% of patients do not receive care that is supported by current scientific evidence, and 20%–25% of the care provided may actually be unneeded or even harmful.1Clinical pathways, clinical practice guidelines, and clinical decision rules, which hereafter will be referred to as evidence-based clinical algorithms (EBCAs), are tools that show promise to ameliorate these problems. EBCAs codify available evidence into specific rules and action plans. These prepackaged action plans facilitate the delivery of appropriate, efficient, evidence-based care to the bedside of patients suffering the illnesses or injuries for which these EBCAs have been developed. Human factors engineers would tell clinicians that EBCAs can augment clinicians ability to deliver complicated, multistep treatments consistently, without omitting important steps, while freeing their cognitive abilities and intellect to focus on the situational, contextual, intrapersonal, and intuitive nature of health care delivery. Work is under way to model medical decision-making processes using an aviation and aerospace error management model, but such efforts are still in their infancy. Gaddis GM et al. Acad Emerg Med 2007;14:")
49
Are Guidelines Following Guidelines
Are Guidelines Following Guidelines? The Methodological Quality of Clinical Practice Guidelines in the Peer-Reviewed Medical Literature Figure 1. Distribution of the Mean Number of Methodological Standards Satisfied by Guidelines Context Practice guidelines play an important role in medicine. Methodological principles have been formulated to guide their development. Objective To determine whether practice guidelines in peer-reviewed medical literature adhered to established methodological standards for practice guidelines. Design Structured review of guidelines published from 1985 through June 1997 identified by a MEDLINE search. Main Outcome Measures Mean number of standards met based on a 25-item instrument and frequency of adherence. Results We evaluated 279 guidelines, published from 1985 through June 1997, produced by 69 different developers. Mean overall adherence to standards by each guideline was 43.1% (10.77/25). Mean (SD) adherence to methodological standards on guideline development and format was 51.1% (25.3%); on identification and summary of evidence, 33.6% (29.9%); and on the formulation of recommendations, 46% (45%). Mean adherence to standards by each guideline improved from 36.9% (9.2/25) in 1985 to 50.4% (12.6/25) in 1997 (P<.001). However, there was little improvement over time in adherence to standards on identification and summary of evidence from 34.6% prior to 1990 to 36.1% after 1995 (P=.11). There was no difference in the mean number of standards satisfied by guidelines produced by subspecialty medical societies, general medical societies, or government agencies (P=.55). Guideline length was positively correlated with adherence to methodological standards (P=.001). Conclusion Guidelines published in the peer-reviewed medical literature during the past decade do not adhere well to established methodological standards. While all areas of guideline development need improvement, greatest improvement is needed in the identification, evaluation, and synthesis of the scientific evidence. Shaneyfelt TM et al. JAMA 1999;281:
. Mean (SD) adherence to methodological standards on guideline development and format was 51.1% (25.3%); on identification and summary of evidence, 33.6% (29.9%); and on the formulation of recommendations, 46% (45%). Mean adherence to standards by each guideline improved from 36.9% (9.2/25) in 1985 to 50.4% (12.6/25) in 1997 (P<.001). However, there was little improvement over time in adherence to standards on identification and summary of evidence from 34.6% prior to 1990 to 36.1% after 1995 (P=.11). There was no difference in the mean number of standards satisfied by guidelines produced by subspecialty medical societies, general medical societies, or government agencies (P=.55). Guideline length was positively correlated with adherence to methodological standards (P=.001). Conclusion Guidelines published in the peer-reviewed medical literature during the past decade do not adhere well to established methodological standards. While all areas of guideline development need improvement, greatest improvement is needed in the identification, evaluation, and synthesis of the scientific evidence. Shaneyfelt TM et al. JAMA 1999;281:")
50
Are Guidelines Following Guidelines
Are Guidelines Following Guidelines? The Methodological Quality of Clinical Practice Guidelines in the Peer-Reviewed Medical Literature Figure 3. Adherence to Methodological Standards Over TimeAsterisk indicates P<.01 for trend across all years; dagger indicates P=.11 for trend across all years. Error bars indicate SDs. Shaneyfelt TM et al. JAMA 1999;281:

51
Are Guidelines Following Guidelines
Are Guidelines Following Guidelines? The Methodological Quality of Clinical Practice Guidelines in the Peer-Reviewed Medical Literature Unzureichende Beschreibung von wissenschaftlicher „Evidenz“ Kostenfaktoren Patientenpräferenzen Standards für Leitlinien müssen beachtet werden ! This guideline describes the dearth of literature, acknowledges the limitations of opinion-based directives, then issues pragmatic recommendations based on both appropriateness scores and consensus ratings. Shaneyfelt TM et al. JAMA 1999;281:

52
Disseminating Innovations in Health Care
igure 1. Cumulative Number of Adopters of Hybrid Seed Corn in 2 Iowa Communities. This Iowa study has been replicated for numerous other innovations. Its authors found that the curve of adoption of the innovation among 300 farmers had an S shape, with an early slow phase affecting a very few farmers, a rapid middle phase with wide spread, and a slow third phase with incomplete penetration in the end. It looks much like the epidemic curve of a contagious disease. Saatgut-kreuzung Berwick DM. JAMA 2003;289:

53
Disseminating Innovations in Health Care
100 Cumulative percentage of adoption igure 1. Cumulative Number of Adopters of Hybrid Seed Corn in 2 Iowa Communities. This Iowa study has been replicated for numerous other innovations. Its authors found that the curve of adoption of the innovation among 300 farmers had an S shape, with an early slow phase affecting a very few farmers, a rapid middle phase with wide spread, and a slow third phase with incomplete penetration in the end. It looks much like the epidemic curve of a contagious disease. Saatgut-kreuzung time Berwick DM. JAMA 2003;289:

54
Disseminating Innovations in Health Care
100 Cumulative percentage of adoption igure 1. Cumulative Number of Adopters of Hybrid Seed Corn in 2 Iowa Communities. This Iowa study has been replicated for numerous other innovations. Its authors found that the curve of adoption of the innovation among 300 farmers had an S shape, with an early slow phase affecting a very few farmers, a rapid middle phase with wide spread, and a slow third phase with incomplete penetration in the end. It looks much like the epidemic curve of a contagious disease. Saatgut-kreuzung 20 time Berwick DM. JAMA 2003;289:

55
Disseminating Innovations in Health Care
igure 2. Adopter Categorization on the Basis of Innovativeness The fastest adopting group (by definition, 2 SDs faster than the mean rate of adoption, and therefore, by definition, about 2.5% of those involved) are called "innovators." They are distinguished from the rest of the population by their venturesomeness, tolerance of risk, fascination with novelty, and willingness to leave the village to learn. Rogers calls them "cosmopolite."21(p299) They belong to cliques that transcend geographical boundaries, and they invest energy in those remote connections. Innovators who were studied in traditional Colombian villages left on trips to cities about 30 times a year, while the average resident left 0.3 times a year.21(p274) Innovators tend to be wealthier than average or otherwise able to accept the risks and costs inherent in innovating. Locally, socially, they tend to be a little disconnected. They are not opinion leaders; in fact, they may be thought of as weird or incautious. In health care, physician-innovators may be thought of as mavericks or may appear to be heavily invested personally in a specialized topic. The next group, called "early adopters," (by definition between 1 and 2 SDs quicker to adopt than the average, and therefore about 13% of individuals) are different from innovators. They are opinion leaders; they are locally well-connected socially, and they do not tend to search quite so widely as the innovators. They do, however, speak with innovators and with each other. They cross-pollinate, and they select ideas that they would like to try out. They have the resources and the risk tolerance to try new things. Such people are generally testing several innovations at once and can report on them if asked. They are self-conscious experimenters. Most crucially to the dynamics of spread, early adopters are watched. In health care settings, they are probably often chosen as elected leaders or representatives of clinical group, and they are the likeliest targets of pharmaceutical company detailing. Individuals who watch the early adopters, the next third of the distribution, are the "early majority." Whereas the early adopters maintain bridges to the outside through innovators by traveling, the early majority are quite local in their perspectives. They learn mainly from people they know well, and they rely on personal familiarity, more than on science or theory, before they decide to test a change. They are more risk-averse than early adopters. Those in the early majority are readier to hear about innovations relevant to current, local problems than general background improvements. Dairy farmers are more ready to accept innovations in dairy farming than in general animal care. Physicians in the early majority are readier to try those innovations that meet their immediate needs than those that are simply interesting ideas. The next group, another third of the population, is even more conservative: the "late majority." While the early majority look to the early adopters for signals about what is safe to try, the late majority look to the early majority. They will adopt an innovation when it appears to be the new status quo (for physicians, the standard of practice), not before. They watch for local proof; they do not find remote, cosmopolite sources of knowledge to be either trustworthy or particularly interesting. Members of the final group are sometimes called "laggards": the 16% of the individuals for whom, in Rogers' term, "the point of reference is the past."21(p265) The term "laggards" probably misstates this group's value and wisdom. They should perhaps be called traditionalists, sea anchors, or archivists, to emphasize that they are often making choices that are wise and useful to the community or organization. They are the physicians who swear by the tried and true. The curve that describes the dissemination of innovation has a tipping point, after which it becomes difficult to stop a change from spreading further. Changes appear to acquire their own momentum somewhere on the ascending portion of the adoption curve, often between 15% and 20% adoption.21(p259) This empirical finding makes theoretical sense in view of the social dynamics in the population model of adoption. Once innovators and early adopters have embraced a change, the model asserts that the early majority will follow their lead if they can interact with them, and, once those in the early majority have done so, the late majority will discover that the majority has changed direction and will feel comfortable changing, too. This dynamic implies that successful diffusion depends more on how an organization or social system deals with its innovators, early adopters, and the interface between early adopters and the early majority than with any other groups or phases. Berwick DM. JAMA 2003;289:
 are called innovators. They are distinguished from the rest of the population by their venturesomeness, tolerance of risk, fascination with novelty, and willingness to leave the village to learn. Rogers calls them cosmopolite. 21(p299) They belong to cliques that transcend geographical boundaries, and they invest energy in those remote connections. Innovators who were studied in traditional Colombian villages left on trips to cities about 30 times a year, while the average resident left 0.3 times a year.21(p274) Innovators tend to be wealthier than average or otherwise able to accept the risks and costs inherent in innovating. Locally, socially, they tend to be a little disconnected. They are not opinion leaders; in fact, they may be thought of as weird or incautious. In health care, physician-innovators may be thought of as mavericks or may appear to be heavily invested personally in a specialized topic. The next group, called early adopters, (by definition between 1 and 2 SDs quicker to adopt than the average, and therefore about 13% of individuals) are different from innovators. They are opinion leaders; they are locally well-connected socially, and they do not tend to search quite so widely as the innovators. They do, however, speak with innovators and with each other. They cross-pollinate, and they select ideas that they would like to try out. They have the resources and the risk tolerance to try new things. Such people are generally testing several innovations at once and can report on them if asked. They are self-conscious experimenters. Most crucially to the dynamics of spread, early adopters are watched. In health care settings, they are probably often chosen as elected leaders or representatives of clinical group, and they are the likeliest targets of pharmaceutical company detailing. Individuals who watch the early adopters, the next third of the distribution, are the early majority. Whereas the early adopters maintain bridges to the outside through innovators by traveling, the early majority are quite local in their perspectives. They learn mainly from people they know well, and they rely on personal familiarity, more than on science or theory, before they decide to test a change. They are more risk-averse than early adopters. Those in the early majority are readier to hear about innovations relevant to current, local problems than general background improvements. Dairy farmers are more ready to accept innovations in dairy farming than in general animal care. Physicians in the early majority are readier to try those innovations that meet their immediate needs than those that are simply interesting ideas. The next group, another third of the population, is even more conservative: the late majority. While the early majority look to the early adopters for signals about what is safe to try, the late majority look to the early majority. They will adopt an innovation when it appears to be the new status quo (for physicians, the standard of practice), not before. They watch for local proof; they do not find remote, cosmopolite sources of knowledge to be either trustworthy or particularly interesting. Members of the final group are sometimes called laggards : the 16% of the individuals for whom, in Rogers term, the point of reference is the past. 21(p265) The term laggards probably misstates this group s value and wisdom. They should perhaps be called traditionalists, sea anchors, or archivists, to emphasize that they are often making choices that are wise and useful to the community or organization. They are the physicians who swear by the tried and true. The curve that describes the dissemination of innovation has a tipping point, after which it becomes difficult to stop a change from spreading further. Changes appear to acquire their own momentum somewhere on the ascending portion of the adoption curve, often between 15% and 20% adoption.21(p259) This empirical finding makes theoretical sense in view of the social dynamics in the population model of adoption. Once innovators and early adopters have embraced a change, the model asserts that the early majority will follow their lead if they can interact with them, and, once those in the early majority have done so, the late majority will discover that the majority has changed direction and will feel comfortable changing, too. This dynamic implies that successful diffusion depends more on how an organization or social system deals with its innovators, early adopters, and the interface between early adopters and the early majority than with any other groups or phases. Berwick DM. JAMA 2003;289:")
56
Diffusion of innovations
FIG 1 - Diffusion of innovations. Speed of diffusion may vary, as shown by innovations I, II, and III. Modified from Rogers

57
AWMF Implementierung: Interventionen zur Unterstützung der Verhaltensänderung Konsistenter Effekt Variabler Effekt Wenig / kein Effekt Besuche vor Ort (educational outreach visit) Audit und feedback Disseminierung von Informationen Erinnerungshilfen (manuell/elektronisch) Einbindung lokaler Meinungsführer Passive Edukation (z.B. Vorträge) Interaktive Edukation (Qualitätszirkel) Lokale Konsensusprozesse Kombinierte Strategie (multifaceted interventions) Patientenzentrierte Intervention Gross et al.: Optimal methods for guideline implementation. Med Care 39:85-92 (2001) Bero et al.: Closing the gap between research and practice. BMJ 314: (1998)
 Audit und feedback. Disseminierung. von Informationen. Erinnerungshilfen. (manuell/elektronisch) Einbindung lokaler. Meinungsführer. Passive Edukation. (z.B. Vorträge) Interaktive Edukation. (Qualitätszirkel) Lokale. Konsensusprozesse. Kombinierte Strategie. (multifaceted interventions) Patientenzentrierte. Intervention. Gross et al.: Optimal methods for guideline implementation. Med Care 39:85-92 (2001) Bero et al.: Closing the gap between research and practice. BMJ 314: (1998)")
58
LaBresh KA et al. Arch Intern Med 2008; 168:411-417
Hospital Treatment of Patients With Ischemic Stroke or Transient Ischemic Attack Using the "Get With The Guidelines" Program Background Adherence to evidence-based interventions for hospitalized patients who have experienced a stroke is suboptimal. We examined the association of process improvement and Internet-based data collection and decision support with stroke care. Methods A 1-year intervention study to assess performance measure adherence in hospitals using the "Get With The Guidelines–Stroke" program. The program included 18 410 patients with ischemic stroke or transient ischemic attack admitted to 99 volunteer community and teaching hospitals. Data from eligible patients in the preintervention baseline period were compared with data from 4 subsequent quarters for 12 acute care or secondary prevention measures and an all-or-none measure of care based on 7 prespecified measures. Results Significant improvements from baseline to the fourth quarter were seen in 11 of 13 measures: use of thrombolytic medications for patients with ischemic stroke presenting within 2 hours of onset, 23.5% vs 40.8% (P < .001); early use of antithrombotic medications, 88.2% vs 95.2% (P < .001); antithrombotic medications prescribed at discharge, 91.0% vs 97.9% (P < .001); anticoagulation agents for atrial fibrillation, 81.4% vs 96.5% (P < .001); smoking cessation counseling, 38.3% vs 54.5% (P < .001); lipid treatment for low-density lipoprotein levels 100 mg/dL or greater, 58.7% vs 77.0% (P < .001); diabetes mellitus treatment, 48.5% vs 83.5% (P = .001); and weight reduction counseling 32.5% vs 43.4% (P < .001). The all-or-none measure increased from 50.2% to 58.0% (P < .001). Complications from thrombolytic medications and prophylaxis for deep venous thrombosis did not change. Conclusion Statistically and clinically significant improvement in 11of 13 quality improvement measures for the treatment of patients hospitalized for cerebrovascular disease was seen in hospitals participating in the Get With The Guidelines program. LaBresh KA et al. Arch Intern Med 2008; 168:
; early use of antithrombotic medications, 88.2% vs 95.2% (P < .001); antithrombotic medications prescribed at discharge, 91.0% vs 97.9% (P < .001); anticoagulation agents for atrial fibrillation, 81.4% vs 96.5% (P < .001); smoking cessation counseling, 38.3% vs 54.5% (P < .001); lipid treatment for low-density lipoprotein levels 100 mg/dL or greater, 58.7% vs 77.0% (P < .001); diabetes mellitus treatment, 48.5% vs 83.5% (P = .001); and weight reduction counseling 32.5% vs 43.4% (P < .001). The all-or-none measure increased from 50.2% to 58.0% (P < .001). Complications from thrombolytic medications and prophylaxis for deep venous thrombosis did not change. Conclusion Statistically and clinically significant improvement in 11of 13 quality improvement measures for the treatment of patients hospitalized for cerebrovascular disease was seen in hospitals participating in the Get With The Guidelines program. LaBresh KA et al. Arch Intern Med 2008; 168:")
59
Improving Guideline Adherence: Randomized Trial Evaluating Strategies to Increase ß-Blocker Use in Heart Failure Background— The dissemination of clinical practice guidelines often has not been accompanied by desired improvements in guideline adherence. This study evaluated interventions for implementing a new practice guideline advocating the use of ß-blockers for heart failure patients. Methods and Results— This was a randomized controlled trial involving heart failure patients (n=169) with an ejection fraction ≤45% and no contraindications to ß-blockers. Patients’ primary providers were randomized in a stratified design to 1 of 3 interventions: (1) control: provider education; (2) provider and patient notification: computerized provider reminders and patient letters advocating ß-blockers; and (3) nurse facilitator: supervised nurse to initiate and titrate ß-blockers. The primary outcome, the proportion of patients who were initiated or uptitrated and maintained on ß-blockers, analyzed by intention to treat, was achieved in 67% (36 of 54) of patients in the nurse facilitator group compared with 16% (10 of 64) in the provider/patient notification and 27% (14 of 51) in the control groups (P<0.001 for the comparisons between the nurse facilitator group and both other groups). The proportion of patients on target ß-blocker doses at the study end (median follow-up, 12 months) was also highest in the nurse facilitator group (43%) compared with the control (10%) and provider/patient notification groups (2%) (P<0.001). There were no differences in adverse events among groups. Conclusions— The use of a nurse facilitator was a successful approach for implementing a ß-blocker guideline in heart failure patients. The use of provider education, clinical reminders, and patient education was of limited value in this setting. Ansari M et al. Circulation 2003;107:2799
 with an ejection fraction ≤45% and no contraindications to ß-blockers. Patients’ primary providers were randomized in a stratified design to 1 of 3 interventions: (1) control: provider education; (2) provider and patient notification: computerized provider reminders and patient letters advocating ß-blockers; and (3) nurse facilitator: supervised nurse to initiate and titrate ß-blockers. The primary outcome, the proportion of patients who were initiated or uptitrated and maintained on ß-blockers, analyzed by intention to treat, was achieved in 67% (36 of 54) of patients in the nurse facilitator group compared with 16% (10 of 64) in the provider/patient notification and 27% (14 of 51) in the control groups (P<0.001 for the comparisons between the nurse facilitator group and both other groups). The proportion of patients on target ß-blocker doses at the study end (median follow-up, 12 months) was also highest in the nurse facilitator group (43%) compared with the control (10%) and provider/patient notification groups (2%) (P<0.001). There were no differences in adverse events among groups. Conclusions— The use of a nurse facilitator was a successful approach for implementing a ß-blocker guideline in heart failure patients. The use of provider education, clinical reminders, and patient education was of limited value in this setting. Ansari M et al. Circulation 2003;107:2799.")
60
Improving Guideline Adherence A Randomized Trial Evaluating Strategies to Increase ß-Blocker Use in Heart Failure Ansari M et al. Circulation 2003;107:2799

61
Häusliche Intervention bei chronischer Herzinsuffizienz
Standardbehandlung (n=148) Häusliche Intervention (n=149) Stewart S, Horowitz JD. Circulation 2002;105:
 Häusliche Intervention (n=149) Stewart S, Horowitz JD. Circulation 2002;105:")
62
Häusliche Intervention bei chronischer Herzinsuffizienz
Nurse entscheidend, beste Ergebnisse Adelaide, Australien, intervention: ein Kontrollbesuch zu Hause mit entsprechender Überwachung u AUFKLÄRUNG; nurse, danach tel f-up: nurse vermittelt auch link zu Dr/Klinik im Falle der Verschlechterung Mittl Alter 75, zusätzl COPD 40%, DM 30%, Hypertonie 60%, post MI 50%, ß-Bl 20%, ACEI 75%, Dig 65%, AF 30% Zeigt Ausmaß des Effektes: mittleres Überleben um sage und schreibe 18 Monate verlängert !! Stewart S, Horowitz JD. Circulation 2002;105:

63
Chronische Herzinsuffizienz am Knappschaftskrankenhaus Sulzbach
Stationäre Patienten mit chronischer Herzinsuffizienz Optimale Therapie, umfassende Information und Schulung (Arzt, Pflege, physikalische Therapie, Diätberatung) vor Entlassung Hausbesuche und Telefonkontakte durch speziell ausgebildete Pflegefachkräfte: ua Titration von BB und ACEI zu in Leitlinien festgelegten Zieldosen Koordination und Rückkopplung mit Hausarzt und Klinik Dokumentation, wissenschaftliche Auswertung
 vor Entlassung. Hausbesuche und Telefonkontakte durch speziell ausgebildete Pflegefachkräfte: ua Titration von BB und ACEI zu in Leitlinien festgelegten Zieldosen. Koordination und Rückkopplung mit Hausarzt und Klinik. Dokumentation, wissenschaftliche Auswertung.")
64
prosper CHI-Programm Knappschaftskrankenhaus Sulzbach
101 2004 2005 2006 2007
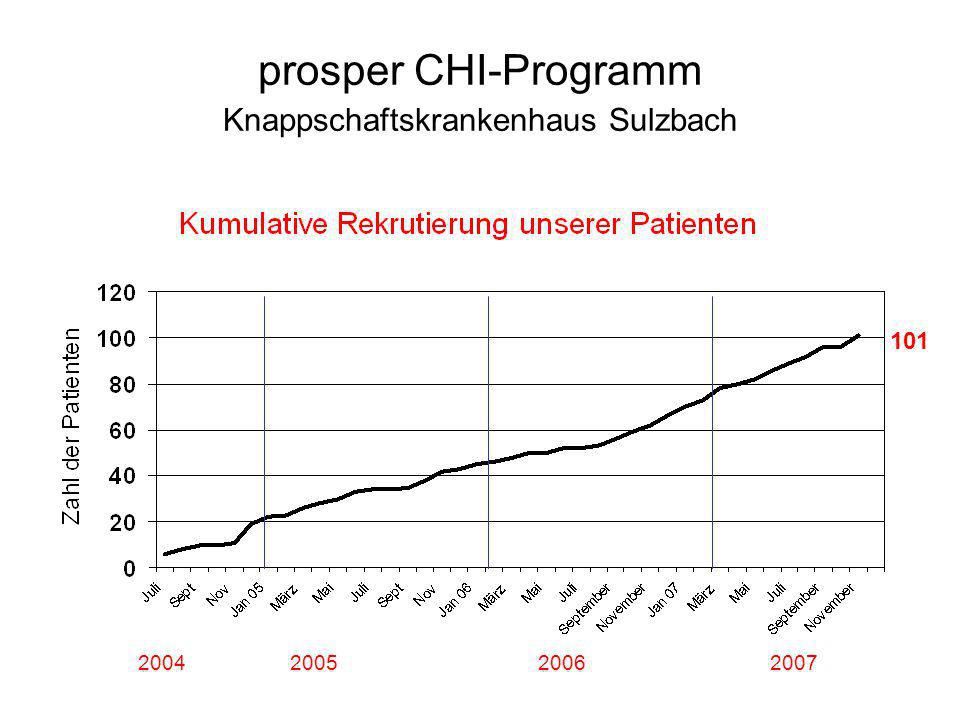
65
CHI-Programm, Stand November 2007
>800 Kontakte (1-29, m=10/Pt)
")
66
AHA, Orlando, Nov 2007

70
Blutdrucksenkung und Risikoreduktion tödlicher Ereignisse: KHK und Schlaganfall
Meta-Analyse aus 61 prospektiven Studien 1 Million Patienten 12.7 Million Patienten-Jahre 7% Reduktion der KHK-Mortalität Senkung des SBD um 2 mmHg Zusammenfassung: BD-Senkung ist wichtig; auch minimale Senkung zeigt Wirkung. Am beeindruckendsten sind vielleicht die praktischen Auswirkungen dieser Daten: sogar eine geringfügige Verringerung des mittleren systolischen BD von 2 mmHg ist mit einer bedeutenden absoluten Senkung der vorzeitigen Todesfälle und des Schlaganfallrisikos verbunden.1 Wie oben gezeigt, kann ein um 2 mmHg niedrigerer mittlerer systolischer BD zu einer 7%igen Reduktion des Risikos einer koronaren Herzerkrankung (KHK) und zu einer 10%igen Reduktion der Schlaganfallmortalität führen.1 Daten aus einer Metaanalyse von 61 prospektiven Beobachtungsstudien liefern aussagekräftige Nachweise, dass der BD im mittleren und höheren Alter in starker und direkter Verbindung mit der Sterblichkeit durch Gefäßerkrankungen steht.1 Beispielsweise ist ein um 10 mmHg niedrigerer systolischer BD langfristig mit einem um 40% geringeren Risiko der Schlaganfallmortalität und einem um 30% geringeren Risiko der Mortalität durch KHK oder aus anderen vaskulären Gründen verbunden.1 Innerhalb jedes Lebensjahrzehnts zwischen 40 und 89 Jahren verhält sich der proportionale Unterschied im Risiko eines Gefäßtods zum gegebenen absoluten Unterschied im mittleren BD annähernd äquivalent bis hinunter zu mindestens 115 mmHg für systolische BD und 75 mmHg für diastolischen BD (unterhalb dieser Werte liegen wenige Daten vor). Bei allen Gruppen im mittleren und höheren Alter ließ sich keine J-Kurve nachweisen.1 Es waren Studien einbezogen, bei denen zum Ausgangszeitpunkt Daten über Blutdruck, Cholesterinwerte, Geburtsdatum (oder Alter) und Geschlecht dokumentiert und eine Todesursache und ein Todeszeitpunkt von den Prüfern aufgezeichnet worden waren. 33 der Studien wurden in Europa durchgeführt (z. B. British Regional Heart Study, Scottish Heart Health Study, Tromsö-Studie, mit Bewertung des Zusammenhangs zwischen Blutdruck und Serumlipidwerten), 18 in Nordamerika oder Australien (z. B. Atherosclerosis Risk in Communities Study, Minnesota Heart Health Program) und 10 in China oder Japan (z. B. die Studie Seven Cities China zur Schlaganfallprävention).1 10% Reduktion der Schlaganfall-Mortalität SBD, systolischer Blutdruck. Lewington S et al. Lancet. 2002;360: Literatur Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:
 und zu einer 10%igen Reduktion der Schlaganfallmortalität führen.1. Daten aus einer Metaanalyse von 61 prospektiven Beobachtungsstudien liefern aussagekräftige Nachweise, dass der BD im mittleren und höheren Alter in starker und direkter Verbindung mit der Sterblichkeit durch Gefäßerkrankungen steht.1 Beispielsweise ist ein um 10 mmHg niedrigerer systolischer BD langfristig mit einem um 40% geringeren Risiko der Schlaganfallmortalität und einem um 30% geringeren Risiko der Mortalität durch KHK oder aus anderen vaskulären Gründen verbunden.1. Innerhalb jedes Lebensjahrzehnts zwischen 40 und 89 Jahren verhält sich der proportionale Unterschied im Risiko eines Gefäßtods zum gegebenen absoluten Unterschied im mittleren BD annähernd äquivalent bis hinunter zu mindestens 115 mmHg für systolische BD und 75 mmHg für diastolischen BD (unterhalb dieser Werte liegen wenige Daten vor). Bei allen Gruppen im mittleren und höheren Alter ließ sich keine J-Kurve nachweisen.1. Es waren Studien einbezogen, bei denen zum Ausgangszeitpunkt Daten über Blutdruck, Cholesterinwerte, Geburtsdatum (oder Alter) und Geschlecht dokumentiert und eine Todesursache und ein Todeszeitpunkt von den Prüfern aufgezeichnet worden waren. 33 der Studien wurden in Europa durchgeführt (z. B. British Regional Heart Study, Scottish Heart Health Study, Tromsö-Studie, mit Bewertung des Zusammenhangs zwischen Blutdruck und Serumlipidwerten), 18 in Nordamerika oder Australien (z. B. Atherosclerosis Risk in Communities Study, Minnesota Heart Health Program) und 10 in China oder Japan (z. B. die Studie Seven Cities China zur Schlaganfallprävention).1. 10% Reduktion der Schlaganfall-Mortalität. SBD, systolischer Blutdruck. Lewington S et al. Lancet. 2002;360: Literatur. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:")
71
- das Modell von Veränderung -
AMWF Konzeptrahmen für Implementierung von Leitlinien - das Modell von Veränderung - Erzeuge Rückkopplung Veränderung Druck für Veränderung Absicht zur Veränderung Identifiziere als Wirksame Alternative Schaffe Liefere Entwickle zusätzliche Personelle Unterstützung Eigene Geschicklichkeiten Unterstützende Infrastruktur Gustafson: Systems to support Health Policy Analysis: Theory, Models, and Uses, p. 45 (1992)
")
72
Gaddis GM et al. Acad Emerg Med 2007;14:1015-1022
Toward Improved Implementation of Evidence-based Clinical Algorithms: Clinical Practice Guidelines, Clinical Decision Rules, and Clinical Pathways Figure 3. The seven-step path from awareness to adherence (Befolgung), as conceptualized by Glasziou and Haynes.30 Steps 1–3 (aware, accepted, and applicable) indicate information that is eligible to be translated to the patient. This idea is captured by the concept of "bedside EBM." Clinicians must be able to recognize and accept the opportunity to deliver evidence-based care. Steps 3–5 (applicable, able, and acted on) encompass steps regarding whether evidence is usable and which clinical quality improvement initiatives can be monitored. Steps 6 and 7 (agreed to and adhered to) complete the implementation of an EBCA. Reproduced from Glasziou and Haynes30 with permission. EBM = evidence-based medicine; CATs = critical appraisal templates; EBCA = evidence-based clinical algorithms. However, implementation of EBCAs involves a team effort, and that team is not composed strictly of EPs. When EBCAs involve follow-up care of a physician from another specialty, implementation may be derailed if that follow-up physician is unaware of the EBCA. For example, an orthopedist ignorant of the OARs may react with disdain (which can cause patients to question the quality of their emergency department care) when no ankle film has been obtained for patients for whom the OARs determine no need for radiography. Nurses, who generally perceive themselves as patient advocates and educators, probably need to be both aware of and supportive of EBCAs if clinical implementation of EBCAs is to succeed. If nurses or allied health personnel, in conversations with patients, cast doubt on the validity or appropriateness of EBCAs, patient compliance and acceptance of these EBCAs is likely to suffer. Patients, who for whatever reason might not accept the validity of EBCAs, might engage clinicians in time-consuming clinical debate or might express dissatisfaction or noncompliance with algorithm-guided care when they do not believe or trust the algorithm. Inpatient efforts that involve physicians of multiple specialties risk failure if all team members are not educated in regard to the evidence and the rationale for the EBCA. For instance, some general surgeons remain ignorant of the fact that the administration of narcotic pain medication to patients with abdominal pain will not lead to management errors in diagnosing these patients.36 Implementation of EBCAs for patients with sepsis requires extensive teamwork across numerous medical specialties and hospital departments. The ability of various educational methods to help important stakeholders "get the evidence straight," to improve non-EP awareness and acceptance of EBCAs, and to improve patients' understanding and acceptance of EBCAs requires further study. Gaddis GM et al. Acad Emerg Med 2007;14:
, as conceptualized by Glasziou and Haynes.30 Steps 1–3 (aware, accepted, and applicable) indicate information that is eligible to be translated to the patient. This idea is captured by the concept of bedside EBM. Clinicians must be able to recognize and accept the opportunity to deliver evidence-based care. Steps 3–5 (applicable, able, and acted on) encompass steps regarding whether evidence is usable and which clinical quality improvement initiatives can be monitored. Steps 6 and 7 (agreed to and adhered to) complete the implementation of an EBCA. Reproduced from Glasziou and Haynes30 with permission. EBM = evidence-based medicine; CATs = critical appraisal templates; EBCA = evidence-based clinical algorithms. However, implementation of EBCAs involves a team effort, and that team is not composed strictly of EPs. When EBCAs involve follow-up care of a physician from another specialty, implementation may be derailed if that follow-up physician is unaware of the EBCA. For example, an orthopedist ignorant of the OARs may react with disdain (which can cause patients to question the quality of their emergency department care) when no ankle film has been obtained for patients for whom the OARs determine no need for radiography. Nurses, who generally perceive themselves as patient advocates and educators, probably need to be both aware of and supportive of EBCAs if clinical implementation of EBCAs is to succeed. If nurses or allied health personnel, in conversations with patients, cast doubt on the validity or appropriateness of EBCAs, patient compliance and acceptance of these EBCAs is likely to suffer. Patients, who for whatever reason might not accept the validity of EBCAs, might engage clinicians in time-consuming clinical debate or might express dissatisfaction or noncompliance with algorithm-guided care when they do not believe or trust the algorithm. Inpatient efforts that involve physicians of multiple specialties risk failure if all team members are not educated in regard to the evidence and the rationale for the EBCA. For instance, some general surgeons remain ignorant of the fact that the administration of narcotic pain medication to patients with abdominal pain will not lead to management errors in diagnosing these patients.36 Implementation of EBCAs for patients with sepsis requires extensive teamwork across numerous medical specialties and hospital departments. The ability of various educational methods to help important stakeholders get the evidence straight, to improve non-EP awareness and acceptance of EBCAs, and to improve patients understanding and acceptance of EBCAs requires further study. Gaddis GM et al. Acad Emerg Med 2007;14:")
73
Zusammenfassung

74
Leitlinien Entscheidungshilfen für die praktische klinische Tätigkeit
Entbinden nicht von kritischer Wertung, insbesondere für die Anwendung auf den individuellen Kranken Gewähren Rahmen, von dem begründet d.h. unter Vor-aussetzung angemessener Kompetenz abgewichen werden kann (soll, muß) zugunsten patientenbezogener, ökonomischer, oder organisatorischer Argumente Dem Mißbrauch um politischer Interessen willen muß entgegengetreten werden Um alle diese PROBLEME LEICHTER LÖSEN ZU KKÖNNEN; HABE WISS Fachgesellschaften Leitlinien nach Maßgabe der aktuellen wiss Liueratur erstellt, in die aber auch dort, wo keine Daten verfügbar, zB Expertenmeinungen aufgenommen sind..... Mit Argumentation auf Stand des Wissens unter Kompetenten, Möglichkeit der Abweichung entbindet allerdings nicht von der Notwendigkeit die Daten zu kennen. Bescheidenheit angesagt. Intellektuelle Herausforderung, Motivation, Begeisterung, Einbeziehung des Patienten, rationelle Durchdringung, trotzdem noch genug Platz für Mystik
 zugunsten patientenbezogener, ökonomischer, oder organisatorischer Argumente. Dem Mißbrauch um politischer Interessen willen muß entgegengetreten werden. Um alle diese PROBLEME LEICHTER LÖSEN ZU KKÖNNEN; HABE WISS Fachgesellschaften Leitlinien nach Maßgabe der aktuellen wiss Liueratur erstellt, in die aber auch dort, wo keine Daten verfügbar, zB Expertenmeinungen aufgenommen sind..... Mit Argumentation auf Stand des Wissens unter Kompetenten, Möglichkeit der Abweichung entbindet allerdings nicht von der Notwendigkeit die Daten zu kennen. Bescheidenheit angesagt. Intellektuelle Herausforderung, Motivation, Begeisterung, Einbeziehung des Patienten, rationelle Durchdringung, trotzdem noch genug Platz für Mystik.")
76
3 Säulen der klinischen Entscheidung
Leitlinienempfehlungen Individuelle Patientenproblematik Präferenz des Patienten

Ähnliche Präsentationen
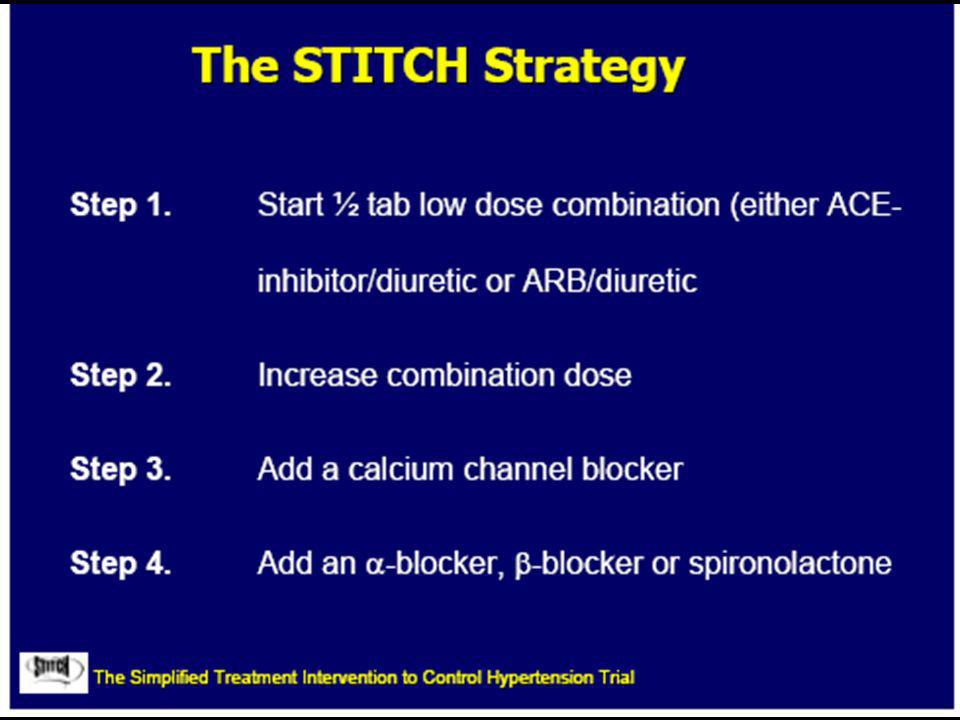
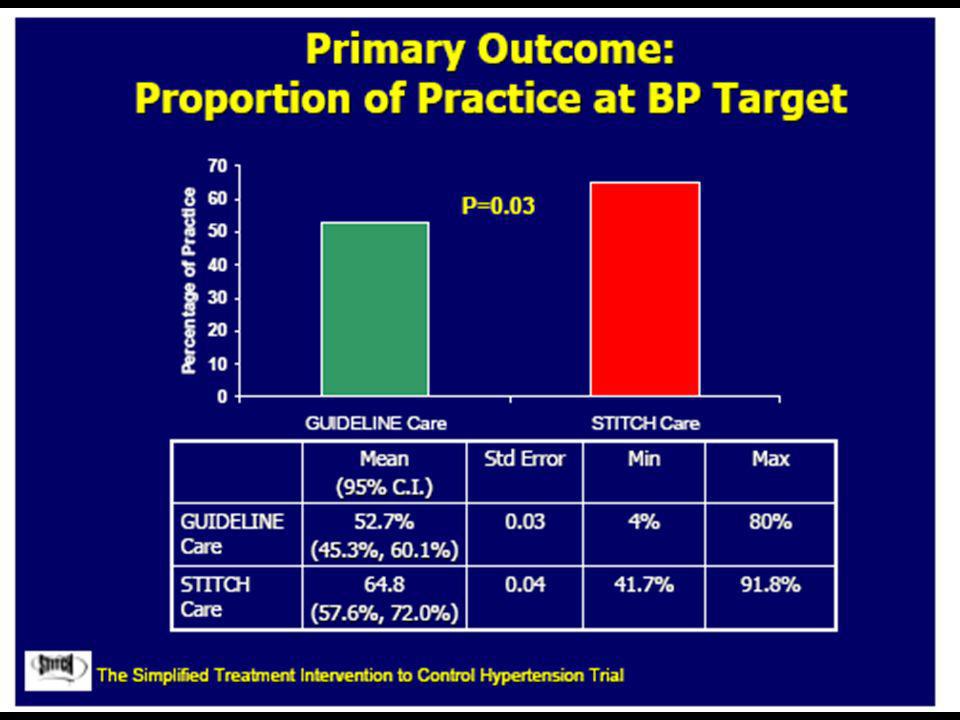


















 in Germany elective subject for medical students during.>")


