Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
C Gubler 17.9.2014 KSSG Ablationen Gallenwege & Pankreas

2
Abtragung von Gewebe SystemischChemotherapie LocoregionalRadiotherapie Chirurgie Locoregional- Interventionell HAI PDT PEI SIRT RFA TACE MWA Nanoknife

3
Abtragung von Gewebe SystemischChemotherapie LocoregionalRadiotherapie Chirurgie Locoregional- Interventionell HAI PDT PEI SIRT RFA TACE MWA Nanoknife

4
-luminal nativ -luminal FK -Parenchym

5
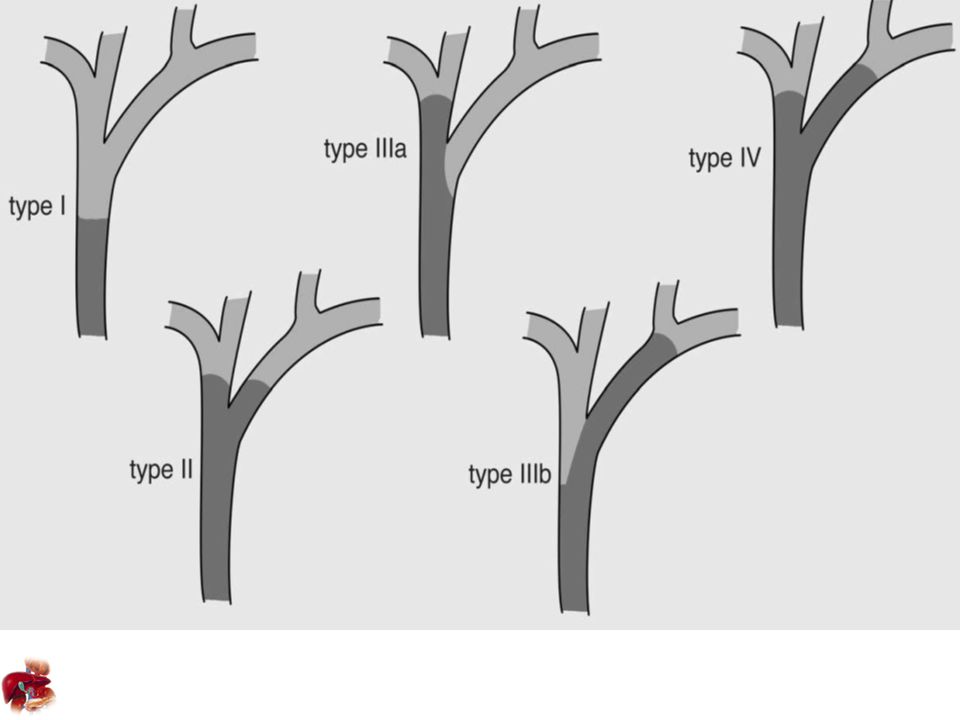
Maligne CCC/PAC nicht kurativ SEMS nicht kurativ Benigne NET anatomisch ungünstig SEMS nicht beschichtet

6
Palliation CCC/PAC Symptome Schmerz, Cholangitis, Pruritus, Nutrition Stent vs. Chirurgieprimär Endoskopie Smith Lancet 1994 Plastikdrain 1 > 2 Di Palma GI endoscopy 2001 PTCD vs. Endoskopieperkutan weniger Eingriffe Paik GI endoscopy 2009 SEMS vs. PlastikKosten abhängig vom Überleben Raju Dig Dis Sci 2011 SEMS coveredEinwachsen vs. Migration Kullmann GI endoscopy 2010 Individueller strategischer Entscheid pro Patient

8
Palliation CCC Überleben SEMS -/+ PDT98 versus 493 Tage Ortner Gastroenterology 2003 Cisplatin + Gemcitabine 11.7 vs 8.1 Monate Gemcitabine Valle N Eng J Med 2010 3 mt 8-12 Mt16 Mt RFA

9
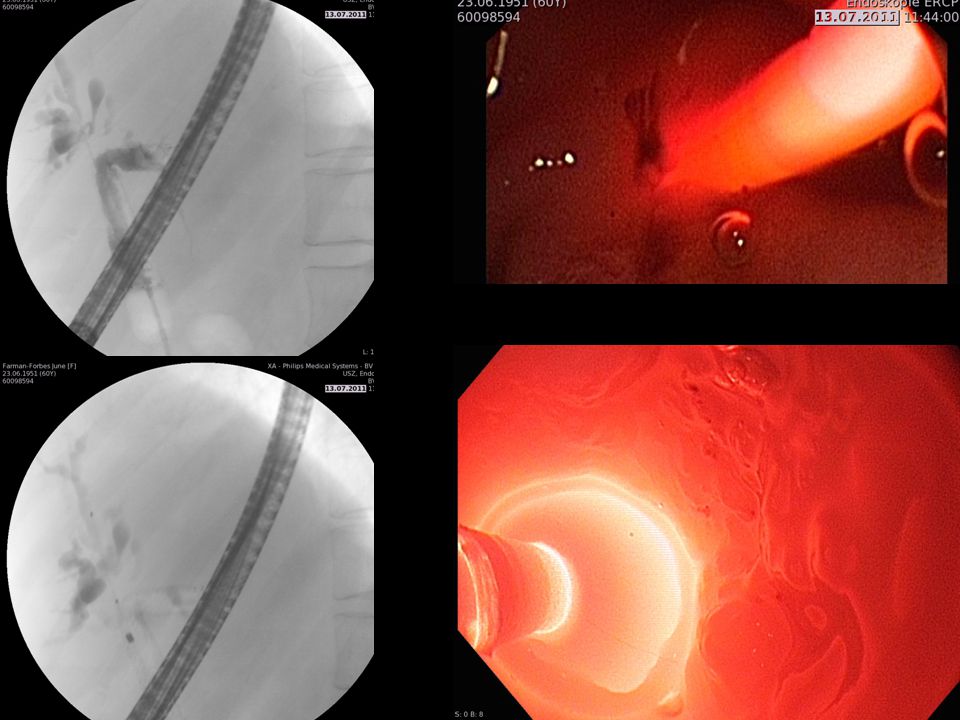
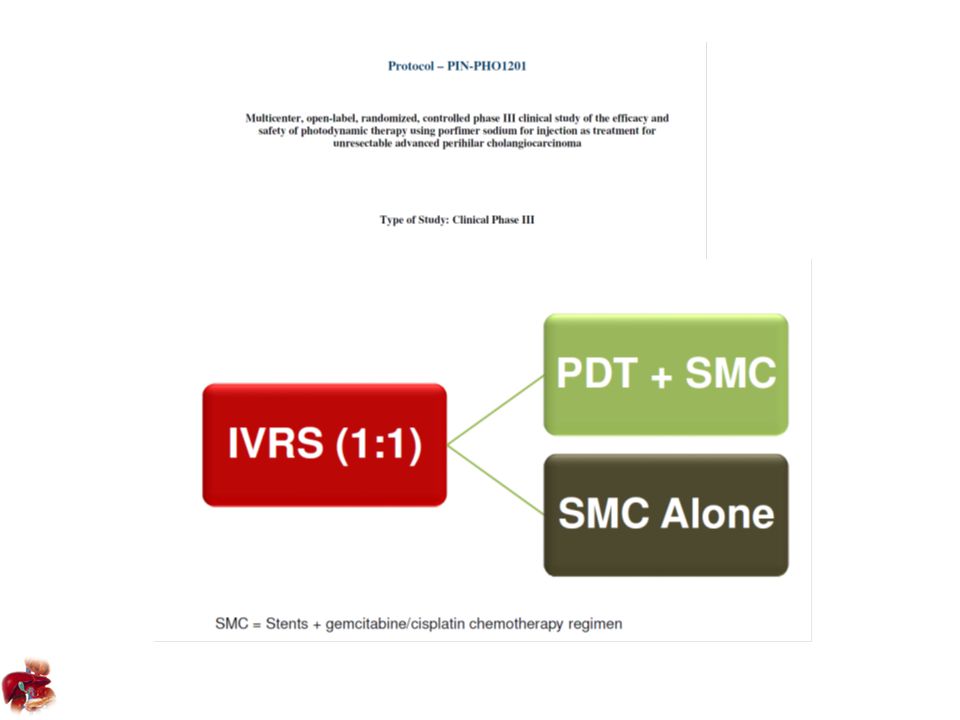
2003 Ortner Gastroenterology prospektiv randomisierte multicenter Studie Photofrin 2mg/kg KG 20 pt PDT mit Stent vs. 19 pt nur Stent 493 Tagevs. 93 Tage Witzigmann 2006 Kahaleh 2008 2010 Pereira Abstract ESMO prospektive randomisierte multicenter Studie Porfimer Sodium 92 pt PDT mit Stent vs nur Stent 5.6 Mt vs 8.5 Mt. PDT wird nicht routinemässig empfohlen Khan BMJ 2012

12
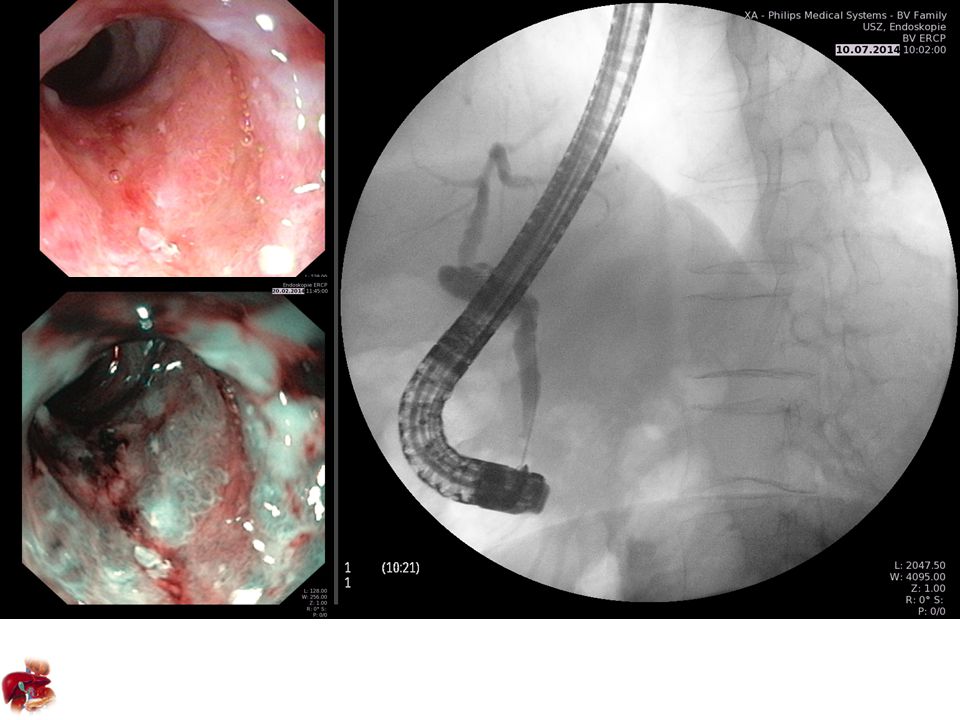
First in men 2011 Steel/Westaby 22 pt16 Pankreas-, 6 Cholangiokarzinome ERCP mit Cholangiographie RFA mit Habib 1.8cm Länge 5-10 Watt für 2 Minuten, Pause 1 Minute Einlage unbeschichteter Stent

13
Itoi 2012 Ex vivo Leber suis 5 – 10- 15- 20 Watt 60 -90- 120 sec

14
Kallis GUT 2011 24 pt + 44 matched Kontrollen17 CCC und 7 PAC Überleben 227 d für RFA und 159 d nur Stent Komplikationen: 1x Cholezystitis, 1x Pankreatitis Figueroa J Oncol 2013 20 pt 11 CCC, 7 PAC 1 IPMN, 1 gastric metastasis 30 Tage- alle Stents offen Komplikationen: 5x Schmerzen, 1x Pankreatitis, 1x Cholezystitis Dolak Surg Endoscopy 2013 58 pt 51 CCC, 4 PAC, 3 mixed HCC/CCC Medianes Überleben nach RFA 10.6 Mt (6.9 – 14.4) Komplikationen: 7 x Cholangitis, 1 x Leber Infarkt, 1x GaBla Empyem 3x Hämobilie, 1x LSB, 1x Leberkoma Sharaiha Dig Dis Sci 2014 26 pt + 40 matched Kontrollen18 CCC und 8 PAC 30 Tage- alle Stents offen Komplikationen: 5x Schmerzen, 1x Cholezystitis, 1x Pankreatitis Ungenügende Evidenz Sicher Ev. Längeres Überleben

15
Hu Dig Endoscopy 2014 9 patienten 4 postop, 3 OLT, 1 entzündlich, 1 cP 4 geheilt, 2 Relaps, 2 SEMS in situ, 1 Tod Mavrogenis Endoscopy 2012 Biliäres Adenom

17
RFA zur Palliation 7 Patienten4 CCC, 2 PAC, 1 CRC Metastase Überleben mean 5.3 Monate (3d – 10 Mt) UAW: 2x Schmerzen RFA zur Eröffnung Stent 2 Patienten-Entfernung nein -biliodigestive Anastomose -Wiedereröffnung 4 Monate RFA bei Restadenom 1 PatientinBiopsie nach 5 Monaten negativ Bipolar Monopolar
 UAW: 2x Schmerzen RFA zur Eröffnung Stent 2 Patienten-Entfernung nein -biliodigestive Anastomose -Wiedereröffnung 4 Monate RFA bei Restadenom 1 PatientinBiopsie nach 5 Monaten negativ Bipolar Monopolar")
19
RFA EUS gesteuert 19 – 22 G Nadel = 1 FR Katheter (0.33mm), monopolar auf 0.014’’ Draht All in one – Tip 1.27mm (18G) Rossi Pancreas 201410 NET, Follow-Up 34 Mt. Pai BSGPoster 20137 Pat. Mit PAC Pai DDW Poster 20148 Pat. Zystische Tumoren 1 HPB Unit, Hammersmith Hospital, Imperial College, London, UK 2 Bezmi Alem University, Istanbul, Turkey 3 Asian Institute of Gastroenterology, Hyderabad, India 4 Department of Transplant Medicine, University Hospital Münster, Germany 5 Digestive Endoscopy Center, Changhai Hospital, Second Military Medical University, Shanghai, China 6 GI Department, Hangzhou First People’s Hospital, Hangzhou, China 7 Division of Gastroenterology & Hepatology, Department of Medicine, Weill Cornell Medical College, New York, NY 10065, USA 8 Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114, USA

20
Succus RFA luminal ist sicher aber nicht etabliert RFA hält Stent länger offen RFA kann ev. Überleben verlängern RFA bei uncovered Stents RFA Parenchym eine Option in Zukunft

Ähnliche Präsentationen


 bei der>")



 BENCHMRK: Blocking integrase in treatment Experienced patients.>")
 U N I V E R S I T Ä T H A M B U R G November 2011.>")

Media Landesanstalt für Kommunikation Baden-Württemberg (LFK) Landeszentrale für Medien und Kommunikation.>")









