Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Endokrinologie und Psyche Aus der Sicht des Endokrinologen
Bruno Müller Endokrinologie und Diabetologie FMH Bern

2
Website Bruno Müller

3
‚kränkeln‘ die Hormone, weil es uns schlecht geht?
Oder: geht es uns schlecht, weil die Hormone ‚kränkeln‘?

4
„Nun sag, wie hast du’s mit der Religion?“
Die berühmte Gretchenfrage!

5
Inhalte – key points Grundlagen (Endokrinologie)
(physischer) Stress / psychiatrische Erkrankung endokrines System Endokrinologisch relevante NW einer Neuroleptika-Therapie Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung
 Stress / psychiatrische Erkrankung endokrines System. Endokrinologisch relevante NW einer Neuroleptika-Therapie. Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung.")
6
Inhalte – key points Grundlagen (Endokrinologie)
(physischer) Stress / psychiatrische Erkrankung endokrines System Endokrinologisch relevante NW einer Neuroleptika-Therapie Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung
 Stress / psychiatrische Erkrankung endokrines System. Endokrinologisch relevante NW einer Neuroleptika-Therapie. Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung.")
7
- + SUMMARY OF HORMONE PHYSIOLOGY Higher Centers Pituitary Liver
Neural activity (neurotransmitters) Hypothalamus Releasing Factors Pituitary posterior anterior Trophic Hormones LH FSH ACTH TSH Liver Fat Thyroid GH Peripheral Hormones IGF-I - Adrenal + Bone Cartilage Muscle Testis Ovary Gonads
 Hypothalamus. Releasing Factors. Pituitary. posterior. anterior. Trophic. Hormones. LH. FSH. ACTH. TSH. Liver. Fat. Thyroid. GH. Peripheral. Hormones. IGF-I. - Adrenal. + Bone. Cartilage. Muscle. Testis. Ovary. Gonads.")
8
T4 80% T3 20% aktives Hormon Konversion zu T3 peripher
SUMMARY OF HORMONE PHYSIOLOGY Higher Centers Neural activity (neurotransmitters) Hypothalamus Releasing Factors Pituitary posterior anterior Trophic Hormones LH FSH ACTH TSH Thyroid T4 80% T3 20% aktives Hormon Konversion zu T3 peripher
 Hypothalamus. Releasing Factors. Pituitary. posterior. anterior. Trophic. Hormones. LH. FSH. ACTH. TSH. Thyroid. T4 80% T3 20% aktives Hormon. Konversion. zu T3 peripher.")
9
Control of androgen secretion

10
Inhalte – key points Grundlagen (Endokrinologie)
(physischer) Stress / psychiatrische Erkrankung endokrines System Endokrinologisch relevante NW einer Neuroleptika-Therapie Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung
 Stress / psychiatrische Erkrankung endokrines System. Endokrinologisch relevante NW einer Neuroleptika-Therapie. Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung.")
14
- - -

15
- -

16
- -

17
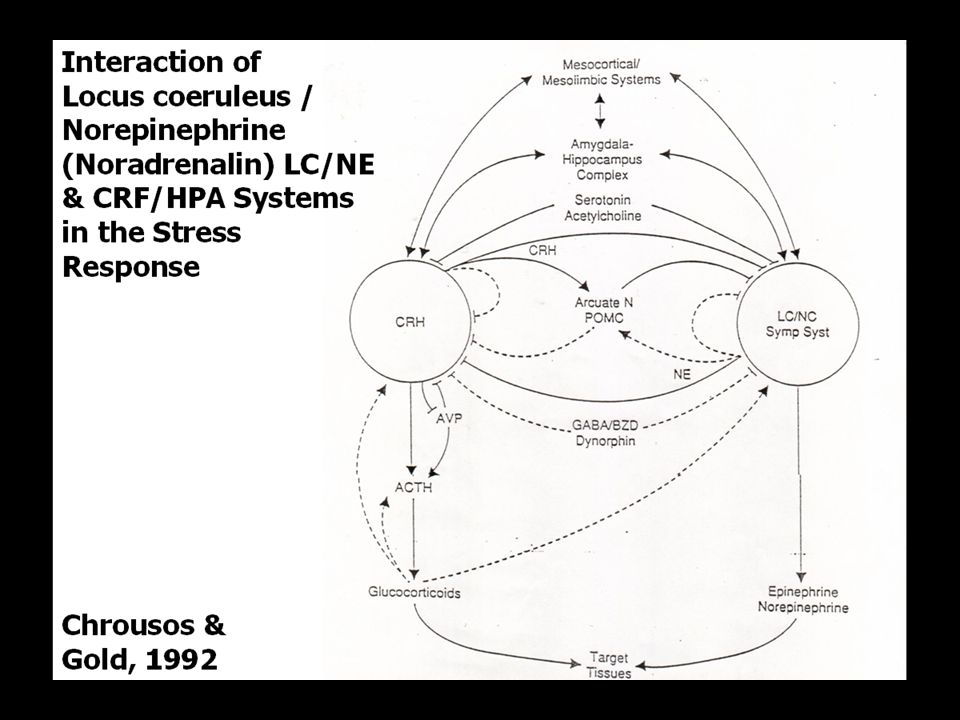
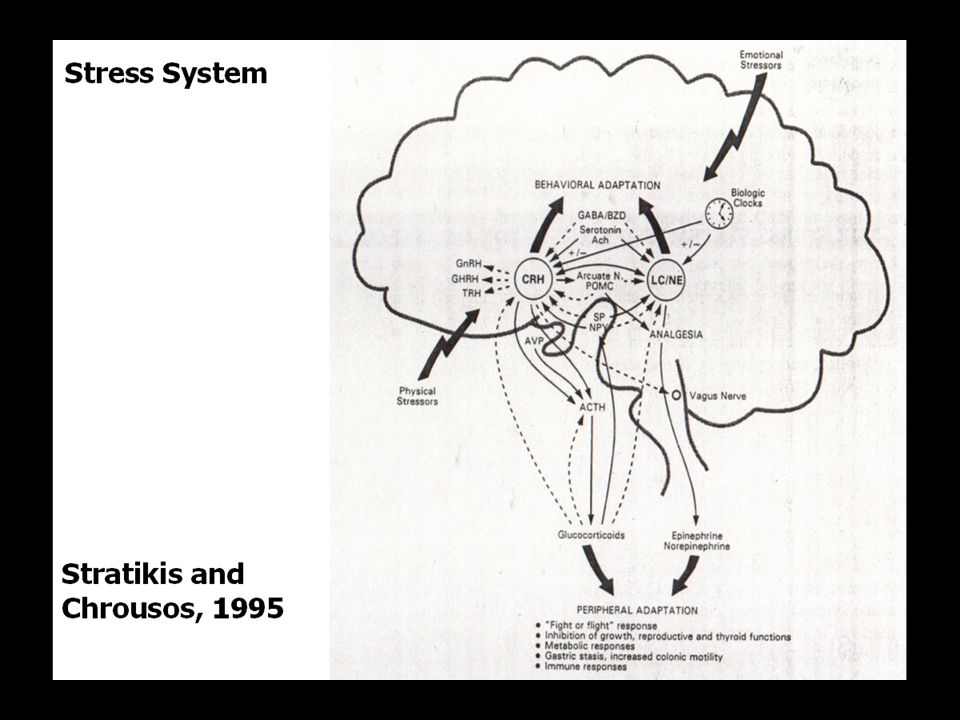
(physischer) Stress / Depressionen und endokrines System, Zusammenfassung
(physischer) Stress führt zu Arousal der CRF-HPA-Achse vermehrter Cortisol-Produktion sekundärem Abfall von Testosteron und Wachstumshormon Verminderter Produktion (d. Konversion) von aktivem Schilddrüsen-Hormon T3
 Stress führt zu. Arousal der CRF-HPA-Achse. vermehrter Cortisol-Produktion. sekundärem Abfall von Testosteron. und Wachstumshormon. Verminderter Produktion (d. Konversion) von aktivem Schilddrüsen-Hormon T3.")
18
Inhalte – key points Grundlagen (Endokrinologie)
(physischer) Stress / psychiatrische Erkrankung endokrines System Endokrinologisch relevante NW einer Neuroleptika-Therapie Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung
 Stress / psychiatrische Erkrankung endokrines System. Endokrinologisch relevante NW einer Neuroleptika-Therapie. Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung.")
19
Optimale Wahl eines Antipsychotikums unter Abwägung der beiden wichtigsten Parameter « Wirksamkeit und Verträglichkeit » Optimale Wahl Verträglichkeit -> Risiken Wirksamkeit -> Nutzen Version 4 27 July 06

20
Antipsychotika: Nebenwirkungsprofil
Falkai et al., WFSBP Guidelines, 2005

21
Antipsychotika: Nebenwirkungsprofil
Falkai et al., WFSBP Guidelines, 2005

22
Schizophrenie: Langzeitbehandlung
CATIE: Nebenwirkungen

23
Neuroleptika SGA: Monitoring
WFSBP, 2005

24
Inhalte – key points Grundlagen (Endokrinologie)
(physischer) Stress / psychiatrische Erkrankung endokrines System Endokrinologisch relevante NW einer Neuroleptika-Therapie Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung
 Stress / psychiatrische Erkrankung endokrines System. Endokrinologisch relevante NW einer Neuroleptika-Therapie. Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung.")
25
Inhalte – key points Grundlagen (Endokrinologie)
(physischer) Stress / psychiatrische Erkrankung endokrines System Endokrinologisch relevante NW einer Neuroleptika-Therapie Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung
 Stress / psychiatrische Erkrankung endokrines System. Endokrinologisch relevante NW einer Neuroleptika-Therapie. Gewichtszunahme / Diabetes / Hyperprolaktinämie / Zusamenfassung.")
26
Inhalte – key points Gewichtszunahme / Diabetes / Hyperprolaktinämie

27
Hintergrund « natürliche Todesursachen » und nicht Suizid sind der Hauptgrund für die erhöhte Mortalität von Pat. mit Schizophrenie oder bipolaren Störungen 1 bereits vor Entdeckung der Neuroleptika waren Verbindungen zwischen Schizophrenie und Diabetes beschrieben worden 2 man schätzt die Prävalenz von Diabetes m. bei schizophrenen Pat. als 3-4 mal und bipolaren Pat. als 2-4 mal höher verglichen mit der Normalbevölkerung 3 retrospektive Daten bei behandlungsnaiven Patienten deuten auf eine pathologische Glukosetoleranz bereits vor Antipsychotikatherapie hin 4 ⇒ Schizophrenie als möglicher unabhängiger Risikofaktor für Diabetes 3 1 Brown et al., Causes of the excess mortality of schizophrenia. British Journal of Psychoiatry, 2000, 177, 2 Maudsley, H,The Pathology of Mind (3rd edn), 1879, London: Macmillan 3 Bushe et al, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia. British Journal of Psychiatry, 2004, 184, 67-71 4 Thakore J.H., Metabolic disturbance in first-episode schizophrenia. British Journal of Psychiatry, 2004, 184, 76-79 File name/location Company Confidential Copyright © 2000 Eli Lilly and Company
, 1879, London: Macmillan. 3 Bushe et al, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia. British Journal of Psychiatry, 2004, 184, Thakore J.H., Metabolic disturbance in first-episode schizophrenia. British Journal of Psychiatry, 2004, 184, File name/location. Company Confidential. Copyright © 2000 Eli Lilly and Company.")
28
Mögliche Ursachen Genetik: Schizophrene haben signifikant häufiger eine positive Familienanamnese für Diabetes m. 1 Stress: metabolische Störungen als Folge eines chronisch erhöten Kortisolspiegels 2 Medikation: Hyperprolaktinämie kann zu Insulinresistenz führen, Einflüsse durch Gewichtszunahme (Datenlage jedoch uneinheitlich) 3 Lebensführung: Essverhalten (Fett↑, Ballaststoffe↓), Bewegung↓,Rauchen, Armut, instabile Lebensbedingungen, niedrigerer Ausbildungsgrad 1 1 Bushe et al, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia. British Journal of Psychiatry, 2004, 184, 67-71 2 Dinan T.G., Stress and the genesis of diabetes mellitus in schizophrenia. British Journal of Psychiatry, 2004, 184, 72-75 3 Bushe et al, Association between atypical antipsychotic agents and type 2 diabetes: review of prospective clinical data. British Journal of Psychiatry, 2004, 184, 87-93 File name/location Company Confidential Copyright © 2000 Eli Lilly and Company
 3. Lebensführung: Essverhalten (Fett↑, Ballaststoffe↓), Bewegung↓,Rauchen, Armut, instabile Lebensbedingungen, niedrigerer Ausbildungsgrad 1. 1 Bushe et al, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia. British Journal of Psychiatry, 2004, 184, Dinan T.G., Stress and the genesis of diabetes mellitus in schizophrenia. British Journal of Psychiatry, 2004, 184, Bushe et al, Association between atypical antipsychotic agents and type 2 diabetes: review of prospective clinical data. British Journal of Psychiatry, 2004, 184, File name/location. Company Confidential. Copyright © 2000 Eli Lilly and Company.")
29
Prävalenz des Diabetes bei Schizophrenie und bipolaren Störungen
Die Prävalenz des Typ-2-Diabetes kann: bei Patienten mit Schizophrenie mindestens x höher sein als in der Allgemeinbevölkerung17,18,19 bei Patienten mit bipolaren Störungen mindestens x höher sein als in der Allgemeinbevölkerung17,19,20 17. Keskiner A et al. Psychosomatics 1973; 14: , 18. Mukherjee S et al. Compr Psychiatry 1996; 37: 68-73 19. Ryan MC, Impaired fasting glucose tolerance in first-episode, drug-naive patients with schizophrenia. Am J Psy 2003, 160, 20. Cassidy F et al. Am J Psy 1999; 156: Version 4 27 July 06

30
Prävalenz des Diabetes bei Schizophrenie und bipolaren Störungen
Schizophrenie (und möglicherweise auch bipolare Störungen) kann als unabhängiger Risikofaktor für die Entstehung eines Diabetes angesehen werden.21 Referenz: 1. Ryan MC & Thakore JH, Physical consequences of schizophrenia and its treatment: the metabolic syndrome. Life Sciences 2002, 71, 21. Dinan TG, British J Psy 2004, 184 (suppl 47):s53-s54 Version 4 27 July 06
 kann als unabhängiger Risikofaktor für die Entstehung eines Diabetes angesehen werden.21. Referenz: 1. Ryan MC & Thakore JH, Physical consequences of schizophrenia and its treatment: the metabolic syndrome. Life Sciences 2002, 71, Dinan TG, British J Psy 2004, 184 (suppl 47):s53-s54. Version 4 27 July 06.")
31
Lebensgewohnheiten bei psychiatrischen Patienten
Viele Patienten mit Schizophrenie : ernähren sich weniger gesund (allgemein zu viel Fett und zu wenig Ballaststoffe) machen weniger Sport rauchen mehr leben in ärmeren und instabileren Verhältnissen haben einen niedrigeren und einen niedriger als erwarteten Bildungsabschluss … als die Allgemeinbevölkerung!22 Referenzen cité dans Bushe C, Holt R, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia, BJP 2004, 184(suppl 47):s67 Brown S, The unhealthy lifestyle of people with schizophrenia. Psychological Medicine 1999, 29, Dixon L, Prevalence and correlates of diabetes in national schizophrenia samples. Schizophrenia Bulletin 2000, 26, 22. Bushe C, Holt R, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia, British J Psy 2004, 184 (suppl47):s67-s71 Version 4 27 July 06
 machen weniger Sport. rauchen mehr. leben in ärmeren und instabileren Verhältnissen. haben einen niedrigeren und einen niedriger als erwarteten Bildungsabschluss. … als die Allgemeinbevölkerung!22. Referenzen cité dans Bushe C, Holt R, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia, BJP 2004, 184(suppl 47):s67. Brown S, The unhealthy lifestyle of people with schizophrenia. Psychological Medicine 1999, 29, Dixon L, Prevalence and correlates of diabetes in national schizophrenia samples. Schizophrenia Bulletin 2000, 26, Bushe C, Holt R, Prevalence of diabetes and impaired glucose tolerance in patients with schizophrenia, British J Psy 2004, 184 (suppl47):s67-s71. Version 4 27 July 06.")
32
Intra-abdominelles Fett
Übergewicht und intra-abdominales Fett Nicht mit Arzneimitteln therapierte Patienten (Drug free patients) mit Schizophrenie haben: einen höheren BMI als die Allgemeinbevölkerung20 chronisch erhöhte Cortisol-Spiegel (die Psychose induziert Stress) resultierend in 3.4 x mehr intra-abdominellem Fett im Vergleich zu gesunden Probanden.23 Intra-abdominelles Fett Referenz: Thakore JH, Metabolic disturbance in first-episode schizophrenia, British J Psy 2004, 184 (suppl 47), s76-s79 23. Thakore JH et al., Brit J Psy 2004; 184 (suppl 47): s76-s79 Version 4 27 July 06
 mit Schizophrenie haben: einen höheren BMI als die Allgemeinbevölkerung20. chronisch erhöhte Cortisol-Spiegel (die Psychose induziert Stress) resultierend in 3.4 x mehr intra-abdominellem Fett im Vergleich zu gesunden Probanden.23. Intra-abdominelles Fett. Referenz: Thakore JH, Metabolic disturbance in first-episode schizophrenia, British J Psy 2004, 184 (suppl 47), s76-s Thakore JH et al., Brit J Psy 2004; 184 (suppl 47): s76-s79. Version 4 27 July 06.")
33
Intra-abdominelles Fett
Schizophrenie und abdominales Fett Abdominelle CT Ergebnisse bei nicht mit Arzneimitteln therapierten Patienten (Drug free patients) 40,000 35,000 Schizophrenie (n = 15) Kontrollgruppe (n = 15) 30,000 *P < 0,005 Fett2 (mm) 25,000 20,000 15,000 * 10,000 7 patients were drug-naive and 8 had not taken any antipsychotic for at least 6 weeks (and 6 months for IM) in the schizo group. Meme proportion de graisse mais 3 à 4 fois plus de graisse intra-abdominale dans le groupe schizo. Cela semble être corrélé avec une augmentation chronique du taux de cortisol localisé au niveau intra-abdominal. 5000 Körperfett gesamt Subkutanes Fett Intra-abdominelles Fett 24. Thakore JH et al., Int J Obes Relat Metab Disord. 2002; 26: Version 4 27 July 06
 40, ,000. Schizophrenie (n = 15) Kontrollgruppe (n = 15) 30,000. *P < 0,005. Fett2 (mm) 25, , ,000. * 10, patients were drug-naive and 8 had not taken any antipsychotic for at least 6 weeks (and 6 months for IM) in the schizo group. Meme proportion de graisse mais 3 à 4 fois plus de graisse intra-abdominale dans le groupe schizo. Cela semble être corrélé avec une augmentation chronique du taux de cortisol localisé au niveau intra-abdominal Körperfett gesamt. Subkutanes Fett. Intra-abdominelles Fett. 24. Thakore JH et al., Int J Obes Relat Metab Disord. 2002; 26: Version 4 27 July 06.")
34
Früherkennung bei Patienten mit erhöhtem Risiko
Bei Patienten mit Schizophrenie24 oder bipolaren Störungen25, die mit Olanzapin therapiert wurden, ist eine frühe Gewichtzunahme ein Prädiktor für eine langfristige Gewichtzunahme. Zyprexa® Dosierung = 5-20 mg/Tag Selon dr. Ineichen, mettre accent sur le fait que 85% ne prennent pas de poids –substantiel- et = aux autres antipsychotiques. Cette étude montre que 15% de patients sous Zyprexa ont eu une augm. Poids significative. Que faire ??? Key points: It is possible to identify patients who have substantial weight gain early in treatment by their greater propensity to gain weight rapidly. Clinically speaking, if patients gain 2-4lbs within 2 weeks then an intervention should be considered. Thus by measuring the weight of patients during the first few weeks of olanzapine treatment and by assessing changes in appetite, clinicians may be able to identify who is likely to gain weight rapidly. Early identification of patients with rapid weight gain and intervention with behavioral and pharmacologic methods may be effective in limiting overall weight gain. Background: A retrospective analysis of weight gain was performed for 1191 patients diagnosed with schizophrenia or schizoaffective disorder who were treated with olanzapine over a 52-week treatment period (1191/1336 patients had sufficient data and were included in the analysis; average olanzapine dose was 13.2 mg). Patients were dichotomized into two main groups according to the percentage of body weight gained during the first 6 weeks of treatment with olanzapine: 1) patients who gained greater than or equal to 7% of their body weight within the first 6 weeks of treatment (Rapid Weight Gain Group, RWG), and 2) patients who lost weight, gained no weight or gained less than 7% of their body weight during the first 6 weeks of treatment (Non-Rapid Weight Gain Group, NRWG). Results demonstrated that approximately 15% of the patient population showed rapid increases in weight (RWG group) while 85% of patients gained weight more slowly or not at all (NRWG group). Patients in the RWG group gained >2% of their body weight (approximately 4-7 pounds) within the first two weeks of treatment with olanzapine and were more likely to report an increase in appetite as compared to patients in the NRWG group. Furthermore, patients who gained weight more rapidly during treatment with olanzapine also showed more robust clinical improvement in psychopathology. Reference: Kinon BJ, Kaiser CJ, Ahmed S, Rotelli M, Kollack-Walker S. Association Between Early and Rapid Weight Gain and Change in Weight Over One Year of Olanzapine Therapy in Patients with Schizophrenia and Related Disorders. Journal of Clinical Psychopharmocology ; 25(3): Jones B, Basson BR, Walker DJ, Crawford AMK, Kinon BJ. Weight change and atypical antipsychotic treatment in patients with schizophrenia. Journal of Clinical Psychiatry ; 62(suppl 2):41-44. 25. Kinon BJ et al., J Clin Psychopharmacol 2005; 25(3): 26. Hennen et al., J Clin Psy 2004; 65: Version 4 27 July 06
. Patients were dichotomized into two main groups according to the percentage of body weight gained during the first 6 weeks of treatment with olanzapine: 1) patients who gained greater than or equal to 7% of their body weight within the first 6 weeks of treatment (Rapid Weight Gain Group, RWG), and 2) patients who lost weight, gained no weight or gained less than 7% of their body weight during the first 6 weeks of treatment (Non-Rapid Weight Gain Group, NRWG). Results demonstrated that approximately 15% of the patient population showed rapid increases in weight (RWG group) while 85% of patients gained weight more slowly or not at all (NRWG group). Patients in the RWG group gained >2% of their body weight (approximately 4-7 pounds) within the first two weeks of treatment with olanzapine and were more likely to report an increase in appetite as compared to patients in the NRWG group. Furthermore, patients who gained weight more rapidly during treatment with olanzapine also showed more robust clinical improvement in psychopathology. Reference: Kinon BJ, Kaiser CJ, Ahmed S, Rotelli M, Kollack-Walker S. Association Between Early and Rapid Weight Gain and Change in Weight Over One Year of Olanzapine Therapy in Patients with Schizophrenia and Related Disorders. Journal of Clinical Psychopharmocology. 2005; 25(3): Jones B, Basson BR, Walker DJ, Crawford AMK, Kinon BJ. Weight change and atypical antipsychotic treatment in patients with schizophrenia. Journal of Clinical Psychiatry. 2001; 62(suppl 2): Kinon BJ et al., J Clin Psychopharmacol 2005; 25(3): Hennen et al., J Clin Psy 2004; 65: Version 4 27 July 06.")
35
Woche 4 Woche 8 Woche 12 Woche 16 Woche 20 Woche 24 Woche 32 Woche 48
Durchschnittliche Gewichtszunahme Olanzapin Risperidon x = signifikanter Unterschied Gewichtszunahme (Kg) Baseline Woche 4 Woche 8 Woche 12 Woche 16 Woche 20 Woche 24 Woche 32 Woche 48 10. Alvares E et al., J Clin Psychopharmacol, 2006; 26: Version 4 27 July 06
 Baseline. Woche 4 Woche 8 Woche 12 Woche 16 Woche 20 Woche 24 Woche 32 Woche Alvares E et al., J Clin Psychopharmacol, 2006; 26: Version 4 27 July 06.")
36
Inhalte – key points Gewichtszunahme / Diabetes / Hyperprolaktinämie

37
Anatomie Dopamin PIF Prolactin inhibiting factor

38
Anatomie TRH

39
Physiologie Peptidhormon (198AS) Homologie mit GH
Neg. Regulation durch Dopamin Anstieg während des Schlafes, Peaks PRL-Rezeptoren sind weit verteilt (Funktion??) Mamma = physiolog. 1° Zielorgan (Differenzierung, Laktation)
 Mamma = physiolog. 1° Zielorgan (Differenzierung, Laktation)")
40
Indikationen für Diagnostik
Zyklusstörungen / Amenorrhoe bei der Frau Galaktorrhoe Gynäkomastie Libido- und Potenzverlust (männlicher Hypogonadismus) Raumforderung im Sellabereich
 Raumforderung im Sellabereich.")
41
Prolaktin-Erhöhung Physiologisch Schwangerschaft Stimulation Stress

42
Prolaktin: Stress (max. 40ng/mL)
")
43
Prolaktin-Erhöhung Physiologisch Schwangerschaft Stimulation Stress
Pathologisch Adenom ‚Hypertrophie‘ Hypothalam. bzw. hypophysäre Erkr. Medikamentös Hypothyreose ... Clearance reduziert Idiopathisch Labor ‚Big‘ Prolaktin Makroprolaktin

44
Prolaktin-Erhöhung Pathologisch Medikamentös ...

45
Medikamentös induzierte Hyperprolaktinämie
Neuroleptika SSRI Metoclopramid H2-Blocker Methyldopa, Reserpin Verapamil Östrogene

46
Tubero-infundibuläres dopaminerges System
Sel. Dopamin- Rezeptoren D2 Serotonin- Rezeptoren 5-HT2, u.a. Hypothalamus

47
Conclusion Ist NL-assoziierte Hyperprolaktinämie HP in der psych. Praxis ein relevantes Problem? Antwort: Ja. Rund 23% aller in einem Zeitraum von 16 Monaten in einer grossen Psych. Kinik hospitaliserten Patienten weisen zu irgendeinem Zeitpunkt der Hosp. Eine relevante (definiert als > 40 ng/mL) HP auf
 HP auf.")
48
Inhalte – key points Zusamenfassend: Vorgehen bei Neuroleptika und Diabetes

49
Therapie der behandelbaren metabolischen Faktoren:
Schlussfolgerung Therapie der behandelbaren metabolischen Faktoren: Monitoring metabolischer Parameter ⇒ rechtzeitige Therapie Veränderung der Lebensführung! Ref.: Gough et al, Diabetes and its prevention: pragmatic solutions for people with schizophrenia. British Journal of Psychiatry, 2004, 184, File name/location Company Confidential Copyright © 2000 Eli Lilly and Company

50
Guidelines (mod. nach Gough et Peveler)
Pat. ohne Diabetes, Therapiebeginn/Switch: Wahl des AP aufgrund der Wirksamkeit « Lifestyle- »beratung Basisuntersuchungen: Nüchtern-Glukose/Insulin, HDL, Triglyceride, HbA1c wenn pathologisch Überweisung zum Allgemeinarzt Ein Wechsel des Antipsychotikums ist meist nicht notwendig ! File name/location Company Confidential Copyright © 2000 Eli Lilly and Company

51
Guidelines (mod. nach Gough et Peveler)
Pat. ohne Diabetes, Erhaltungstherapie: « Lifestyle- »beratung Nüchtern-Glukose/Insulin, HDL, Triglyceride, HbA1c/Jahr Monitoring von typischen Hyperglykämiesymptomen File name/location Company Confidential Copyright © 2000 Eli Lilly and Company

52
Guidelines (Gough et Peveler)
Pat. mit Diabetes: Optimierung der Schizophrenietherapie Antidiabetische Therapie durch Diabetologen oder Allgemeinmediziner File name/location Company Confidential Copyright © 2000 Eli Lilly and Company

54
Neuroleptika SGA: Monitoring
WFSBP, 2005

Ähnliche Präsentationen