Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
GLP-1 Mimetika: eine Alternative vor der Insulintherapie?
Bruno Müller Endokrinologie und Diabetologie FMH Bern

2
Antwort Yes Oder moderner….

3
Lernziele Yes you can Knacken the Bankgeheheimis

4
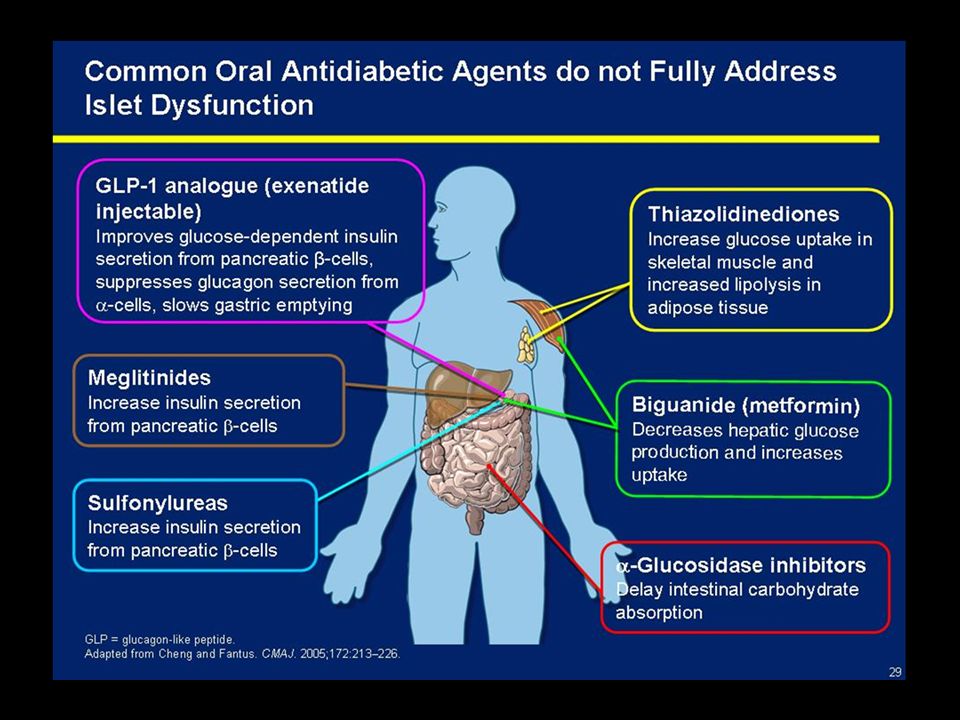
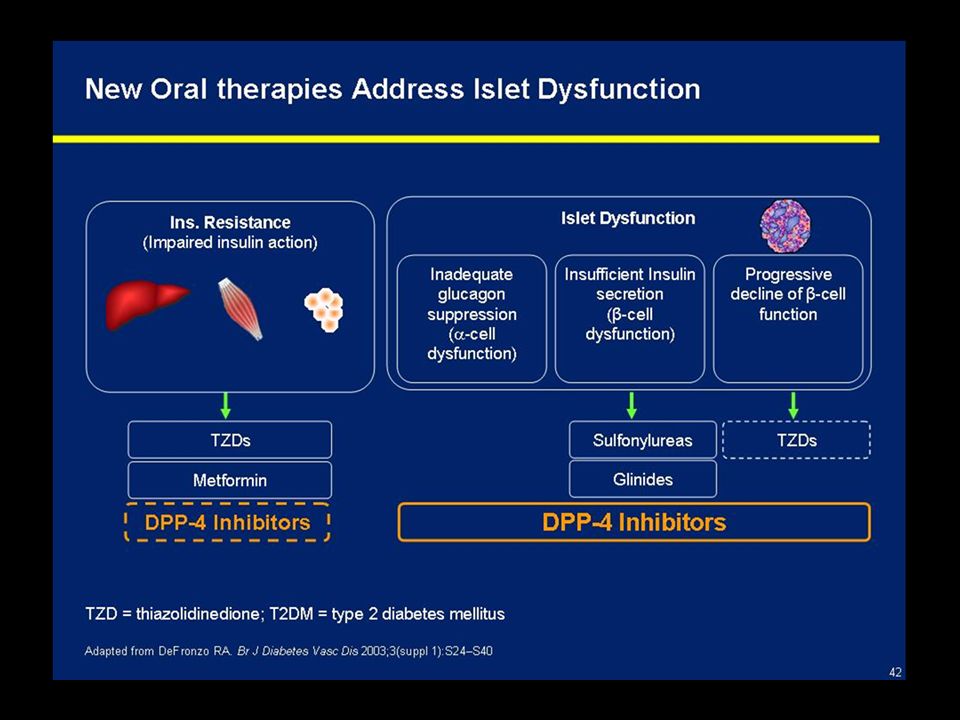
Lernziele Zuhörer kennt die wichtigsten Vor- und Nachteile sowie die wichtigsten pharmakologischen Wirkstoffgruppen der OAD Kennt die wichtigsten Eigenschaften und Indikationen der neuen Antidiabetika Vortrag Praxisnah

5
Faust

6
„Nun sag, welches ist die beste Medizin?“
Die berühmte Gretchenfrage!

9
Wie hat sich Hans Meister ca. 1930 bewegt / ernährt

10
Inhalte – key points Stufe 2 der Diabetestherapie Fallbeispiel
Praktische Tipps Change

13
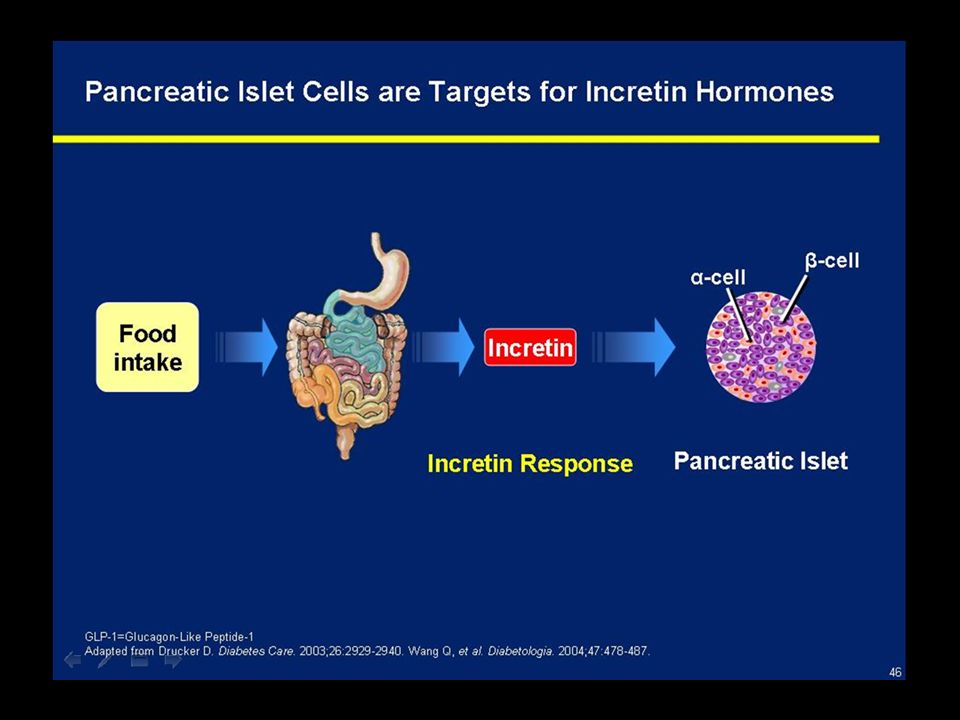
GLP-1 Effects in Humans: Understanding the Glucoregulatory Role of Incretins
Promotes satiety and reduces appetite Alpha cells: ↓ Postprandial glucagon secretion DISCUSSION By decreasing β-cell workload and improving β-cell response, the incretin glucagon-like peptide 1 (GLP-1) is an important regulator of glucose homeostasis A thorough understanding of the five GLP-1 glucoregulatory effects is important to assess the value of GLP-1 in controlling glucose levels, particularly during the postprandial period Upon ingestion of food, GLP-1 is secreted in into the bloodstream and enhances glucose dependent insulin secretion from β-cells GLP-1 suppresses inappropriately elevated glucagon secretion from alpha cells Lower levels of glucagon lead to a reduction of glucose output from the liver and indirectly reduce the β-cell workload By slowing the gastric emptying rate, GLP-1 slows the release of nutrients into the gut allowing more time to control the postprandial increase in glucose levels GLP-1 promotes satiety, potentially through centrally mediated mechanisms BACKGROUND GLP-1 is secreted from L cells of the small intestine GLP-1 decreases β-cell workload, hence the demand for insulin secretion, by: Regulating the rate of gastric emptying such that meal nutrients are delivered to the small intestine and, in turn, absorbed into the circulation more smoothly, reducing peak nutrient absorption and insulin demand (β-cell workload) Decreasing postprandial glucagon secretion from pancreatic alpha cells, which helps to maintain the counterregulatory balance between insulin and glucagon Reducing postprandial glucagon secretion, GLP-1 has an indirect benefit on β-cell workload, since decreased glucagon secretion will produce decreased postprandial hepatic glucose output Having effects on the central nervous system, resulting in increased satiety (sensation of satisfaction with food intake) and a reduction of food intake Effect on Beta cell: Drucker DJ. Diabetes. 1998;47: Effect on Alpha cell: Larsson H, et al. Acta Physiol Scand. 1997;160: Effects on Liver: Larsson H, et al. Acta Physiol Scand. 1997;160: Effects on Stomach: Nauck MA, et al. Diabetologia. 1996;39: Effects on CNS: Flint A, et al. J Clin Invest. 1998;101: Liver: ↓ Glucagon reduces hepatic glucose output Beta cells: Enhances glucose-dependent insulin secretion Stomach: Helps regulate gastric emptying Adapted from Flint A, et al. J Clin Invest. 1998;101: ; Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160: ; Adapted from Nauck MA, et al. Diabetologia. 1996;39: ; Adapted from Drucker DJ. Diabetes. 1998;47:
 is an important regulator of glucose homeostasis. A thorough understanding of the five GLP-1 glucoregulatory effects is important to assess the value of GLP-1 in controlling glucose levels, particularly during the postprandial period. Upon ingestion of food, GLP-1 is secreted in into the bloodstream and enhances glucose dependent insulin secretion from β-cells. GLP-1 suppresses inappropriately elevated glucagon secretion from alpha cells. Lower levels of glucagon lead to a reduction of glucose output from the liver and indirectly reduce the β-cell workload. By slowing the gastric emptying rate, GLP-1 slows the release of nutrients into the gut allowing more time to control the postprandial increase in glucose levels. GLP-1 promotes satiety, potentially through centrally mediated mechanisms. BACKGROUND. GLP-1 is secreted from L cells of the small intestine. GLP-1 decreases β-cell workload, hence the demand for insulin secretion, by: Regulating the rate of gastric emptying such that meal nutrients are delivered to the small intestine and, in turn, absorbed into the circulation more smoothly, reducing peak nutrient absorption and insulin demand (β-cell workload) Decreasing postprandial glucagon secretion from pancreatic alpha cells, which helps to maintain the counterregulatory balance between insulin and glucagon. Reducing postprandial glucagon secretion, GLP-1 has an indirect benefit on β-cell workload, since decreased glucagon secretion will produce decreased postprandial hepatic glucose output. Having effects on the central nervous system, resulting in increased satiety (sensation of satisfaction with food intake) and a reduction of food intake. Effect on Beta cell: Drucker DJ. Diabetes. 1998;47: Effect on Alpha cell: Larsson H, et al. Acta Physiol Scand. 1997;160: Effects on Liver: Larsson H, et al. Acta Physiol Scand. 1997;160: Effects on Stomach: Nauck MA, et al. Diabetologia. 1996;39: Effects on CNS: Flint A, et al. J Clin Invest. 1998;101: Liver: ↓ Glucagon reduces hepatic glucose output. Beta cells: Enhances glucose-dependent insulin secretion. Stomach: Helps regulate gastric emptying. Adapted from Flint A, et al. J Clin Invest. 1998;101: ; Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160: ; Adapted from Nauck MA, et al. Diabetologia. 1996;39: ; Adapted from Drucker DJ. Diabetes. 1998;47:")
14
Nur BYETTA hat fünf wichtige Wirkungen
Organe Die fünf Vorteile von BYETTA1 Klinische Hauptergebnisse zu BYETTA 1 Fördert die Glukose-abhängige Insulinsekretion Nachhaltige A1C-Kontrolle Geringes Hypoglykämie- Risiko† Gewichtsabnahme Stellt die First-Phase-Insulin- Response wieder her Supprimiert Glukagon; senkt Glukoseproduktion Verlangsamt beschleunigte Magenentleerung Senkt die Nahrungsaufnahme* DISCUSSION POINTS BYETTA, like a pharmacologic dose of continuously infused GLP-12-6 CLICK #1: Enhances glucose-dependent insulin production CLICK #2: Restores first-phase insulin response CLICK #3: Decreases postprandial glucagon production, thus decreasing hepatic glucose output CLICK #4: Regulates gastric emptying, decreasing the rate of peak nutrient absorption from meals CLICK #5: Decreases food intake BUT, one important difference – BYETTA is resistant to enzymatic degradation by DPP-4, thus extending the presence of BYETTA in plasma following a subcutaneous (SC) injection (measurable for up to 10 hours) SLIDE BACKGROUND Following the SC administration of BYETTA to patients with type 2 diabetes, BYETTA reaches median peak plasma concentrations in 2.1 hours The mean terminal half-life of BYETTA is 2.4 hours Pharmacokinetic characteristics of BYETTA are independent of the dose; in most individuals, BYETTA concentrations are measurable for approximately 10 hours post dose See accompanying Arzneimittel-Kompendium der Schweiz and safety information included in this presentation References: 1. Aronoff SL, et al. Diabetes Spectrum. 2004;17: 2. Nielsen LL, et al. Regul Pept. 2004;117:77-88. 3. Fehse F, et al. J Clin Endocrinol Metab. 2005;90: 4. Kolterman OG, et al. J Clin Endocrinol Metab. 2003;88: 5. Maekawa F, et al. J Neuroendocrinol. 2006;18: 6. Rachman J, et al. Diabetes. 1996;45: *Dieser Effekt wird vermutlich durch das Zentralnervensystem vermittelt. †Wird BYETTA mit einem SFU benutzt, besteht ein erhöhtes Risiko von Hypoglykämie. Literatur: 1 Arzneimittel-Kompendium der Schweiz 34 F ©2007 AMYLIN PHARMACEUTICALS, INC. AND ELI LILLY AND COMPANY. 14
 injection (measurable for up to 10 hours) SLIDE BACKGROUND. Following the SC administration of BYETTA to patients with type 2 diabetes, BYETTA reaches median peak plasma concentrations in 2.1 hours. The mean terminal half-life of BYETTA is 2.4 hours. Pharmacokinetic characteristics of BYETTA are independent of the dose; in most individuals, BYETTA concentrations are measurable for approximately 10 hours post dose. See accompanying Arzneimittel-Kompendium der Schweiz and safety information included in this presentation. References: 1. Aronoff SL, et al. Diabetes Spectrum. 2004;17: Nielsen LL, et al. Regul Pept. 2004;117: Fehse F, et al. J Clin Endocrinol Metab. 2005;90: Kolterman OG, et al. J Clin Endocrinol Metab. 2003;88: Maekawa F, et al. J Neuroendocrinol. 2006;18: Rachman J, et al. Diabetes. 1996;45: *Dieser Effekt wird vermutlich durch das Zentralnervensystem vermittelt. †Wird BYETTA mit einem SFU benutzt, besteht ein erhöhtes Risiko von Hypoglykämie. Literatur: 1 Arzneimittel-Kompendium der Schweiz F. ©2007 AMYLIN PHARMACEUTICALS, INC. AND ELI LILLY AND COMPANY. 14.")
16
Blutzuckerkontrolle und Gewichtsmanagement: Welche Wahlmöglichkeiten haben wir?
Was tun, wenn sich A1C durch Änderungen des Lebensstils und Metformin-Gabe nicht unter Kontrolle bringen oder unter Kontrolle halten lässt? Therapieoptionen A1C Körpergewicht Sulfonylharnstoff1 TZD2,3 DPP-4-Hemmer4 DISCUSSION POINTS The patient is on the foundation of medical nutritional therapy and metformin, but needs an additional agent to reach A1C goal We have multiple choices for therapy, from oral meds to injectable meds, all of which have been shown to lower A1C Remembering that 85% of patients with T2DM are overweight or obese5, and the well-established benefits of weight maintenance, which agent would be the ideal next addition to meet those ADA goals? SLIDE BACKGROUND References: Malone M. Ann Pharmacother. 2005;39: Pfizer. Glucotrol XL® Full Arzneimittel-Kompendium der Schweiz.2006. Takeda. Actos® Full Arzneimittel-Kompendium der Schweiz GlaxoSmithKline. Avandia® Full Arzneimittel-Kompendium der Schweiz.2007. Merck Januvia® Full Arzneimittel-Kompendium der Schweiz Literatur: 1. W.S. Leslie et al. Weight gain as an adverse effect of some commonly prescribed drugs: a systematic review. Q J Med 2007; 100:395–404. ; 2. Takeda. Actos® Arzneimittel-Kompendium der Schweiz. 2008; 3. GlaxoSmithKline. Avandia® Arzneimittel-Kompendium der Schweiz ; 4. Merck Januvia® Arzneimittel-Kompendium der Schweiz. 2008 F ©2007 AMYLIN PHARMACEUTICALS, INC. AND ELI LILLY AND COMPANY. 16

17
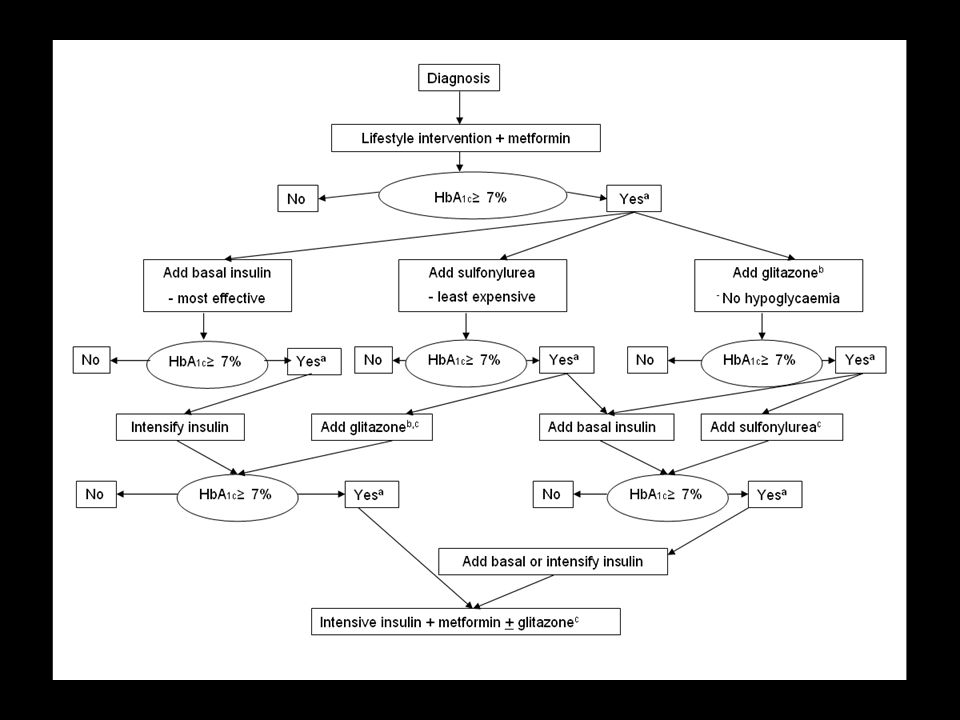
Lifestyle intervention + metformin
Diagnosis Lifestyle intervention + metformin HbA1c≥ 7% No Yesª Add basal insulin - most effective Add sulfonylurea - least expensive Add glitazoneb - No hypoglycaemia HbA1c≥ 7% HbA1c≥ 7% HbA1c≥ 7% No Yesª No Yesª No Yesª Intensify insulin Add glitazoneb,c Add basal insulin Add sulfonylureac HbA1c≥ 7% HbA1c≥ 7% No Yesª No Yesª Add basal or intensify insulin Intensive insulin + metformin + glitazonec

18
Diabetes mellitus – Update 2009
ADA-EASD Diabetes Care, Dezember 2008 Diabetes mellitus – Update 2009

19
Inhalte – key points Stufe 2 der Diabetestherapie Fallbeispiel
Praktische Tipps Change

20
Fallbeispiel Konsultation 2003
30j 40j 50j 60j 70j Konsultation 2003 K.B., Metzger, körperl. nicht mehr sehr aktiv, kinderlos, verheiratet Pos. FA für Diabetes mellitus Typ 2 (Mutter, mit Beinamputationen) Weitere Diagnosen: Hypertonie, hypertensive (und eventuell koronare) Kardiopathie (formal St. nach inferiorem MI möglich), Hyopogonadismus Diskussion Diabetes Prävention
 Weitere Diagnosen: Hypertonie, hypertensive (und eventuell koronare) Kardiopathie (formal St. nach inferiorem MI möglich), Hyopogonadismus. Diskussion Diabetes Prävention.")
21
Fallbeispiel Konsultation 2003
30j 40j 50j 60j 70j Konsultation 2003 Medikamente: Andriol, 2-1-2, Coversum Combi, Glucophage 2mal 850mg Grösse 190 cm, G 129 kg, BMI 36 kg/m2 BD 145/90 Diskussion Diabetes Prävention

22
Fallbeispiel Konsultation 2003 Nüchtern-Glucose (Plasma) 7.5 mmol/l
30j 40j 50j 60j 70j Konsultation 2003 Nüchtern-Glucose (Plasma) 7.5 mmol/l Cholesterin Gesamt mmol/l HDL Cholesterin mmol/l Nü-Triglyzeride < 0.8 mmol/l Kreatinin umol/l HbA1c % Diskussion Diabetes Prävention
 7.5 mmol/l. Cholesterin Gesamt 3.19 mmol/l. HDL Cholesterin 1.25 mmol/l. Nü-Triglyzeride < 0.8 mmol/l. Kreatinin 74 umol/l. HbA1c 8.2 % Diskussion Diabetes Prävention.")
23
Verlaufskontrolle 4 Jahre später
30j 40j 50j 60j 70j Verlaufskontrolle 4 Jahre später Nun unter Sulfonylharnstoff (Diamicron MR 30mg 2-0-1) und Metformin (3mal 850) BMI 38 kg/m2 (190 cm, 137 kg) Blutdruck 145/90 mmHg, normokard HbA1c 6.7% BZ-Profil im Durchschnitt (kapillär): Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin) Morgen Mittag Abend Vor Bettruhe 7-8 mmol/l 6-9 mmol/l 6-8 mmol/l Nicht gemessen
 und Metformin (3mal 850) BMI 38 kg/m2 (190 cm, 137 kg) Blutdruck 145/90 mmHg, normokard. HbA1c 6.7% BZ-Profil im Durchschnitt (kapillär): Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin) Morgen. Mittag. Abend. Vor Bettruhe. 7-8 mmol/l. 6-9 mmol/l. 6-8 mmol/l. Nicht gemessen.")
24
Neu Schlaf-Apnoe-Syndrom
30j 40j 50j 60j 70j ... Zufrieden? Probleme? Gewichtszunahme von 129 kg, BMI 36 kg/m2 auf aktuelle 137 kg, BMI neu 38 Lipide gut !! Hat Aspirin Neu Schlaf-Apnoe-Syndrom Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin)
")
25
SH kontraindiziert (Gewichtszunahme)
30j 40j 50j 60j 70j Probleme SH kontraindiziert (Gewichtszunahme) Was ist wichtiger: HbA1c-Verbesserung (von 8.2 auf 6.7) oder aber ungünstiger Gewichtsverlauf? Güterabwägung…. Wie Gewicht reduzieren? SAS gerichtet angehen? Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin)
 Was ist wichtiger: HbA1c-Verbesserung (von 8.2 auf 6.7) oder aber ungünstiger Gewichtsverlauf Güterabwägung…. Wie Gewicht reduzieren SAS gerichtet angehen Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin)")
26
... Gewicht reduzieren, aber wie?
30j 40j 50j 60j 70j ... Gewicht reduzieren, aber wie? Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin)
")
27
... Gewicht reduzieren, aber wie?
30j 40j 50j 60j 70j ... Gewicht reduzieren, aber wie? Beginn mit Byetta Oktober 2007, Gewicht 137 kg HbA1c 6.6% Stand 09/08: Byetta 10 ug morgens/abends, Diamicron gestoppt, Glucophage unverändert Gewicht 111.9, Reduktion von 25kg innerhalb von rund 10 Monaten Kein Schlaf-Apnoe-Syndrom Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin)
")
28
Vorschlag fürs Procedere?
30j 40j 50j 60j 70j Vorschlag fürs Procedere? Erhöhter Nü-BZ -> Diskussion Monotherapie first line (Metformin)
")
29
Inhalte – key points Stufe 2 der Diabetestherapie Fallbeispiel
Praktische Tipps Change

30
BYETTA: einfacher Therapiebeginn
Nach dem ersten Gebrauch kann BYETTA bei Raumtemperatur (<25 °C) aufbewahrt werden. BYETTA wird innerhalb einer Stunde vor einer Mahlzeit angewendet. Keine Dosisanpassungen wegen Umfang der Mahlzeit oder Sport Keine zusätzliche Blutzuckerüberwachung erforderlich Einfache Verabreichung mit vorbefülltem Injektionspen 2x tgl. 5 µg kann auf 2x tgl. 10 µg gesteigert werden Woche ab der 5. Woche* **Die subkutane Injektion kann jederzeit innerhalb von 60 Minuten vor dem Frühstück oder der Abendmahlzeit erfolgen.1 DISCUSSION POINT BYETTA can be easily added to a patient’s current therapy Initiate the patient with 5 µg BID; then, based on glycemic response and tolerability, increase to 10 µg BID after 1 month No dose adjustments are necessary based on meal size or exercise No additional glucose monitoring required BYETTA is available in easy-to-use prefilled pens Before first use, BYETTA must be stored refrigerated at 36ºF to 46ºF (2ºC to 8ºC) After first use, BYETTA can be kept at a room temperature not to exceed 77ºF (25ºC) Do not freeze the BYETTA pen SLIDE BACKGROUND See accompanying Arzneimittel-Kompendium der Schweiz and safety information included in this presentation Siehe beiliegenden Text aus dem Arzneimittel-Kompendium der Schweiz und die Sicherheitsdaten in dieser Präsentation. F ©2007 AMYLIN PHARMACEUTICALS, INC. AND ELI LILLY AND COMPANY. 30
 aufbewahrt werden. BYETTA wird innerhalb einer Stunde vor einer Mahlzeit angewendet. Keine Dosisanpassungen wegen Umfang der Mahlzeit oder Sport. Keine zusätzliche Blutzuckerüberwachung erforderlich. Einfache Verabreichung mit vorbefülltem Injektionspen. 2x tgl. 5 µg kann auf 2x tgl. 10 µg gesteigert werden. Woche 1-4 ab der 5. Woche* **Die subkutane Injektion kann jederzeit innerhalb von 60 Minuten vor dem Frühstück oder der Abendmahlzeit erfolgen.1. DISCUSSION POINT. BYETTA can be easily added to a patient’s current therapy. Initiate the patient with 5 µg BID; then, based on glycemic response and tolerability, increase to 10 µg BID after 1 month. No dose adjustments are necessary based on meal size or exercise. No additional glucose monitoring required. BYETTA is available in easy-to-use prefilled pens. Before first use, BYETTA must be stored refrigerated at 36ºF to 46ºF (2ºC to 8ºC) After first use, BYETTA can be kept at a room temperature not to exceed 77ºF (25ºC) Do not freeze the BYETTA pen. SLIDE BACKGROUND. See accompanying Arzneimittel-Kompendium der Schweiz and safety information included in this presentation. Siehe beiliegenden Text aus dem Arzneimittel-Kompendium der Schweiz und die Sicherheitsdaten in dieser Präsentation F. ©2007 AMYLIN PHARMACEUTICALS, INC. AND ELI LILLY AND COMPANY. 30.")
31
Die häufigsten Nebenwirkungen Grosse klinische Studien der Phase III
Kombinierte Ergebnisse der 30-wöchigen Phase-III-Studien zu Exenatide Placebo (N = 483) 5 µg Exenatide (N = 480) 10 µg Exenatide (N = 483) 48% 39% 18% Übelkeit 25% 15% 8% Hypoglykämie 15% 11% 6% Diarrhö 13% 4% Erbrechen 7% 10% 6% Kopfschmerzen 10% 9% 4% Nervosität ITT-Population; Mittelwert (Standardfehler); MET (N=336), SFU (N=377), MET + SFU (N=733); *p<0,05 vs. Placebo; **p<0,001 vs. Placebo. Mittl. Baseline-Gewicht in allen Studienarmen zwischen 95 und 101 kg. Adaptiert aus: DeFronzo RA, et al. Diabetes Care. 2005;28: ; Buse JB, et al. Diabetes Care. 2004;27: ; Kendall DM, et al. Diabetes Care. 2005;28: Nachdruck mit Genehmigung der American Diabetes Association.
 5 µg Exenatide (N = 480) 10 µg Exenatide (N = 483) 48% 39% 18% Übelkeit. 25% 15% 8% Hypoglykämie. 15% 11% 6% Diarrhö. 13% 4% Erbrechen. 7% 10% 6% Kopfschmerzen. 10% 9% 4% Nervosität. ITT-Population; Mittelwert (Standardfehler); MET (N=336), SFU (N=377), MET + SFU (N=733); *p<0,05 vs. Placebo; **p<0,001 vs. Placebo. Mittl. Baseline-Gewicht in allen Studienarmen zwischen 95 und 101 kg. Adaptiert aus: DeFronzo RA, et al. Diabetes Care. 2005;28: ; Buse JB, et al. Diabetes Care. 2004;27: ; Kendall DM, et al. Diabetes Care. 2005;28: Nachdruck mit Genehmigung der American Diabetes Association.")
32
Change

34
Diabetes mellitus – Update 2009
ADA-EASD Diabetes Care, Dezember 2008 Diabetes mellitus – Update 2009

35
When asked why he changed his position on an issue, John Maynard Keynes said: “When the facts change, I change my mind. What do you do, sir?”

36
Schlussfolgerung Griffige Lifestyle- und Therapeimassnahmen zielen darauf ab, bei übergewichtigen Diabetikern das Gewicht zu reduzieren … und die Sarkopenie zu verhindern Dies geschieht durch geeignete Ernährungsmassnahmen und Bewegung (Hypertrophie-Training!!)
")
37
Schlussfolgerung Medikamentöse Hilfen? Acomplia, Reductil, Xenical, SRI wie Fluctine, Efexor…, Topamax.. oder aber gewichtsreduzierende gr Antidiabetika Unter den gr ‚Antidiabetika‘ ist Byetta ein effizientes Tool, um Gewicht und Blutzucker zu reduzieren

38
„Nun sag, welches ist die beste Medizin?“
… auf Stufe 2 Die berühmte Gretchenfrage!

Ähnliche Präsentationen