Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Il monitoraggio nervoso intraoperatorio
Il Linfonodo Sentinella in Chirurgia: Attualità e Prospettive Direttore: Prof. A. Liboni 20 gennaio 2012 Ferrara, ITALY Il monitoraggio nervoso intraoperatorio Gianlorenzo Dionigi, MD, FACS Department of Surgical Sciences UNIVERSITY OF INSUBRIA (COMO – VARESE) - ITALY
 - ITALY.")
2
This report does not endorse any specific Company or set of monitoring equipment

3
Exposure of RLN reduce the rate of RLN injury
No identification RLN Localized RLN Partially exposed RLN Completely dissected RLN Lahey FH, Ann Surg Riddell VH, Lancet Jazko, Surgery % % Wagner, Br J Surg % % Hermann, Ann Surg, % % % % Dralle H, Surgery % % Chiang, Surgery % %

4
Gold standards for RLN management
Extensive knowledge of RLN anatomy Visual identification of RLN Exposure of RLN Experience & training Pre- & post-op. laryngoscopy

5
Why neuromonitoring? RLN and laryngeal anatomy are the basis of modern thyroid surgery Why do we need more than anatomical nerve identification?

6
Neuromonitoring: history
Laryngeal palpation with stimulation of RLN: feel for laryngeal twitch Riddell published in 1970, studies over Palpation of posterior crico-arytenoid muscle, with stimulation of mA Galivan 1986

7
Evolution of RLN Monitoring
Intra-operative invasive techniques Non-invasive surface electrodes Lamadé W Transtracheal monitoring of the recurrent laryngeal nerve. Prototype of a new tube Intraoperative monitoring of the recurrent laryngeal nerve. A new method Chirurg & 1997

8
ETT ETT electrodes Stimulator probe NIM monitor

9
RLN identified both visually and electrically

10
Intraoperative evidence of RLN injury
Evidence RLN injury Author Reference N % Bergenfelz A Langenbecks Arch Surg / % Chiang FY Surgery / % Lo CY Arch Surg /33 15% Patlow CA Ann Surg /10 10% Caldarelli D Otolaryngol Clin North Am /10 10% Scandinavian Quality Register Thyroid Surgery

11
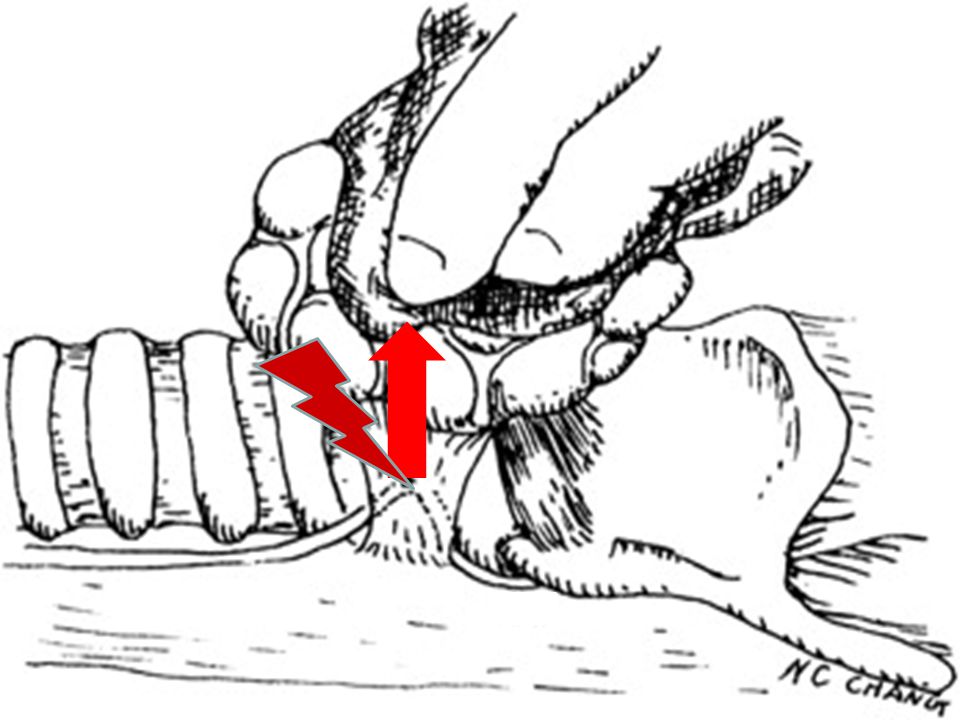
After transection of the artery, a disrupted point was detected on the nerve. Above this point, the EMG signal was normal. So, not only the Berry’s ligament but also a crossing artery can cause a type 1 stretch injury.

12
After complete nerve dissection, R2 and V2 signals were lost
After complete nerve dissection, R2 and V2 signals were lost. No disrupted point could be detected on the exposed nerve. Before closing the wound I retest the nerve. R2 and V2 signal did not recover, and the patient developed temporary palsy.

14
Intraoperative RLN injury causes
Section (mistake in surgical technique) Ligature (without transection) Mistake in hemostasis and dissection maneuvers Stretch/traction Excessive traction during the medial traction of the thyroid lobe Excessive aspiration near to the nerve (suction) Compression/contusion/pressure Thermal/electrical injury Diffusion by haemostatic devices Ischemia Ligation of the inferior pole vessels before identifying RLN Excessive dissection of the nerve with ischemia
 Ligature (without transection) Mistake in hemostasis and dissection maneuvers. Stretch/traction. Excessive traction during the medial traction of the thyroid lobe. Excessive aspiration near to the nerve (suction) Compression/contusion/pressure. Thermal/electrical injury. Diffusion by haemostatic devices. Ischemia. Ligation of the inferior pole vessels before identifying RLN. Excessive dissection of the nerve with ischemia.")
15
Types of nerve injury neuropraxia: simple contusion of a nerve
treated by simple observation return to normal function over weeks to months axonotmesis: more significant disruption followed by degeneration healing takes a prolonged time neurotmesis: complete division of a nerve requires surgical repair

16
anatomical nerve lesions are only exceptional reasons for postop VC palsy
Dralle H. WJS 2008 Bergenfelz A . Langenbecks Arch Surg 2008 Chiang FY . Surgery 2005 Lo CY . Arch Surg 2000 Patlow CA . Ann Surg 1986 Caldarelli D. Otolaryngol Clin North Am 1980

17
AUDIT True incidence of RLN injury
No routine post-operative laryngoscopy 0.3% RLNP Routine postoperative laryngeal exams 7% RLNP

18
1. Evidence from the Literature (?)
Transient RLN palsy Permanent RLN palsy Parameter Odds ratio P value Odds ratio P value Graves’ disease < <0.37 Recurrent goiter < <0.0001 Thyroiditis < <0.92 Uninodular goiter* < <0.51 IONM < <0.004 Am J Surg 2002

19
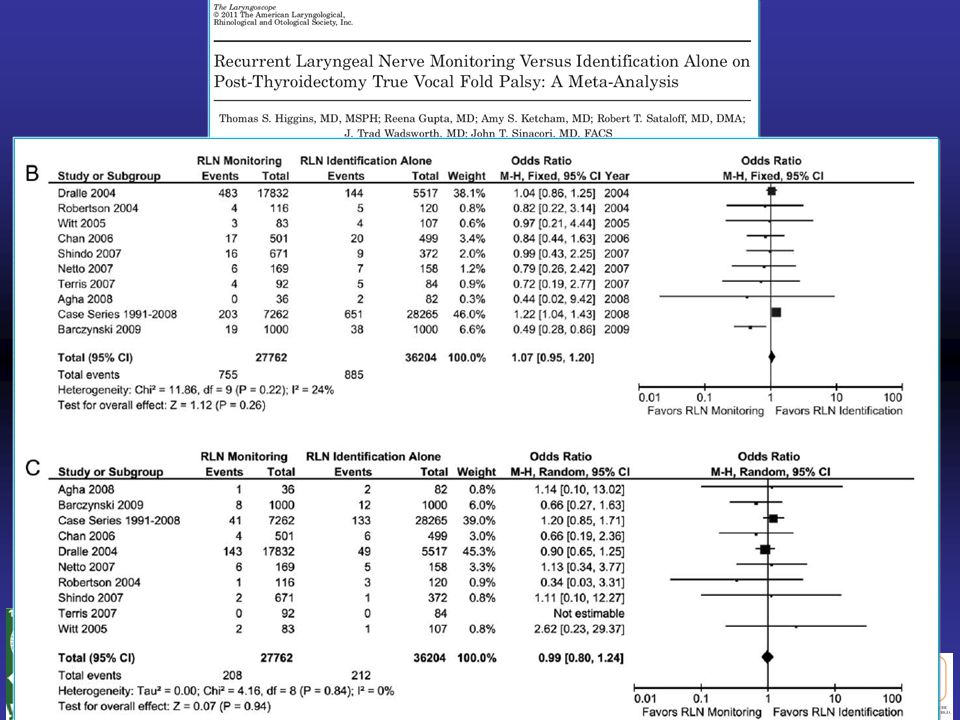
2. Evidence from the Literature (?)
")
21
Dralle H, WJS 2008

22
Reasons for RLN protection with IONM
Adds early and definite localization of RLN To prevent visual misidentification To avoid excessive traction To identify extralaryngeal branches, anatomical variation, distored RLN, non-RLN Adds confirmation of RLN Adds dissection of RLN

23
Nerve Identification 2mA

24
Nerve Confirmation 1-0.5mA

25
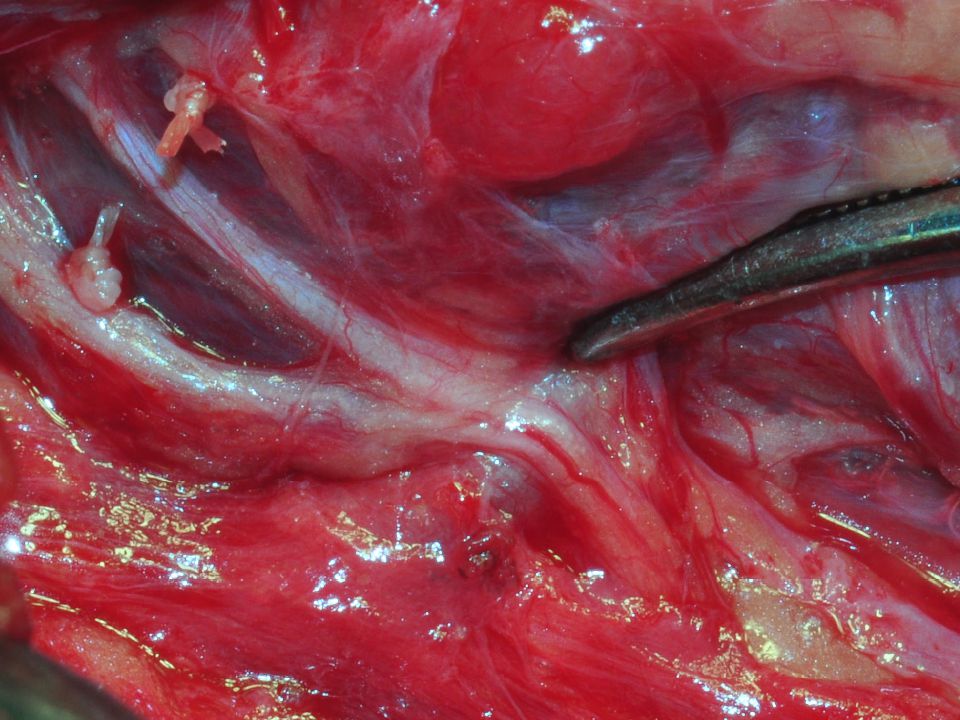
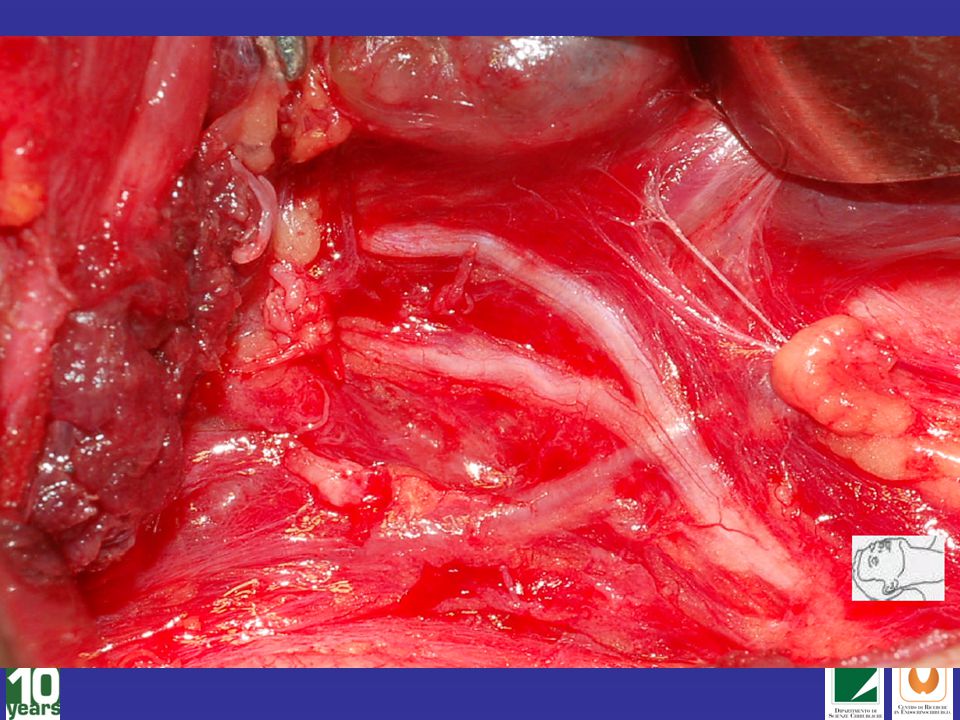
In this case, it seems hard to tell which is the nerve, which is the vessel.
With the application of neuromonitoring, it is easy to identify the anterior motor branch, posterior sensory branch, and the vessels. Nerve Confirmation 0.5mA 25

29
The answer is very simple: based on anatomical nerve assessment alone 1. the frequency of postop VC dysfunction is more common than expected 2. because anatomical nerve lesions are only exceptional reasons for postop VC palsy Why neuromonitoring?

30
Which is the fundamental difference
between visual identification and RLN monitoring? RLN monitoring can change strategy

31
Strategy changes in bilateral goiter
36 LOS at first side 16 unchanged strategy ↓ 9 (56%) unilateral palsy 3 (19%) bilateral palsy 20 changed strategy ↓ 20 (100%) unilateral palsy 0 bilateral palsy
 unilateral palsy. 3 (19%) bilateral palsy. 20 changed strategy. ↓ 20 (100%) unilateral palsy. 0 bilateral palsy.")
32
How to treat RLN injury intraoperatively?
When LOS is real: How to treat RLN injury intraoperatively? Intraop steroids* (n=143) No intraop steroids (n=152) NAR Vocal corde palsy temporary permanent 12 Recovery (days) 28.6 (10-36) (14-61)**
 No intraop steroids. (n=152) NAR. Vocal corde palsy temporary. permanent Recovery (days) 28.6 (10-36) 37.4 (14-61)**")
34
MEDICO-LEGAL ISSUES Reduction of major injury to patient
Bilateral RLN palsy Recorded nerve signal Early differentiation between RLN related and unrelated voice changes New standard of care (?)
")
35
US thyroid surgery monitored

36
IONM procedures in Asia
Chiang FY, 2011 IONM procedures in Asia

37
IONM PREVALENCE IN EUROPE
Danmark 77% Godballe C, ETA Meeting, Lisbona, Poland 5% Barcinsky M, Polish Endocrine Surgeons Germany 90% Dralle H, Harvard Meeting, Boston France # Carnaille B, IONM study group France # Carnaille B, IONM study group Spain # Manuel Poveda, Madrid 2010 Spain # Jan-april Manuel Poveda, Madrid 2011

38
PREVALENCE IN ITALY source Medtronic Italy

39
http://www.dgch.de German Association of Endocrine Surgeons
Langenbecks Arch Surg 2011;396(5): Darstellung des Nervus laryngeus recurrens Funktionsstörungen des Nervus laryngeus recurrens sind mit Stimmstörungen, Schluckstörungen und Beeinträchtigungen der Atmung verbunden. Bei bilateraler Rekurrensparese ist häufig eine Tracheotomie erforderlich. Das Risiko, den N. laryngeus recurrens zu verletzen, wird durch das Ausmaß der Resektion und die individuelle Lagevariante des Nerven bestimmt. Die schonende, das heißt nicht-skelettierende, nervendurchblutungserhaltende präparative Darstellung des N. laryngeus recurrens mindert das Schädigungsrisiko und sollte grundsätzlich sowohl bei Primäreingriffen als auch bei Rezidiveingriffen durchgeführt werden (6, 18). Der visualisierte anatomische Nervenverlauf sollte vor und nach Resektion dokumentiert werden. Ausnahmsweise kann auf die Darstellung verzichtet werden, wenn sich die Resektionsebene in sicherem Abstand ventral der lateralen Grenzlamelle zum Nervenverlauf befindet (46). Die Nichtdarstellung des Nervus laryngeus recurrens soll begründend dokumentiert werden. Das intraoperative Neuromonitoring ersetzt nicht den Goldstandard der visuellen Nervendarstellung, sondern ist nur in Ergänzung zu dieser einsetzbar. Das Verfahren kann die Identität des Nervus laryngeus recurrens sicher bestätigen und seine Funktionsfähigkeit bei ungestörtem Überleitungssignal sehr wahrscheinlich machen, wobei zur Erfassung des gesamten Nervenverlaufes die Stimulation über den Nervus vagus vor und nach Resektion erforderlich ist (10, 17, 28, 48, 50). Die sicherste Methode zur Differenzierung zwischen Artefakten und Aktionspotenzialen ist die Ableitung von Elektromyogrammen. Eine signifikante Senkung des Rekurrenspareserisikos durch Einsatz des Neuromonitoring ist bislang nur bei Rezidiveingriffen gesichert (9, 28).
: Darstellung des Nervus laryngeus recurrens Funktionsstörungen des Nervus laryngeus recurrens sind mit Stimmstörungen, Schluckstörungen und Beeinträchtigungen der Atmung verbunden. Bei bilateraler Rekurrensparese ist häufig eine Tracheotomie erforderlich. Das Risiko, den N. laryngeus recurrens zu verletzen, wird durch das Ausmaß der Resektion und die individuelle Lagevariante des Nerven bestimmt. Die schonende, das heißt nicht-skelettierende, nervendurchblutungserhaltende präparative Darstellung des N. laryngeus recurrens mindert das Schädigungsrisiko und sollte grundsätzlich sowohl bei Primäreingriffen als auch bei Rezidiveingriffen durchgeführt werden (6, 18). Der visualisierte anatomische Nervenverlauf sollte vor und nach Resektion dokumentiert werden. Ausnahmsweise kann auf die Darstellung verzichtet werden, wenn sich die Resektionsebene in sicherem Abstand ventral der lateralen Grenzlamelle zum Nervenverlauf befindet (46). Die Nichtdarstellung des Nervus laryngeus recurrens soll begründend dokumentiert werden. Das intraoperative Neuromonitoring ersetzt nicht den Goldstandard der visuellen Nervendarstellung, sondern ist nur in Ergänzung zu dieser einsetzbar. Das Verfahren kann die Identität des Nervus laryngeus recurrens sicher bestätigen und seine Funktionsfähigkeit bei ungestörtem Überleitungssignal sehr wahrscheinlich machen, wobei zur Erfassung des gesamten Nervenverlaufes die Stimulation über den Nervus vagus vor und nach Resektion erforderlich ist (10, 17, 28, 48, 50). Die sicherste Methode zur Differenzierung zwischen Artefakten und Aktionspotenzialen ist die Ableitung von Elektromyogrammen. Eine signifikante Senkung des Rekurrenspareserisikos durch Einsatz des Neuromonitoring ist bislang nur bei Rezidiveingriffen gesichert (9, 28).")
40
Polish Journal of Surgery (transl)
Polish Journal of Surgery (transl). Guideline Statement of the Polish Study Group for Nerve Monitoring of the Polish Club of the Endocrine Surgeons Members of the Study Group for Nerve Monitoring of the Polish Club of Endocrine Surgery during the conference on 16th of April 2011 in Krakow opine that centers of thyroid surgery in Poland should be equipped with nerve integrity monitoring systems. Following the analysis of the published data and based on our own experience the need to introduce routine training courses of standardized technique of electrophysiological monitoring of the recurrent nerves and employment of this technique in selected thyroid operations was recognized".
. Guideline Statement of the Polish Study Group for Nerve Monitoring of the Polish Club of the Endocrine Surgeons. Members of the Study Group for Nerve Monitoring of the Polish Club of Endocrine Surgery during the conference on 16th of April 2011 in Krakow opine that centers of thyroid surgery in Poland should be equipped with nerve integrity monitoring systems. Following the analysis of the published data and based on our own experience the need to introduce routine training courses of standardized technique of electrophysiological monitoring of the recurrent nerves and employment of this technique in selected thyroid operations was recognized .")
41
Neuromonitoring for residents in surgical training
Incorporating new technology Teaching aid Elucidate errors Less-experienced surgeons IONM decrease RLN paralysis (Dralle H, 2004)
")
42
LIMITATIONS OF IONM RLN palsy still occur
need for standardized and well-trained use to avoid pitfalls knowledge of most-common pitfalls ability to use troubleshooting algorithms IONM does not replace clinical judgment relatively low positive predictive value cost-effectiveness is still not evaluated need for further research focused on neurophysiology of the RLNs IONM of the external branch of the superior laryngeal nerve thyroidectomy in local anesthesia

43
Conclusions

44
Why should RLN be monitored in any bilateral case ?
RLN monitoring improves Nerve ID (Randolph GW, 2002) Clarification of RLN anatomy (Delbridge 2002) Nerve dissection (Chan WF 2006) Reoperations with pre-existing RLN morbidity (Gorentzy P, 2008) Intraoperative assessment of RLN function (non postoperative) Intraoperative prediction of post-operative function (prognosis) (Timmermann W, 2004) Prevention of bilateral RLN injury: “one-stage thyroidectomy” (Randolph GW, 2002) Elucidate where and how the RLN was injured (intraoperative evidence) (Chan WF 2006) Early differentiation between RLN related and unrelated voice changes (Dralle H 2004)
 Clarification of RLN anatomy (Delbridge 2002) Nerve dissection (Chan WF 2006) Reoperations with pre-existing RLN morbidity (Gorentzy P, 2008) Intraoperative assessment of RLN function (non postoperative) Intraoperative prediction of post-operative function (prognosis) (Timmermann W, 2004) Prevention of bilateral RLN injury: one-stage thyroidectomy (Randolph GW, 2002) Elucidate where and how the RLN was injured (intraoperative evidence) (Chan WF 2006) Early differentiation between RLN related and unrelated voice changes (Dralle H 2004)")
45
IONM technology in thyroid surgery
(IONM: intraoperative neuromonitoring) IMPLICATIONS CLINICAL PRACTICE RESEARCH EDUCATION MEDICO-LEGAL
 IMPLICATIONS. CLINICAL PRACTICE. RESEARCH. EDUCATION. MEDICO-LEGAL.")
46
Surgeons should not overstate benefits of neuromonitoring to patients

47
Modern Surgery ERADICATION OF DISEASE SAFETY OF PROCEDURE
DOCUMENTATION

Ähnliche Präsentationen