Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Hyponatriämie Sebastiano A.G. Lava Geriatrische Universitätsklinik,
Spitalnetz Bern, Zieglerspital, Bern 19. April 2010

2
Inhaltsverzeichnis Fall Relevanz Physiologie “body fluids metabolism”
Hyponatriämie Symptome Einteilung (“rationale”) Behandlung… SIADH-Th + SIADH-Ursachen Take home
 Behandlung… SIADH-Th + SIADH-Ursachen. Take home.")
3
Frau E., 30.1.1913 Einweisungsgrund: Sturz Fx ISG Probleme Medik.
Kardiopathie (valv., rhytm. und koronare) Niereninsuff. (schwer) Hyponatriämie Gangstörung mit Sturz Schambeinast-Fx links Pneumopathie Anämie (hyperchrom makrozyt.) Vit. D Mangel Makuladeg. bds Medik. ASS, β-Blocker, Nitro, Liquemin Torem, Laxoberon Atrovent, Ventolin Temesta, Trittico, … Pantozol, Motilium Morphin, Paracet.,
 Niereninsuff. (schwer) Hyponatriämie. Gangstörung mit Sturz Schambeinast-Fx links. Pneumopathie. Anämie (hyperchrom makrozyt.) Vit. D Mangel. Makuladeg. bds. Medik. ASS, β-Blocker, Nitro, Liquemin. Torem, Laxoberon. Atrovent, Ventolin. Temesta, Trittico, … Pantozol, Motilium. Morphin, Paracet.,")
4
Hyponatriämie: Relevant?
rel. hohe Prävalenz bei älteren Leuten: ca. 6%, aber bis 30% in Pflegeheimen (Schrier RW, 2010) 60x ↑ in Morbidität und Mortalität (Reddy & Morandian, 2009) schlechter prognostischer Faktor (CHD, liver cirrhosis, …)
 60x ↑ in Morbidität und Mortalität (Reddy & Morandian, 2009) schlechter prognostischer Faktor (CHD, liver cirrhosis, …)")
5
Physiologie 1: Kompartmente
♀: 50% KG ♂: 60% KG Alter: Fett ↑, H2O ↓ %- H2O : ↓ Intrazell. Extrazell. 2/3 1/3

6
Physiologie 1: Kompartmente
♀: 50% KG ♂: 60% KG Alter: Fett ↑, H2O ↓ %- H2O : ↓ Intrazell. Extrazell. 2/3 1/3 v.a. K+ v.a. Na+

7
Physiologie 1: Kompartmente
♀: 50% KG ♂: 60% KG Alter: Fett ↑, H2O ↓ %- H2O : ↓ 2/3 1/3 Intrazell. interstit. intravasc. 1/3 v.a. K+ v.a. Na+

8
Physiologie 2: Regulation
Volumenregulation > Osmoregulation Volumen: Na+ RAAS Natriuretic Peptides (ANP, BNP, …) … Osmolalität: H2O ADH Durst
 … Osmolalität: H2O. ADH. Durst.")
9
Physiologie 3: Na+-Resorbption
ENAC 5 - 1 0% Na Cl (TSC) Selective Sodium Channel Aldost. Na+/… -CoTransp. Na+/H+-Exchanger 60-70% Aldost. 20-30% Na+ K+ Cl-
 Selective Sodium Channel. Aldost. Na+/… -CoTransp. Na+/H+-Exchanger % Aldost % Na+ K+ Cl-")
10
Hyponatriämie 1: Symptome
Faktoren [Na+], Zeit! “asymptomatisch”? Elderly: falls, attention and neuropsyc. tests, … Progn. Faktor! Hypoosmolalität (…) Hyponatremic encephalopathy Cerebral edema Neur.: < mmol/L und akut (:= < 48h) <125mmol/L Reizbarkeit, Nausea, Erbrechen Verwirrtheit <120mmol/L Kopf-Sz Somnolenz <115mmol/L ↑ Reflexe Epilepsie Koma Tod aus Surf Med
 Hyponatremic encephalopathy. Cerebral edema. Neur.: < mmol/L. und akut (:= < 48h) <125mmol/L. Reizbarkeit, Nausea, Erbrechen. Verwirrtheit. <120mmol/L. Kopf-Sz. Somnolenz. <115mmol/L. ↑ Reflexe. Epilepsie. Koma. Tod. aus Surf Med.")
11
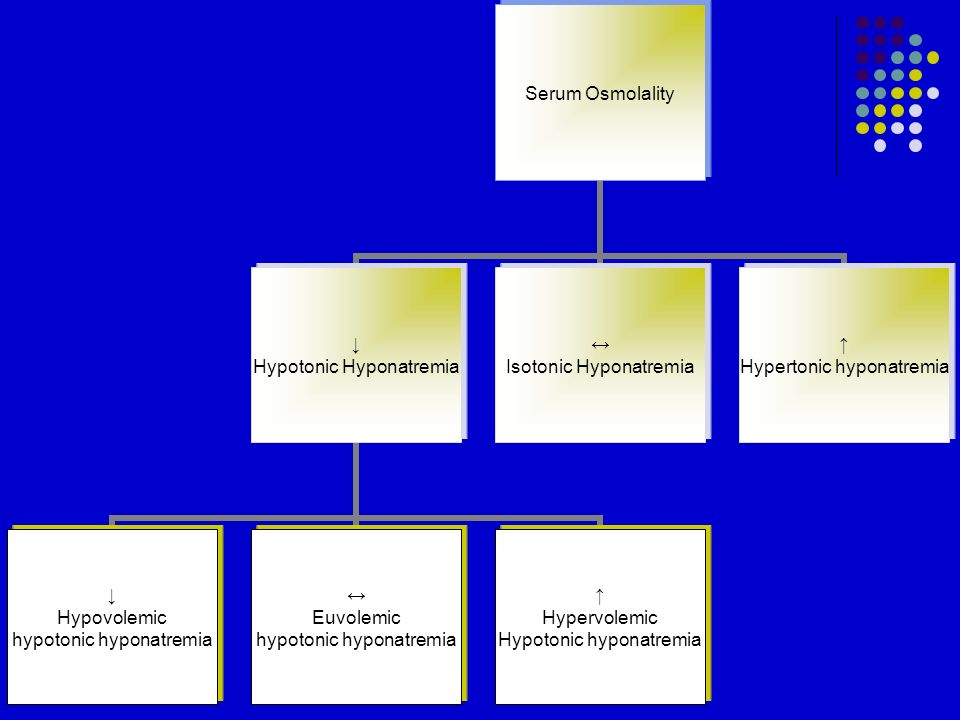
Hyponaträmie 2: Einteilung
Harrison’s, 17th ed.

15
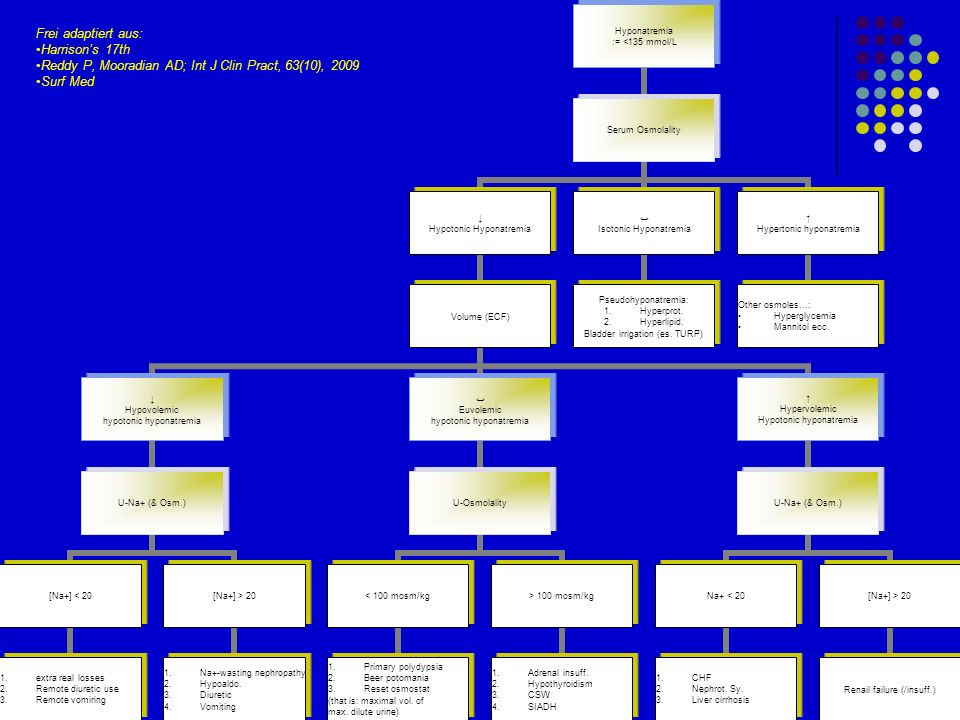
Frei adaptiert und vereinfacht aus:
Harrison’s 17th Reddy P, Mooradian AD; Int J Clin Pract, 63(10), 2009 Surf Med
, Surf Med.")
16
Frau E.: Labor Na+: 124 mmol/L ↓ Plasma-Osm.: 276 mosm/kg ↓
Volumen: zuerst trocken/normal dann ↑ 2,8kg in 4 Tage > Aber: /!\: unter Diuretika-Th (loop-d. + Aldact.) Urin-Na+: 42 mmol/L ↑ Urin-Osm.: 445 mosm/kg mosm/kg (♂493±184mosm/kg, ♀ 657±127mosm/kg) (Parlindungan S, Setiati S; Urine Osmolality in the Elderly; Indones J Intern Med, 42 (1), January 2010) trocken/normal ↑ ↓ / ↔ / ↑
 Urin-Na+: 42 mmol/L ↑ Urin-Osm.: 445 mosm/kg mosm/kg. (♂493±184mosm/kg, ♀ 657±127mosm/kg) (Parlindungan S, Setiati S; Urine Osmolality in the Elderly; Indones J Intern Med, 42 (1), January 2010) trocken/normal. ↑ ↓ / ↔ / ↑")
17
Frei adaptiert und vereinfacht aus:
Harrison’s 17th Reddy P, Mooradian AD; Int J Clin Pract, 63(10), 2009 Surf Med
, Surf Med.")
18
Behandlung (Prinzipien)
Ödemat. Pat., CHF, hepat. Zirrhose, NI Volumenverlust unkontr. DM SIADH Reset osmostat Primary polydypsia Adrenalinsuff., Hypothyroidismus Hypervolemic, hypotonic Hypovolemic, hypotonic Hypertonic Euvolemic, hypotonic

19
Behandlung (Prinzipien)
Hypotonisch, hypervoläm Hypotonisch, hypovoläm Euvoläm Endokrin H2O Restriktion Isotone NaCl –L. (± hypert.) Kompliziert, differenziert SIADH: V2-Rez. Antag. + kausal Faustregel: H2O-Restr., (± isot.) ± hypert. ± Schleifendiuretika (Surf Med, Reddy 2009) kausal /!\: hypertone NaCl-L. nur bei schweren u./o. symptomatische Hyponatriämie!
 Kompliziert, differenziert. SIADH: V2-Rez. Antag. + kausal Faustregel: H2O-Restr., (± isot.) ± hypert. ± Schleifendiuretika (Surf Med, Reddy 2009) kausal. /!\: hypertone NaCl-L. nur bei schweren u./o. symptomatische Hyponatriämie!")
20
SIADH mit isotonic saline?
+ 547 Hypertonic -500 Hypertonic + loop diuretic - 1280

21
SIADH - Behandlung Ursächlich H2O-Restr. Hypert. NaCl
Aber /!\: Pneumonie, Meningitis, … H2O geben! Hypert. NaCl ± Schleifendiuretika (Furosemid, Torasemid, …) (Colombo SM et al., Akute Meningitis mit Hyponatriämie = SIADH = Syndrom des inappropriaten ärztlichen diagnostischen Hirnreflexes?; Poster, SGP-SSP 2002 von Vigier RO, Colombo SM, Stoffel PB, Meregalli P, Truttmann AC, Bianchetti MG: Circulating sodium in acute meningitis. Am J Nephrol 21: 87-90)
 (Colombo SM et al., Akute Meningitis mit Hyponatriämie = SIADH = Syndrom des inappropriaten ärztlichen diagnostischen Hirnreflexes ; Poster, SGP-SSP von Vigier RO, Colombo SM, Stoffel PB, Meregalli P, Truttmann AC, Bianchetti MG: Circulating sodium in acute meningitis. Am J Nephrol 21: 87-90)")
22
SIADH: Ursachen Onko.: v.a. SMLC
Oropharynx, GIT, genitourinary tract, Lymphomen, Ewing sarcomas, … Lungen: (Pneumonie), CF, St. asthmaticus ZNS: Infektionen, CVI, … Medik.: Diuretika (v.a. Thiazide), Antidepressiva (v.a. SSRI), Antiepileptika, Antipsichotika, Anästhetica, … Nausea, Sz., Stress Exercice associated (aber…) Idiopatisch
, CF, St. asthmaticus. ZNS: Infektionen, CVI, … Medik.: Diuretika (v.a. Thiazide), Antidepressiva (v.a. SSRI), Antiepileptika, Antipsichotika, Anästhetica, … Nausea, Sz., Stress. Exercice associated (aber…) Idiopatisch.")
23
Teaching points Hyponatriämie Alter(n): anfällig(er) werden?
differenziertes Handeln zuerst denken, dann agieren (Physiol., PPH, PHA) Pat. behandeln, nicht Labor (riskant!) “asymptomatische” Hyponatriämie ???? Alter(n): anfällig(er) werden? Sturz: Morbidität und Mortalität Ende des Lebens
 Pat. behandeln, nicht Labor (riskant!) asymptomatische Hyponatriämie Alter(n): anfällig(er) werden Sturz: Morbidität und Mortalität. Ende des Lebens.")
24
Literatur: 2 wichtige Angaben
Reddy P, Mooradian P; Diagnosis and management of hyponatremia in hospitalised patients; Int J Clin Pract, October 2009, 63(10): Schrier RW, Does ‘asymptomatic hyponatremia’ exist?, Nature Reviews Nephrology, Vol. 6, April 2010: 185 Zur Vertiefung: Goh PK, Management of Hyponatremia, Am Fam Physician, 69 (10), May 2004 Hoorn EJ et al., SIADH and hyponatremia: why does it matter?; NDT Plus, 2009, 2 [Suppl 3]: iii5-iii11 Parlindungan S, Setiati S; Urine Osmolality in the Elderly; Indones J Intern Med, 42 (1), January 2010
: Schrier RW, Does ‘asymptomatic hyponatremia’ exist , Nature Reviews Nephrology, Vol. 6, April 2010: 185. Zur Vertiefung: Goh PK, Management of Hyponatremia, Am Fam Physician, 69 (10), May Hoorn EJ et al., SIADH and hyponatremia: why does it matter ; NDT Plus, 2009, 2 [Suppl 3]: iii5-iii11. Parlindungan S, Setiati S; Urine Osmolality in the Elderly; Indones J Intern Med, 42 (1), January")
25
Vielen Dank für Ihre Aufmerksamkeit!
Sebastiano A.G. Lava

Ähnliche Präsentationen