Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Referenzfilme zu Berufskrankheiten der Wirbelsäule
BK 2108, 2109, 2110 Stand: Juli 2005 Konsensusarbeitsgruppe des HVBG Dr. Kurt G. Hering, Dortmund

2
Referenzfilme - WS Definitionen:
Sklerose - I° - optisch wahrnehmbare vermehrte Sklerose (Osteose) II° - HWS - > 1 mm Sklerose der WK-Abschlußplatten - BWS/LWS - > 2 mm Sklerose der WK-Abschl. Chondrose - I° - Höhenminderung mittig ≥ 1/5 bis 1/3 (HWS bis 1/2) II° - Höhenminderung mittig >1/3 bis 1/2 (HWS > 1/2) III° - Höhenminderung mittig >1/2 IV° - Ankylosierende Chondrose Spondylose - I° - HWS/obere BWS bis 1 mm; untere BWS/LWS bis 2 mm II° - HWS/obere BWS bis 2-3 mm; untere BWS/LWS 3-5 mm III° - HWS/obere BWS über 3 mm; untere BWS/LWS >5 mm IV° - Tendenzielle und vollständige Brückenbildung Retrospondylose I° - bis 2 mm II°- ab 3 mm Spondylarthrose I° - vermehrte Sklerose der Wirbelgelenke erkennbar II° - + Verplumpungen od. Randanbauten der Wirbelgelenke
 II° - HWS - > 1 mm Sklerose der WK-Abschlußplatten. - BWS/LWS - > 2 mm Sklerose der WK-Abschl. Chondrose - I° - Höhenminderung mittig ≥ 1/5 bis 1/3 (HWS bis 1/2) II° - Höhenminderung mittig >1/3 bis 1/2 (HWS > 1/2) III° - Höhenminderung mittig >1/2. IV° - Ankylosierende Chondrose. Spondylose - I° - HWS/obere BWS bis 1 mm; untere BWS/LWS bis 2 mm. II° - HWS/obere BWS bis 2-3 mm; untere BWS/LWS 3-5 mm. III° - HWS/obere BWS über 3 mm; untere BWS/LWS >5 mm. IV° - Tendenzielle und vollständige Brückenbildung Retrospondylose I° - bis 2 mm II°- ab 3 mm Spondylarthrose I° - vermehrte Sklerose der Wirbelgelenke erkennbar. II° - + Verplumpungen od. Randanbauten der Wirbelgelenke.")
3
Referenzfilme - WS Definitionen:
Sklerose (Osteose) - vermehrte Sklerosierung der Deck- und Bodenplatten (unabhängig von einer ggf. gleichzeitig vorliegenden Höhenminderung der Bandscheibe) Grad I - optisch wahrnehmbare vermehrte Sklerose Grad II - HWS - > 1 mm Sklerose der WK-Abschlußplatten BWS/LWS - > 2 mm Sklerose der WK-Abschl.
 - vermehrte Sklerosierung der Deck- und Bodenplatten (unabhängig von einer ggf. gleichzeitig vorliegenden Höhenminderung der Bandscheibe) Grad I - optisch wahrnehmbare vermehrte Sklerose. Grad II - HWS - > 1 mm Sklerose der WK-Abschlußplatten. BWS/LWS - > 2 mm Sklerose der WK-Abschl.")
4
Referenzfilme - WS HWS BWS LWS
Sklerose (Osteose) [ SK ] - I° - optisch wahrnehmbare vermehrte Sklerose II°- HWS - > 1 mm Sklerose der WK-Abschlußplatten BWS/LWS - > 2 mm Sklerose der WK-Abschl. SK I SK I SK I SK I SK I SK I HWS BWS LWS
 [ SK ] - I° - optisch wahrnehmbare vermehrte Sklerose. II°- HWS - > 1 mm Sklerose der WK-Abschlußplatten. BWS/LWS - > 2 mm Sklerose der WK-Abschl. SK I. SK I. SK I. SK I. SK I. SK I. HWS. BWS. LWS.")
5
Referenzfilme - WS HWS BWS LWS
Sklerose (Osteose) [ SK ] - I° - optisch wahrnehmbare vermehrte Sklerose II°- HWS - > 1 mm Sklerose der WK-Abschlußplatten BWS/LWS - > 2 mm Sklerose der WK-Abschl. SK II SK II SK II HWS BWS LWS
 [ SK ] - I° - optisch wahrnehmbare vermehrte Sklerose. II°- HWS - > 1 mm Sklerose der WK-Abschlußplatten. BWS/LWS - > 2 mm Sklerose der WK-Abschl. SK II. SK II. SK II. HWS. BWS. LWS.")
6
Traktions-Spondylophyth
Referenzfilme - WS Sklerose (Osteose) - I° - optisch wahrnehmbare vermehrte Sklerose II°- HWS - > 1 mm Sklerose der WK-Abschlußplatten BWS/LWS - > 2 mm Sklerose der WK-Abschl. 1 Retrospondylose SKII SKII Traktions-Spondylophyth
 - I° - optisch wahrnehmbare vermehrte Sklerose. II°- HWS - > 1 mm Sklerose der WK-Abschlußplatten. BWS/LWS - > 2 mm Sklerose der WK-Abschl. 1. Retrospondylose. SKII. SKII. Traktions-Spondylophyth.")
7
Referenzfilme - WS Definitionen:
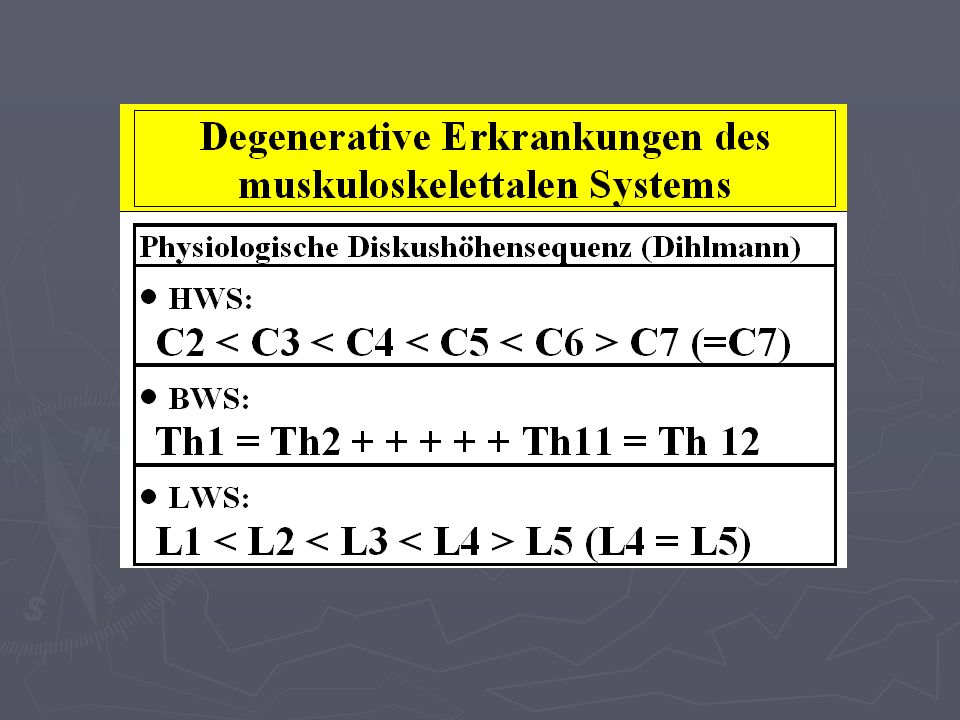
Chondrose - Höhenminderung der Bandscheibe, Bezugnahme auf gesunde WS-Abschnitte; s. „Dihlmann“-Regel Grad I - Höhenminderung mittig ≥ 1/5 bis 1/3 (HWS bis 1/2) Grad II - Höhenminderung mittig >1/3 bis 1/2 (HWS >1/2) Grad III - Höhenminderung mittig >1/2 Grad IV - Ankylosierende Chondrose
 Grad II - Höhenminderung mittig >1/3 bis 1/2 (HWS >1/2) Grad III - Höhenminderung mittig >1/2. Grad IV - Ankylosierende Chondrose.")
9
Referenzfilme - WS Definitionen:
Chondrose - Höhenminderung der Bandscheibe, Bezugnahme auf gesunde WS-Abschnitte; s. „Dihlmann“-Regel Grad I - Höhenminderung mittig ≥ 1/5 bis 1/3 (HWS bis 1/2) Grad II - Höhenminderung mittig >1/3 bis 1/2 (HWS > 1/2) Grad III - Höhenminderung mittig >1/2 Grad IV - Ankylosierende Chondrose
 Grad II - Höhenminderung mittig >1/3 bis 1/2 (HWS > 1/2) Grad III - Höhenminderung mittig >1/2. Grad IV - Ankylosierende Chondrose.")
10
Referenzfilme - WS Chondrose - I° - Höhenminderung mittig ≥ 1/5 bis 1/3 (HWS bis 1/2) II° - Höhenminderung mittig >1/3 bis 1/2 (HWS > 1/2) III° - Höhenminderung mittig >1/2 IV° - Ankylosierende Chondrose CH I CH I CH II CH III CH II CH II CH III CH I CH III(IV) CH I CH III CH IV
 CH I. CH III. CH IV.")
11
Referenzfilme - WS Definitionen:
Spondylose - Randzackenbildung ventral und lateral; s.a. „Dihlmann“ Grad I - HWS/obere BWS bis 1 mm untere BWS/LWS bis 2 mm Grad II - HWS/obere BWS bis 2-3 mm untere BWS/LWS bis 3-5 mm Grad III - HWS/obere BWS über 3 mm untere BWS/LWS über 5 mm Grad IV - Tendenzielle und vollständige Brückenbildung I° II° III° IV°

12
Referenzfilme - WS 4 5 6 2 verschiedene Patienten SP III SP I SP II
Schaltknochen SP IV 2 verschiedene Patienten

13
Referenzfilme - WS 4 6 6 7 8 9 Spondylose (SP): I° und II° 6 6
SP II 6 SP I 6 SP I SP II Spondylose (SP): I° und II° 2 verschiedene Patienten
: I° und II° 2 verschiedene Patienten.")
14
Referenzfilme - WS 1 3 2 5 3 3 4 5 Spondylose (SP): I°, II°, III°, IV
+ beginnende Bandverkalkung SP II SP I SP III SP II SP III SP II SP III SP II SP IV SP II Spondylose (SP): I°, II°, III°, IV 3 verschiedene Patienten
: I°, II°, III°, IV. 3 verschiedene Patienten.")
15
Traktions-Spondylophyth
Referenzfilme - WS Definitionen: Retrospondylose [ RS ]- - Randzackenbildung dorsal ; s. „Dihlmann“ Grad I - bis 2 mm Grad II - > 2 mm 1 Retrospondylose RS II Traktions-Spondylophyth

16
Referenzfilme - WS * 3 3 * 5 Retrospondylose - I° - bis 2 mm
II° - ab 3 mm 5 3 * # 3 RS I * = Retrospondylose # = Variante, betonte dorsale Randkontur RS I * * Verschiedene Patienten

17
Referenzfilme - WS Definitionen:
Spondylarthrose - Sklerose u. Randzackenbildung der kleinen Wirbelgelenke Grad I - vermehrte Sklerose der Wirbelgelenke erkennbar Grad II - Grad I plus Verplumpungen oder Randanbauten der Wirbelgelenke erkennbar

18
Referenzfilme - WS 3 5 Verschiedene Patienten
Spondylarthrose - I° - vermehrte Sklerose der Wirbelgelenke erkennbar II° - I° plus Verplumpungen oder Randanbauten der Wirbelgelenke erkennbar 3 SA I SA II SA I 5 SA II SA II SA I Verschiedene Patienten SA II

19
Referenzfilme - WS 4 5 I° 6 Sklerose: I° Chondrose: II° Spondylose:
Grad I (I°) Grad II (II°) Grad III (III°) Spondyl- arthrose 2 verschiedene Patienten
 Grad II (II°) Grad III (III°) Spondyl- arthrose. 2 verschiedene Patienten.")
20
Referenzfilme - WS Sklerose : I° Chondrose: I° + II° Spondylose:
5 5 6 6 5 Sklerose : I° Chondrose: I° + II° 6 Spondylose: I° und II° Uncarthrose:

21
Referenzfilme - WS Sklerose (Osteose) I° u. II° Chondrose III° u. IV°
Spondylose II° u. III° Spondylarthrose I° u. II°

22
Referenzfilme - WS Spondylose: Grad I Grad II Sklerose: I°
6 6 Costotransversalarthrose 7 7 8 8 6 6 9 9 Mediastinaler LN Spondylose: Grad I Grad II Sklerose: I° Chondrose:I°

23
Referenzfilme - WS 4 4 4 6 6 8 6 10 12 Sklerose: I°
Spondylose: I u. II°

24
Referenzfilme - WS Chondrose: I° 3 4 5 1 1 2 3 4 4 5

25
Referenzfilme - WS 3 Sklerose: I° 3 Chondrose: I u. II° Spondylose: 4
5 5 3 * Sklerose: I° Chondrose: I u. II° Spondylose: I und II° * Retrospondylose I° 2 verschiedene Patienten

26
Referenzfilme - WS 1 2 3 5 3 Sklerose: I° u. II° Chondrose: I° - IV°
4 5 5 3 Sklerose: I° u. II° Chondrose: I° - IV° Spondylose: I°, II° u. III° Spondylarthrose: I° u. II° 3 verschiedene Patienten

27
Referenzfilme - WS CT – Definitionen:
Verlagerung von Bandscheibengewebe Grad I: Konzentrische Vorwölbung (Protrusion) Konkavität dorsal aufgehoben, Vorwölbung über Verbindungslinie WK-Hinterkante bis 3mm* Grad II: Verlagerung des Nukleus (Vorfall) Vorwölbung 5 mm* Grad III: Vorfall mit Sequestration Strukturänderung: Vakuumphänomen, Destruktion * !! Grenzbefunde >3 bis <5 mm, siehe ergänzende Folie !!
 Konkavität dorsal aufgehoben, Vorwölbung über Verbindungslinie WK-Hinterkante bis 3mm* Grad II: Verlagerung des Nukleus (Vorfall) Vorwölbung 5 mm* Grad III: Vorfall mit Sequestration. Strukturänderung: Vakuumphänomen, Destruktion. * !! Grenzbefunde >3 bis <5 mm, siehe ergänzende Folie !!")
28
s. auch „Consensus AJNR“ (auf gleicher CD-ROM)
")
29
Referenzfilme - WS I° = konzentrische Ausweitung („bulging“)
- Protrusion - II° = Ausweitung ≥5 mm, Verlagerung des Nukleus - Vorfall - III° = Vorfall und Sequester

30
Referenzfilme - WS B = medio-lateral C = lateral A = medial

31
Referenzfilme - WS Definitionen: MRT –
Signaländerung der Deck- und Bodenplatten (Modic) Höhen- und Signaländerung der Bandscheibe Verlagerung von Bandscheibengewebe Grad I: Konkavität dorsal aufgehoben (Protrusion), Vorwölbung über Verbindungslinie WK-Hinterkante bis 3mm* Grad II: Verlagerung 5 mm*(Vorfall) Grad III: Vorfall mit Sequestration * !! Grenzbefunde >3 bis <5 mm, siehe ergänzende Folie !!
 Höhen- und Signaländerung der Bandscheibe. Verlagerung von Bandscheibengewebe Grad I: Konkavität dorsal aufgehoben (Protrusion), Vorwölbung über Verbindungslinie WK-Hinterkante bis 3mm* Grad II: Verlagerung 5 mm*(Vorfall) Grad III: Vorfall mit Sequestration. * !! Grenzbefunde >3 bis <5 mm, siehe ergänzende Folie !!")
32
Referenzfilme - WS Reaktion der WK: Einteilung nach MODIC

33
Referenzfilme - WS T1 T2 Reaktion der WK-Abschlußplatten:
Einteilung nach MODIC T1 T2 Bsp. Typ 2 - L5/S1

34
Referenzfilme - WS c, b? c, e?
Risstypen (Yu 1989 nach Uhlenbrock 2001: a Normalbefund b Konzentrischer Riss c Transversaler Riss d Radialer Riss e Kompletter Riss

35
Referenzfilme - WS M-II T1W M-III M-II MODIC Typ II (M-II)
Reaktion der WK-Abschlußplatten: Einteilung nach MODIC M-II T1W M-III M-II MODIC Typ II (M-II) Typ III (M-III) M-III T2W
 Typ III (M-III) M-III. T2W.")
36
Radiologie der Wirbelsäule

37
Menmonic Skelettbeurteilung
H K K W !! Befund-Diktat immer geordnet, Reihenfolge einhalten !!

38
Referenzfilme - WS Übersichtsschema als Hilfe beim Diktat (in Einschweißfolie)
")
39
Eingeführte Messmethoden (Winkelangaben) - Überblick -
Zervikale Lordose Thorakale Kyphose Lumbal-Lordose Lumbosakrale Lordose Sakrale Inklination Lumbosakralwinkel nach JUNGHANNS Promotoriumswinkel Dorsaler Neigungswinkel des Sakrums (Delta-Winkel) Lumbosakralwinkel (FERGUSON-Winkel) entspricht Kreuzbeinbasiswinkel Lot von L3 (FERGUSON´sche Belastungslinie) Skoliosewinkel nach COBB-LIPPMANN Skoliosewinkel nach RISSER-FERGUSON Torsionsbestimmung nach COBB Torsionsbestimmung nach NASH-MOE Spondylolisthesis (Erklärung: = gebräuchlichste Methode)
 Lumbosakralwinkel (FERGUSON-Winkel) entspricht Kreuzbeinbasiswinkel. Lot von L3 (FERGUSON´sche Belastungslinie) Skoliosewinkel nach COBB-LIPPMANN. Skoliosewinkel nach RISSER-FERGUSON. Torsionsbestimmung nach COBB. Torsionsbestimmung nach NASH-MOE. Spondylolisthesis. (Erklärung: = gebräuchlichste Methode)")
40
Messmethoden an der Wirbelsäule (Winkelangaben)
Zervikale Lordose Linie durch die Atlasebene, Tangente entlang Basisplatte C7, Winkel am Schnittpunkt = Lordosewinkel Ø 40° (35–45°)
")
41
Messmethoden an der Wirbelsäule (Winkelangaben)
Thorakale Kyphose Tangente entlang der Deckplatte des 3. BWK, (alternativ 1. BWK) Tangente entlang Basisplatte des 11. BWK, (alternativ 12. BWK) Winkel am Schnittpunkt = Kyphosewinkel Ø 25°, geschlechts- und altersabhängig
 Tangente entlang Basisplatte des 11. BWK, (alternativ 12. BWK) Winkel am Schnittpunkt = Kyphosewinkel Ø 25°, geschlechts- und altersabhängig.")
42
Messmethoden an der Wirbelsäule (Winkelangaben)
Lumbal-Lordose Tangente entlang Deckplatte L1 und Deckplatte S1. Winkel am Schnittpunkt = Lordosewinkel: Normalwert 50–60°

43
Messmethoden an der Wirbelsäule (Winkelangaben)
Lumbosakrale Lordose Verbindungslinie durch Zentren L3, L5 und S1 = Lumbosakraler Lordosewinkel Ø 146° (124–162°)
")
44
Messmethoden an der Wirbelsäule (Winkelangaben)
Sakrale Inklination Senkrechte Linie entlang Hinterkante L5, Tangente dorsale Hinterkante S1 = Inklination Ø 46° (30–72 °)
")
45
Messmethoden an der Wirbelsäule (Winkelangaben)
Lumbosakralwinkel nach JUNGHANNS Schnitt der Trageachse des 5. LWK und der Trageachse des Segments L1, nach hinten offener stumpfer Winkel

46
Messmethoden an der Wirbelsäule (Winkelangaben)
Promotoriumswinkel Schnittpunkt Tangente an der Vorderkante L5 und Tangente Vorderkante S1

47
Messmethoden an der Wirbelsäule (Winkelangaben)
Dorsaler Neigungs-winkel des Sakrums, sog. Delta-Winkel Schnittpunkt Tangente an der Hinterkante von S1 und S2 und Horizontale a) „Horizontales Sakrum“ = Winkel Delta < 35° b) „Neutrales Sakrum“ = Winkel Delta 35 bis 45° c) „Steiles Sakrum“ = Winkel Delta > 45°
 „Horizontales Sakrum = Winkel Delta < 35° b) „Neutrales Sakrum = Winkel Delta 35 bis 45° c) „Steiles Sakrum = Winkel Delta > 45°")
48
Messmethoden an der Wirbelsäule (Winkelangaben)
Lumbosakralwinkel FERGUSON-Winkel entspricht Kreuzbeinbasiswinkel Horizontallinie parallel zur Filmbasis, Tangente entlang der Deckplatte S1 = Lumbosakralwinkel Ø 41° (26-57°)
")
49
Messmethoden an der Wirbelsäule (Winkelangaben)
Lot von L3 = FERGUSON‘sche Belastungslinie Lot vom Zentrum L3 bilden, Relation zur Vorderkante S1. Normal: Etwa durch Vorderkante, > 10 mm vor Vorderkante: Verstärkte Scherkräfte, Dorsalverlagerung: Verstärkte Belastung der lumbosakralen Gelenke

50
Messmethoden an der Wirbelsäule (Winkelangaben)
Skoliosewinkel nach COBB-LIPPMANN Winkel zwischen Deckplatte des oberen Skoliose-Endwirbels und Bodenplatte des unteren Skoliose-Endwirbels

51
Messmethoden an der Wirbelsäule (Winkelangaben)
Skoliosewinkel nach RISSER-FERGUSON Winkel zwischen den Linien durch das Zentrum des Apexwirbels und den Mittelpunkt des oberen und unteren Skoliose-Endwirbels

52
Messmethoden an der Wirbelsäule (Winkelangaben)
Torsionsbestimmung nach COBB Abweichung des Proc. spinosus aus der Mittellinie: Wirbel in sechs gleich große Abschnitte eingeteilt a = Mittellinie, b, c, d Abweichung nach re. oder li. Processus bei b = + Rotation; bei c = ++ Rotation, bei d = +++ Rotation

53
Messmethoden an der Wirbelsäule (Winkelangaben)
Torsionsbestimmung nach NASH-MOE Abweichung der Pedikelposition: Wirbel in sechs gleich große Abschnitte eingeteilt. Normal-Pedikel seitengleich in äußeren Feldern; Pedikel einer Seite teilweise abgebildet = +Rotation; Pedikel einer Seite nicht mehr abgebildet = ++; 1 Pedikel im Zentrum = +++; Pedikel überschreitet Mittellinie = ++++

54
Messmethoden an der Wirbelsäule (Winkelangaben)
Spondylolisthesis Messung der Spondylolisthesis nach MEYERDING: Einteilung der Deckplatte S1 in 4 Segmente, Ventralverschiebung nach Anzahl der verschobenen Segmente von 1-4

55
Nomenclature and Classification of Lumbar Disc Pathology
Consensus, präsentiert von der American Society of Neuroradiology, American Society of Spine Radiology and North American Spine Society American Journal of Neuroradiology 2003

56
(Figure 1) General classification of disc disorders. In the proposed model, the use of the "normal" category is restricted to discs free of any degenerative changes, whether age related or pathologic. (Adapted from Milette PC. Classification, diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000; 38: )
")
57
(Figure 2) Schematic sagittal anatomical sections showing the differentiating features of an anular tear (radial tear in this case) and a disc herniation. The term "tear" is used to refer to a localized radial, concentric, or horizontal disruption of the anulus without associated displacement of disc material beyond the limits of the intervertebral disc space. Nuclear material is shown in black, and the anulus (internal and external) corresponds to the white portion of the intervertebral space. The same convention is used in Figures 3, 12, 13, and 14. (Adapted from Milette PC. The proper terminology for reporting lumbar intervertebral disk disorders. AJNR Am J Neurorad 1997;18: ; with permission.)
 and a disc herniation. The term tear is used to refer to a localized radial, concentric, or horizontal disruption of the anulus without associated displacement of disc material beyond the limits of the intervertebral disc space. Nuclear material is shown in black, and the anulus (internal and external) corresponds to the white portion of the intervertebral space. The same convention is used in Figures 3, 12, 13, and 14. (Adapted from Milette PC. The proper terminology for reporting lumbar intervertebral disk disorders. AJNR Am J Neurorad 1997;18: ; with permission.)")
58
(Figure 3) Schematic sagittal anatomical sections showing the differentiating characteristics of the normal disc, spondylosis deformans, and intervertebral osteochondrosis. The distinction between these three entities is usually possible on all imaging modalities, including conventional radiographs. (Adapted from Milette PC. The proper terminology for reporting lumbar intervertebral disk disorders. AJNR Am J Neurorad 1997;18: ; with permission.)
")
59
(Figure 4) The term "herniated disc", as defined in this work, refers to localized displacement of nucleus, cartilage, fragmented apophyseal bone, or fragmented anular tissue beyond the intervertebral disc space (disc space, interspace). The interspace is defined, craniad and caudad, by the vertebral body end-plates.. Two intravertebral herniations, one with an upward orientation and the other with a downward orientation with respect to the disc space, are illustrated schematically.
. The interspace is defined, craniad and caudad, by the vertebral body end-plates.. Two intravertebral herniations, one with an upward orientation and the other with a downward orientation with respect to the disc space, are illustrated schematically.")
60
(Figure 5) The interspace is defined, peripherally, by the edges of the vertebral ring apophyses, exclusive of osteophytic formations. The line drawing schematically illustrates a localized extension of disc material beyond the intervertebral disc space, in a left posterior direction, which qualifies as a disc herniation.

61
(Figure 6) For classification purposes, the intervertebral disc is considered as a two dimensional round or oval structure having four 90 quadrants. By convention, a herniation is a "localized" process involving less than 50% (180) of the disc circumference.
 of the disc circumference.")
62
(Figure 7) By convention, a "focal herniation" involves less than 25% (90) of the disc circumference.
 By convention, a focal herniation involves less than 25% (90) of the disc circumference.")
63
Figure 8) By convention, a "broad-based" herniation involves between 25% and 50% (90-180) of the disc circumference.
 By convention, a broad-based herniation involves between 25% and 50% (90-180) of the disc circumference.")
64
(Figure 9) Symmetrical presence (or apparent presence) of disc tissue "circumferentially" (50-100%) beyond the edges of the ring apophyses may be described as a "bulging disc" or "bulging appearance", and is not considered a form of herniation. Furthermore, “bulging” is a descriptive term for the shape of the disc contour and not a diagnostic category.
 of disc tissue circumferentially (50-100%) beyond the edges of the ring apophyses may be described as a bulging disc or bulging appearance , and is not considered a form of herniation. Furthermore, bulging is a descriptive term for the shape of the disc contour and not a diagnostic category.")
65
(Figure 10) Asymmetrical bulging of the disc margin (50%-100%), such as is found in severe scoliosis, is also not considered a form of herniation.
 Asymmetrical bulging of the disc margin (50%-100%), such as is found in severe scoliosis, is also not considered a form of herniation.")
66
(Figure 11) Herniated discs may take the form of protrusion or extrusion, based on the shape of the displaced material (see definitions in text).
 Herniated discs may take the form of protrusion or extrusion, based on the shape of the displaced material (see definitions in text).")
67
(Figure 12) When a relatively large amount of disc material is displaced, distinction between protrusion (A) and extrusion (B or C) will generally only be possible on sagittal MR sections or sagittal CT reconstructions. In Figure C, although the shape of the displaced material is similar to that of a protrusion, the greatest cranio-caudal diameter of the fragment is greater than the cranio-caudal diameter of its base at the level of the parent disc, and the lesion therefore qualifies as an extrusion. In any situation, the distance between the edges of the base, which serves as reference for the definition of protrusion and extrusion, may differ from the distance between the edges of the aperture in the anulus, which cannot be assessed on CT images and is seldom appreciated on MR images. In the cranio-caudal direction, the length of the base cannot exceed, by definition, the height of the intervertebral space (Adapted from Milette PC. Classification, diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000; 38: )
 and extrusion (B or C) will generally only be possible on sagittal MR sections or sagittal CT reconstructions. In Figure C, although the shape of the displaced material is similar to that of a protrusion, the greatest cranio-caudal diameter of the fragment is greater than the cranio-caudal diameter of its base at the level of the parent disc, and the lesion therefore qualifies as an extrusion. In any situation, the distance between the edges of the base, which serves as reference for the definition of protrusion and extrusion, may differ from the distance between the edges of the aperture in the anulus, which cannot be assessed on CT images and is seldom appreciated on MR images. In the cranio-caudal direction, the length of the base cannot exceed, by definition, the height of the intervertebral space (Adapted from Milette PC. Classification, diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000; 38: )")
68
Radiol Clin North Am 2000; 38:1267-1292)
(Figure 13) Schematic representation of various types of posterior central herniations. A, Small sub-ligamentous herniation (or protrusion) without significant disc material migration. B, Sub-ligamentous herniation with downward migration of disc material under the posterior longitudinal ligament (PLL). C, Sub-ligamentous herniation with downward migration of disc material and sequestered fragment (arrow). (From Milette PC. Classification, diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000; 38: )
 Schematic representation of various types of posterior central herniations. A, Small sub-ligamentous herniation (or protrusion) without significant disc material migration. B, Sub-ligamentous herniation with downward migration of disc material under the posterior longitudinal ligament (PLL). C, Sub-ligamentous herniation with downward migration of disc material and sequestered fragment (arrow). (From Milette PC. Classification, diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000; 38: )")
69
Radiol Clin North Am 2000; 38:1267-1292)
(Figure 14) Relationship of typical posterior disc herniations with the posterior longitudinal ligament. A, Midline sagittal section: unless very large, a posterior midline herniation usually remains entrapped underneath the deep layer of the PLL and sometimes a few intact outer anulus fibers joining with the PLL to form a “ capsule.” The deep layer of the PLL (arrow) also attaches to the posterior aspect of the vertebral body so that no potential space is present underneath. B, Sagittal para-central section: the PLL extends laterally at the disc level (arrowhead) but, above and below the disc, an anterior epidural space (as), where disc fragments are frequently entrapped, is present between the lateral membranes (peridural membrane) and the posterior aspect of the vertebral bodies. (Adapted from Milette PC. Classification, diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000; 38: )
 Relationship of typical posterior disc herniations with the posterior longitudinal ligament. A, Midline sagittal section: unless very large, a posterior midline herniation usually remains entrapped underneath the deep layer of the PLL and sometimes a few intact outer anulus fibers joining with the PLL to form a capsule. The deep layer of the PLL (arrow) also attaches to the posterior aspect of the vertebral body so that no potential space is present underneath. B, Sagittal para-central section: the PLL extends laterally at the disc level (arrowhead) but, above and below the disc, an anterior epidural space (as), where disc fragments are frequently entrapped, is present between the lateral membranes (peridural membrane) and the posterior aspect of the vertebral bodies. (Adapted from Milette PC. Classification, diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000; 38: )")
70
(Figure 15) Proposed categories for the description and classification of disc herniations. Some distinctions may not be possible with currently available non-invasive imaging modalities

71
Coronal drawing illustrating the main anatomical "zones" and "levels".
(Figure 16) Coronal drawing illustrating the main anatomical "zones" and "levels". (From Wiltse LL, Berger PE, McCulloch JA. A system for reporting the size and location of lesions of the spine. Spine 1997;22: )
 Coronal drawing illustrating the main anatomical zones and levels . (From Wiltse LL, Berger PE, McCulloch JA. A system for reporting the size and location of lesions of the spine. Spine 1997;22: )")
72
by an imaginary coronal line in the center of the vertebral body.
(Figure 17) Schematic representation of the anatomical "zones" identified on axial images. The anterior zone (not illustrated) is delineated from the extra-foraminal zone by an imaginary coronal line in the center of the vertebral body. (Adapted from Wiltse LL, Berger PE, McCulloch JA. A system for reporting the size and location of lesions of the spine. Spine 1997;22: )
 Schematic representation of the anatomical zones identified on axial images. The anterior zone (not illustrated) is delineated from the extra-foraminal zone. by an imaginary coronal line in the center of the vertebral body. (Adapted from Wiltse LL, Berger PE, McCulloch JA. A system for reporting the size and location of lesions of the spine. Spine 1997;22: )")
73
(Adapted from Wiltse LL, Berger PE, McCulloch JA.
(Figure 18) Schematic representation of the anatomical "levels" identified on cranio-caudal images. (Adapted from Wiltse LL, Berger PE, McCulloch JA. A system for reporting the size and location of lesions of the spine. Spine 1997;22: )
 Schematic representation of the anatomical levels identified on cranio-caudal images. (Adapted from Wiltse LL, Berger PE, McCulloch JA. A system for reporting the size and location of lesions of the spine. Spine 1997;22: )")
74
Nomenclature and Classification of Lumbar Disc Pathology
APPENDIX Chairpersons of the Task Forces David F. Fardon, MD Orthopedic Surgeon Knoxville Orthopedic Clinic Knoxville, Tennessee USA Pierre C. Milette, MD Neuroradiologist Clinical Professor of Radiology Université de Montréal Montreal, Quebec Canada Members of the Task Forces Brigitte Appel, M.D. Neuroradiologist Head of Neuroradiology-CT-MRI. A.Z. Middelheim Antwerp, Belgium Jean-François Bonneville, MD Neuroradiologist Professor of Neuroradiology Université de Franche-Comté Besançon, France Tom Faciszewski, MD Orthopedic Surgeon Marshfield Clinic Marshfield, Wisconsin USA Steven R. Garfin, MD Orthopedic Surgeon Professor of Orthopedic Surgery University of California, San Diego San Diego, California USA Scott Haldemann, MD, PhD Neurologist Associate Clinical Professor of Neurology University of California, Irvine Irvine, California USA Neil Kahanovitz, MD Orthopedic Surgeon Anderson Orthopedic Clinic Arlington, Virginia USA Marco Leonardi, MD Neuroradiologist Head of Neuroradiology Ospedala Bellaria Bologna, Italy Jeffrey S. Ross, MD Neuroradiologist Head of Radiology Research Cleveland Clinic Cleveland, Ohio USA Volker K.H. Sonntag, MD Neurological Surgeon Barrow Neurological Institute Phoenix, Arizona USA Alan L. Williams, MD Neuroradiologist Professor of Radiology St. Louis University St. Louis, Missouri USA Jan T. Wilmink, MD, PhD Neuroradiologist Professor of Neuroradiology University of Maastricht Maastricht, The Netherlands Consultants and Advisors Robert E. Florin, MD Neurological Surgeon Clinical Professor of Neurosurgery University of Southern California Los Angeles, California USA Richard J. Herzog, MD Radiologist Chief of Teleradiology Hospital for Special Surgery New York, New York USA Jerrold H. Mink, MD Radiologist Tower Imaging Medical Group Los Angeles, California USA John D. Simmons MD Neuroradiologist Abercrombie Radiology Knoxville, Tennessee USA

Ähnliche Präsentationen











 in Germany elective subject for medical students during.>")





 Trackball. Joystick.>")
>")
