Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
(Unübliches zur) Menopause
Bruno Müller Bern

2
Absturz / Pause oder Abflug?
Machen Sie sich selber ein Bild …

4
positiver Feedback (Hohlwegeffekt)
Der Temperaturanstieg um ca. 0,6 °C ist ein Gestageneffekt Karyopyknose-Index = kernlose, pyknotische kernhaltige Zellen Ausschüttung von LH positiver Feedback (Hohlwegeffekt) Östradiolanstieg Östrogene: Proliferation, Zervikalsekret spinn- bar, hoher Karyopyknose-Index Gestagene: sekretorische Umwandlung, Vorbereitung Nidation/Eitransport Zervikalsekret zähflüssig, niedriger Karyopyknose-Index Proliferative / Sekretorische Phase
 Östradiolanstieg. Östrogene: Proliferation, Zervikalsekret spinn- bar, hoher Karyopyknose-Index. Gestagene: sekretorische Umwandlung, Vorbereitung Nidation/Eitransport Zervikalsekret zähflüssig, niedriger Karyopyknose-Index. Proliferative / Sekretorische Phase.")
7
Pause / Abbruch oder Abflug?
Endokrinologisch gesehen ist die Frau überaus komplex gesteuert …. Leider sind Störfälle Oder gar definitive Funktionsausfälle vorprogrammiert Absturz

8
Inhalte – key points Menopause allgemein: - Altern - Epidemiologie
- Reparaturmechanismen

9
Alle versuchen, die Zeit totzuschlagen, und keiner will sterben
Franz. Sprichwort

11
Altern wir, weil die Menge wichtiger Hormone abnimmt?
Oder: nimmt die Hormonkonzentration ab, weil wir altern?

12
„Nun sag, wie hast du’s mit der Religion?“
Die berühmte Gretchenfrage!

13
Altern, am Bsp. der Oocyten
5th SS-Monat — 7 million Geburt — 1-2 Millionen Pubertät — 400,000 Rascher Oocytenverlust

14
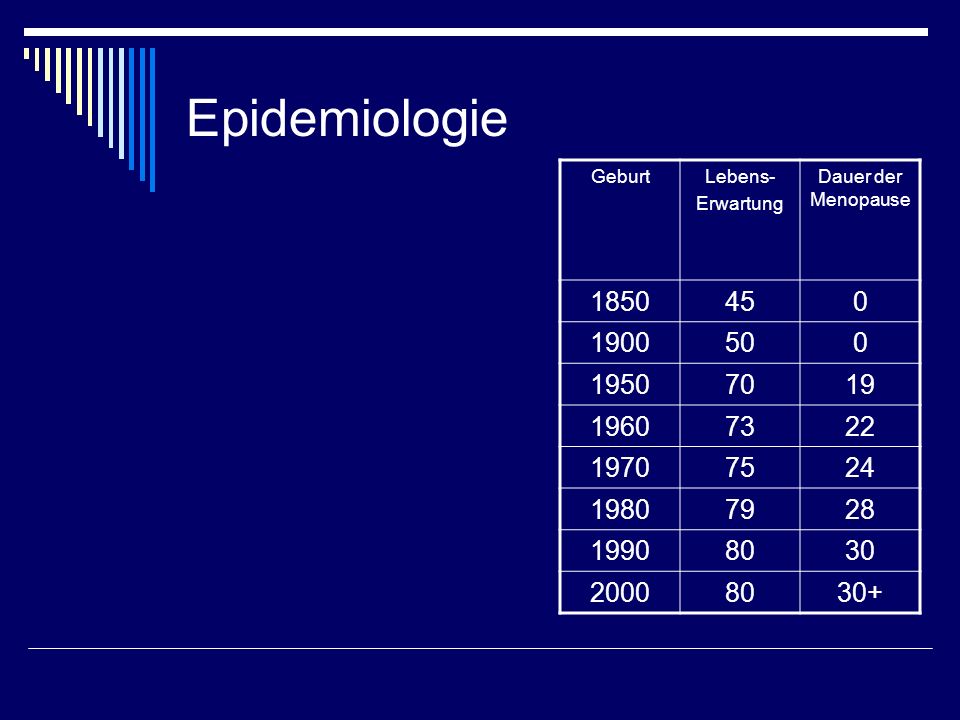
Epidemiologie Geburt Lebens- Erwartung Dauer der Menopause 1850 45 1900 50 1950 70 19 1960 73 22 1970 75 24 1980 79 28 1990 80 30 2000 30+
15
Demografische Angaben
Quelle: Statistisches Bundesamt, Statistisches Jahrbuch 2007

16
Theories of Aging Genetic Wear and Tear
Aging is “programmed” into the genes Certain genes are “timekeepers” for the aging process Wear and Tear Cumulative damage to cells from Metabolic processes Environmental factors Mechanisms to resist and repair damage are critical

17
Mechanisms to resist and repair damage
Zelluläre Endokrinologische Lifestyle, Therapeutische (Hormonersatz, HRT, Alternatives)
")
18
N oxygen glucose Energy SOD N
Cellular Damage and Defense Antioxidants (GSH, tocopherols, etc.) Energy (ATP) O2 radicals O• DNA damage Protein damage Lipid damage SOD Catalase GPX H2O2 H2O + O2 Defense Enzymes OH- Mitochondria Nucleus (DNA) Cell Membrane Cytoplasm -proteins Repair Processes N
 Energy. (ATP) O2 radicals. O• DNA damage. Protein damage. Lipid damage. SOD. Catalase. GPX. H2O2. H2O + O2. Defense. Enzymes. OH- Mitochondria. Nucleus (DNA) Cell Membrane. Cytoplasm -proteins. Repair. Processes. N.")
19
Mechanisms to resist and repair damage
Zelluläre Endokrinologische Lifestyle, Therapeutische (Hormonersatz, HRT, Alternatives)
")
20
Menopause Sympome infolge Östrogen- Ausfall und -Entzug
Klimakterische Beschwerden Schweißausbrüche Müdigkeit Schlaflosigkeit Nervosität Herzrasen Depressive Verstimmungen Urogenitale Atrophie Atrophische Veränderungen des Harntrakts und ihre Folgen (z.B. vaginale Trockenheit, Dyspareunie, häufiges Wasserlassen und Harndrang)
")
21
Wenn uns Verzweiflung überkommt, liegt das gewöhnlich daran, dass wir zu viel an die Vergangenheit und an die Zukunft denken Hl Therese von Lisieux

22
Östrogen- Ausfall und/oder –Entzug Wie reagiert das Hormonsystem?
= Stress Wie reagiert das Hormonsystem?

23
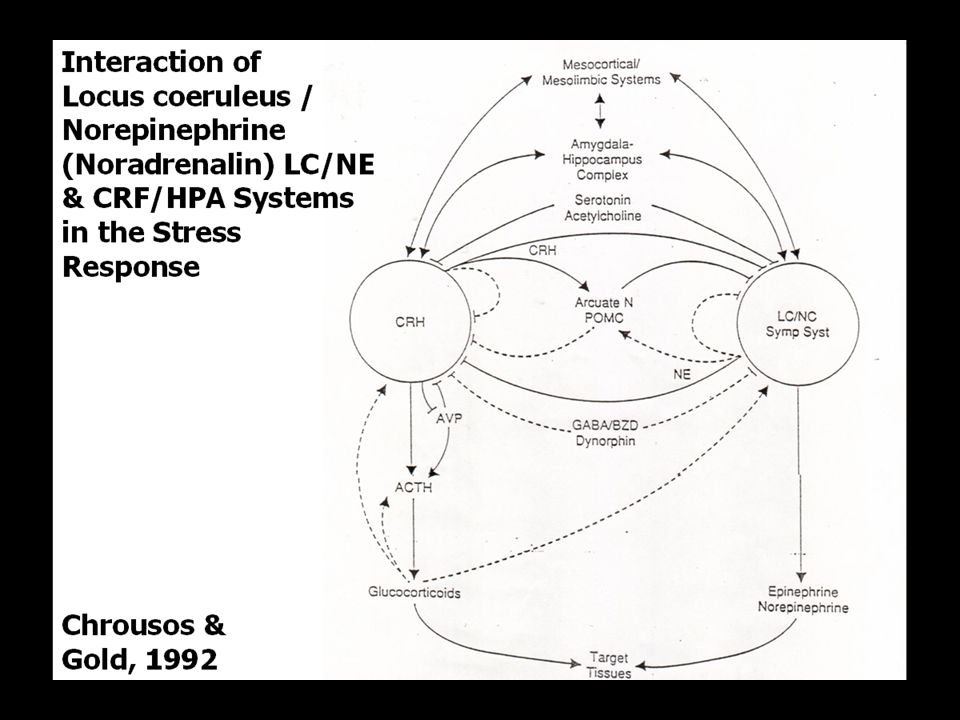
- + SUMMARY OF HORMONE PHYSIOLOGY Higher Centers Pituitary Liver
Neural activity (neurotransmitters) Hypothalamus Releasing Factors Pituitary posterior anterior Trophic Hormones LH FSH ACTH TSH Liver Fat Thyroid GH Peripheral Hormones IGF-I - Adrenal + Bone Cartilage Muscle Testis Ovary Gonads
 Hypothalamus. Releasing Factors. Pituitary. posterior. anterior. Trophic. Hormones. LH. FSH. ACTH. TSH. Liver. Fat. Thyroid. GH. Peripheral. Hormones. IGF-I. - Adrenal. + Bone. Cartilage. Muscle. Testis. Ovary. Gonads.")
24
T4 80% T3 20% aktives Hormon Konversion zu T3 peripher
SUMMARY OF HORMONE PHYSIOLOGY Higher Centers Neural activity (neurotransmitters) Hypothalamus Releasing Factors Pituitary posterior anterior Trophic Hormones LH FSH ACTH TSH Thyroid T4 80% T3 20% aktives Hormon Konversion zu T3 peripher
 Hypothalamus. Releasing Factors. Pituitary. posterior. anterior. Trophic. Hormones. LH. FSH. ACTH. TSH. Thyroid. T4 80% T3 20% aktives Hormon. Konversion. zu T3 peripher.")
26
Control of androgen secretion

29
- - -

30
- -

31
- -

32
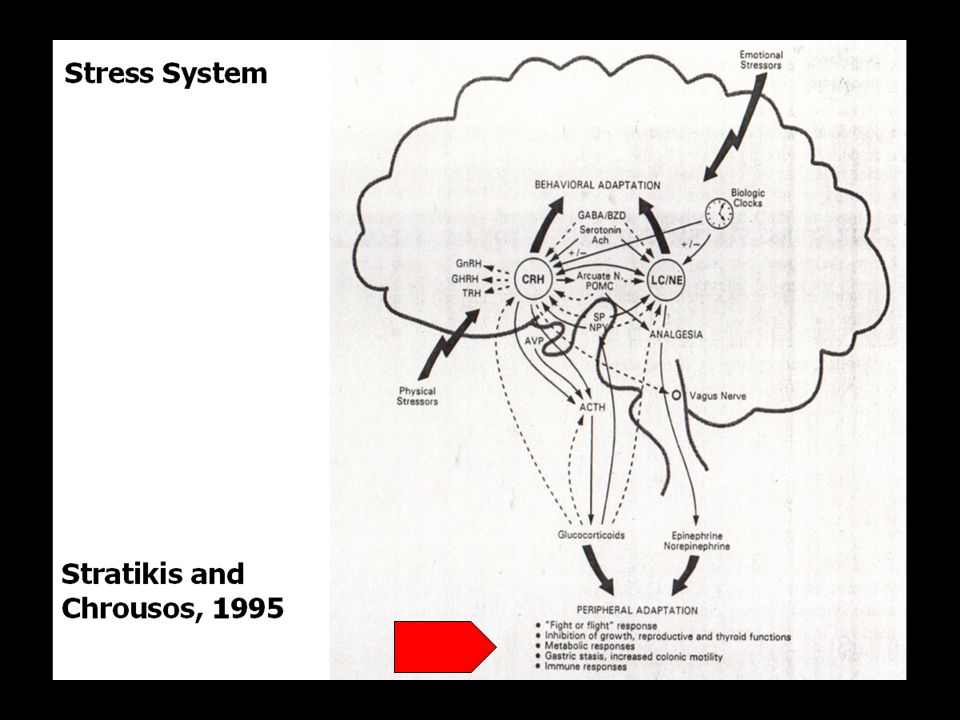
(physischer) Stress und endokrines System, Zusammenfassung
(physischer) Stress führt zu Arousal der CRF-HPA-Achse vermehrter Cortisol-Produktion sekundärem Abfall von Testosteron (und Östradiol, Anstieg von Prolaktin, nicht gezeigt) und Wachstumshormon Verminderter Produktion (d. Konversion) von aktivem Schilddrüsen-Hormon T3
 Stress führt zu. Arousal der CRF-HPA-Achse. vermehrter Cortisol-Produktion. sekundärem Abfall von Testosteron (und Östradiol, Anstieg von Prolaktin, nicht gezeigt) und Wachstumshormon. Verminderter Produktion (d. Konversion) von aktivem Schilddrüsen-Hormon T3.")
33
Östrogen- Ausfall und/oder –Entzug
Wie reagiert der Körper (body composition)?
")
34
Age-related Changes in Body Composition and Function

35
Age-related Changes in Body Composition and Function
Loss of lean body (muscle) mass Decreased strength Decreased fitness and loss of functional capacity Increase in total fat mass (percent body fat) Insulin resistance (type 2 diabetes) Increased LDL cholesterol, triglycerides, and fatty acids Decreased bone density (negative calcium balance) Metabolic/Physiologic Function Decreased protein synthesis Slower healing Reduced immune system function Altered hormone balance
 mass. Decreased strength. Decreased fitness and loss of functional capacity. Increase in total fat mass (percent body fat) Insulin resistance (type 2 diabetes) Increased LDL cholesterol, triglycerides, and fatty acids. Decreased bone density (negative calcium balance) Metabolic/Physiologic Function. Decreased protein synthesis. Slower healing. Reduced immune system function. Altered hormone balance.")
36
Age-related Changes in Body Composition in Normal Sedentary Men
Muscle Mass (lbs) 70 Fat (%) 60 50 Body Composition 40 30 20 10 20 30 40 50 60 70 80 Age (years) (Balagopal et al. Endocrine 7:57, 1997)
 70. Fat (%) Body Composition Age (years) (Balagopal et al. Endocrine 7:57, 1997)")
37
Decreases in Muscle Strength with Age
Men 250 Women 200 Isokinetic Force (Nm) 150 100 10 20 30 40 50 60 70 80 Age (years) (Borges, Scand J Rehabil Med 21:45, 1989)
 Age (years) (Borges, Scand J Rehabil Med 21:45, 1989)")
38
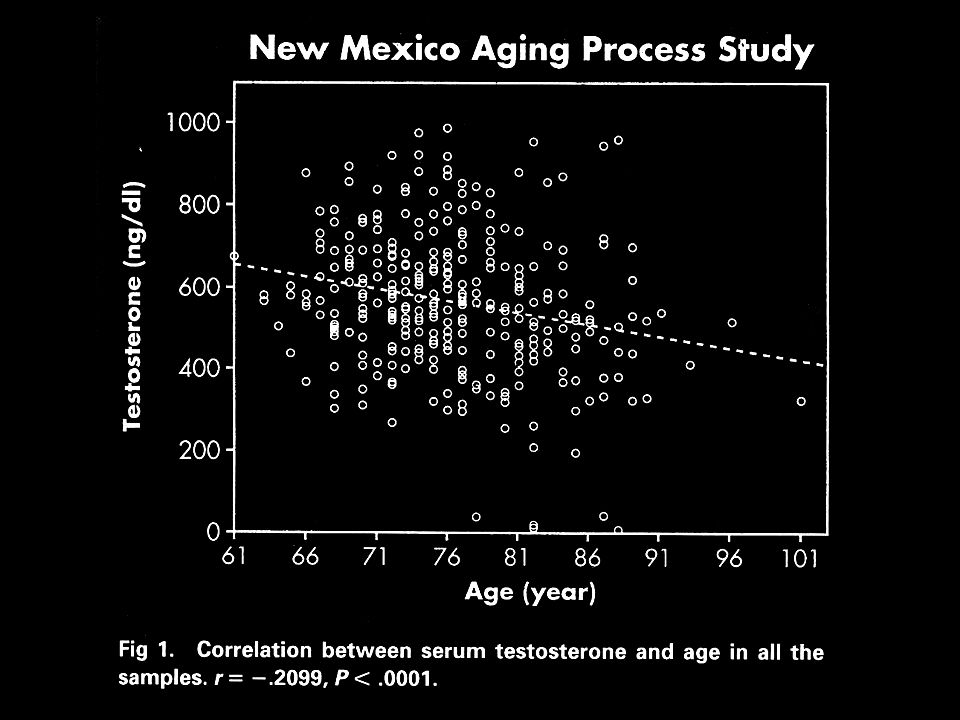
Altern wir, weil die Menge wichtiger Hormone abnimmt?
Oder: nimmt die Hormonkonzentration ab, weil wir altern?

39
How Do Hormones Change with Normal Aging?
Estrogens- decrease to very low levels over a 1-3 year period at menopause (between ages 45-55) Testosterone (T)- Gradual decline from age 30 onward reaching low (hypogonadal) levels in >20% of men by age 65 Growth Hormone (GH)- Gradual decrease in secretion (and circulating IGF-I levels) from age 45-90
 Testosterone (T)- Gradual decline from age 30 onward reaching low (hypogonadal) levels in >20% of men by age 65. Growth Hormone (GH)- Gradual decrease in secretion (and circulating IGF-I levels) from age")
40
How Do Hormones Change with Normal Aging?
Adrenal Steroids- Active adrenal hormones (cortisol and aldosterone) change little DHEA, steady decrease with age to very low levels in both sexes Thyroid- not much change in healthy men and women, but increased prevalence of hypothyroid disease in older persons. Insulin- loss of sensitivity to insulin action with aging and obesity
 change little. DHEA, steady decrease with age to very low levels in both sexes. Thyroid- not much change in healthy men and women, but increased prevalence of hypothyroid disease in older persons. Insulin- loss of sensitivity to insulin action with aging and obesity.")
41
Mechanisms to resist and repair damage
Zelluläre Endokrinologische Lifestyle, Therapeutische (Hormonersatz, HRT, Alternatives)
")
42
Wichtigste Lifestyle-Massnahme
Wer die Nacht nicht ehrt, ist des Tages nicht wert Italienisches Sprichwort

43
Effects of Aging on Growth Hormone Secretion in Men
15 Young 10 5 Growth Hormone (ng/ml) 8:00 am 12:00 pm 4:00 pm 8:00 pm 12:00 am 4:00 am 8:00 am Time (Corpas, et al., J Clin Endocrinol Metab 75:530, 1992)
 8:00 am. 12:00 pm. 4:00 pm. 8:00 pm. 12:00 am. 4:00 am. 8:00 am. Time. (Corpas, et al., J Clin Endocrinol Metab 75:530, 1992)")
44
Gibt es sonst was zu tun, ausser viel schlafen? Müller’sche Frage

45
The International Menopause Society
The IMS Updated Recommendations on postmenopausal hormone therapy February 27, 2007 Climacteric 2007;10:181–94 45

46
Exercise in the menopause
Any physical activity is better than being sedentary Regular exercise reduces total and cardiovascular mortality Better metabolic profile, balance, muscle strength, cognition and quality of life are observed in physically active persons. Heart events, stroke, fractures and breast cancer are significantly less frequent Benefits far outweigh possible adverse consequences: the more – the better, but too much may cause harm Summarizing the topic of exercise in the menopause, here are my conclusions: 46

47
Exercise in the menopause: optimal exercise prescription
At least 30 minutes of moderate intensity exercise, at least three times weekly Two additional weekly training sessions of resistance exercise may provide further benefit What is the optimal exercise prescription? Thank you for your kind attention 47

48
AHA 2006 Diet and Lifestyle Recommendations 1
Balance calorie intake and physical activity to achieve or maintain a healthy body weight Consume a diet rich in vegetables and fruits Choose whole-grain, high-fiber foods Consume fish, especially oily fish, at least twice a week Circulation 2006;114:82 48

49
AHA 2006 Diet and Lifestyle Recommendations 2
Limit intake of saturated fat to < 7% of energy, trans fat to < 1% and cholesterol to < 300 mg/day by choosing lean meats and vegetable alternatives, selecting fat-free, 1% fat and low-fat products Choose and prepare foods with little or no salt Increase fiber intake (beans, whole grain, other fruits and vegetables) If you consume alcohol, do so in moderation Quit smoking Circulation 2006;114:82 49
 If you consume alcohol, do so in moderation. Quit smoking. Circulation 2006;114:")
50
Mechanisms to resist and repair damage
Zelluläre Endokrinologische Lifestyle, Therapeutische (Hormonersatz, HRT, Alternatives)
")
51
Indikationen für eine HRT
Klimakterische Beschwerden Schweißausbrüche Müdigkeit Schlaflosigkeit Nervosität Herzrasen Depressive Verstimmungen Urogenitale Atrophie Atrophische Veränderungen des Harntrakts und ihre Folgen (z.B. vaginale Trockenheit, Dyspareunie, häufiges Wasserlassen und Harndrang) Topische niedrig dosierte Präparate sind die Behandlung der Wahl, wenn lediglich lokale Beschwerden auftreten. Die Therapie klimakterischer Beschwerden erhält die Lebensqualität
 Topische niedrig dosierte Präparate sind die Behandlung der Wahl, wenn lediglich lokale Beschwerden auftreten. Die Therapie klimakterischer Beschwerden erhält die Lebensqualität.")
52
Praktische Empfehlungen zur Hormonersatztherapie in der Peri- und Postmenopause
Menopausale Einschätzung: Symptome (Hitzewallungen, Schweißausbrüche, Schlaflosigkeit, Müdigkeit, Reizbarkeit, Nervosität, depressive Verstimmungen, Urogenitalatrophie), körperliche Untersuchung (Gewicht, Knochendichte), persönliche und Familienanamnese, Risiko/Nutzen-Analyse (Osteoporose, tiefe Venenthrombose, Brustkrebs, koronare Herzerkrankung) Symptome, aber HRT kontraindiziert Nur urogenitale Atrophie Menopausale Symptome Erhöhtes Osteoporoserisiko/Frakturen bei asymptomatischen Frauen Möglich sind: Phytoestrogene α-adrenerge Agonisten Hoch dosierte Gestagene Selektive Serotonin-Wiederaufnahmehemmer (SSRI) Gabapentin Kein Uterus intakter Uterus Muskelaufbautraining nicht rauchen Calcium/Vitamin D + HRT als erste Option Gefolgt von SERM und/oder Bisphosphonat und Teriparatid Peri-meno-pausal Post-meno-pausal Topisches niedrig dosiertes vaginales Estrogen Niedrig dosierte Estrogenmonotherapie Niedrig dosiertes orales Kontrazeptivum Niedrig dosierte sequentiell kombinierte (sc) gestagenbetonte HRT zyklische Gestagengabe (2. Zyklushälfte) Niedrig dosierte kontinuierlich kombinierte (cc) HRT Neueinschätzung nach 8-12 Wochen Therapie, u.U. Dosisanpassung Jährliche Neubewertung von nach lokalen Richtlinien: ۰ Indikation ۰ Mammographie** ۰ Dosis ۰ Vaginaler Ultraschall und/oder Endometriumbiopsie ۰ Therapieregime* ۰ Knochendichtemessung ۰ Risiko/Nutzenanalyse Vorzeitige Menopause Frauen mit vorzeitiger Menopause sollte routinemäßig eine HRT zumindest bis zum durchschnittlichen Menopausealter (51 Jahre) angeboten werden. *zu überlegen ist Umstellung auf ccHRT bei postmenopausalen Frauen regulären Entzugsblutungen Frauen ohne irreguläre Blutungen unter scHRT oder Frauen ohne Blutung unter scHRT **Einige Frauen können eine erhöhte mammographische Dichte entwickeln, insbesondere unter einer höher dosierten kontinuierlich-kombinierten HRT. Um bei solchen Patientinnen diagnostische Probleme zu vermeiden, kann ein Absetzen der HRT für 2-4 Wochen vor der Mammographie in Erwägung gezogen werden.
, körperliche Untersuchung (Gewicht, Knochendichte), persönliche und Familienanamnese, Risiko/Nutzen-Analyse (Osteoporose, tiefe Venenthrombose, Brustkrebs, koronare Herzerkrankung) Symptome, aber HRT kontraindiziert. Nur urogenitale Atrophie. Menopausale Symptome. Erhöhtes Osteoporoserisiko/Frakturen bei asymptomatischen Frauen. Möglich sind: Phytoestrogene. α-adrenerge Agonisten. Hoch dosierte Gestagene. Selektive Serotonin-Wiederaufnahmehemmer (SSRI) Gabapentin. Kein Uterus. intakter Uterus. Muskelaufbautraining. nicht rauchen. Calcium/Vitamin D. + HRT als erste Option. Gefolgt von SERM und/oder Bisphosphonat und Teriparatid. Peri-meno-pausal. Post-meno-pausal. Topisches niedrig dosiertes vaginales Estrogen. Niedrig dosierte Estrogenmonotherapie. Niedrig dosiertes orales Kontrazeptivum Niedrig dosierte sequentiell kombinierte (sc) gestagenbetonte HRT zyklische Gestagengabe (2. Zyklushälfte) Niedrig dosierte kontinuierlich kombinierte (cc) HRT. Neueinschätzung nach 8-12 Wochen Therapie, u.U. Dosisanpassung. Jährliche Neubewertung von nach lokalen Richtlinien: ۰ Indikation ۰ Mammographie** ۰ Dosis ۰ Vaginaler Ultraschall und/oder Endometriumbiopsie ۰ Therapieregime* ۰ Knochendichtemessung ۰ Risiko/Nutzenanalyse. Vorzeitige Menopause Frauen mit vorzeitiger Menopause sollte routinemäßig eine HRT zumindest bis zum durchschnittlichen Menopausealter (51 Jahre) angeboten werden. *zu überlegen ist Umstellung auf ccHRT bei. postmenopausalen Frauen. regulären Entzugsblutungen. Frauen ohne irreguläre Blutungen unter scHRT. oder. Frauen ohne Blutung unter scHRT. **Einige Frauen können eine erhöhte mammographische Dichte entwickeln, insbesondere unter einer höher dosierten kontinuierlich-kombinierten HRT. Um bei solchen Patientinnen diagnostische Probleme zu vermeiden, kann ein Absetzen der HRT für 2-4 Wochen vor der Mammographie in Erwägung gezogen werden.")
53
Zusammenfassung HRT Die Hormonersatztherapie sollte nur verordnet werden, wenn eine klare Indikation besteht (primär zur Behandlung klimakterischer Beschwerden). Es gibt keine wirksamen Alternativen zur Behandlung vasomotorischer Symptome. Die Hormonsubstitution kann bei Frauen mit erhöhtem Frakturrisiko eine Anfangsoption zur Senkung des Frakturrisikos darstellen. Die langfristige Hormonsubstitution ist mit einigen zusätzlichen Risiken verbunden. Venöse thromboembolische Erkrankungen Schlaganfall Brustkrebs (nur bei Normalgewicht) Die Indikation zur Fortsetzung der Hormonbehandlung sollte jährlich überprüft werden.
. Es gibt keine wirksamen Alternativen zur Behandlung vasomotorischer Symptome. Die Hormonsubstitution kann bei Frauen mit erhöhtem Frakturrisiko eine Anfangsoption zur Senkung des Frakturrisikos darstellen. Die langfristige Hormonsubstitution ist mit einigen zusätzlichen Risiken verbunden. Venöse thromboembolische Erkrankungen. Schlaganfall. Brustkrebs (nur bei Normalgewicht) Die Indikation zur Fortsetzung der Hormonbehandlung sollte jährlich überprüft werden.")
54
Zu den Risiken einer HRT
Die Indikation zur Fortsetzung der Hormonbehandlung sollte jährlich überprüft werden Unter besonderer Beachtung der Risiken einer HRT

55
HRT Credo HRT bedeutet Substitution des fehlenden körpereigenen Hormons in subphysiologischer Dosis. Die Evolution hat nicht eingeplant, dass die Lebenserwartung so ansteigt Hätten Männer einen so starken klimakterischen Hormonabfall, gäbe es für den Mann schon lange eine HRT. Männer haben höhere Östrogenspiegel als nicht behandelte postmenopausale Frauen.

56
HRT Credo Östrogene sind nicht mutagen oder cancerogen.
Östrogene wirken evtl. als Promotor auf vorhandene noch okkulte Mammacarcinome.

57
Inzidenz: Estrogene Inzidenz: Estrogen/Gestagen Mortalität
Bush et al Hormontherapie und Mammakarzinomrisiko 0, 0, 0, I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I Inzidenz: Estrogene Inzidenz: Estrogen/Gestagen Mortalität

58
HRT Credo Östrogene erhöhen bei genetisch praedisponierten Patientinnen das Thromboembolierisiko.

59
WHI-Studie relative Risiken unter CEE oder CEE/MPA
Koronare Herzerkrankungen 0,91 ns 1,24 ns (im 1. Jahr 1,81*) Schlaganfall 1,39* 1,31* ischämisch 1,44* hämorrhagisch 0,82 ns Venöse Thromboembolien 1,33 ns 2,06* Übergewicht 3,80* Adipositas 5,61* Mammakarzinom 0,77 ns 1,24* Kolonkarzinom 1,08 0,61* Oberschenkelhals-Frakturen 0,66*
 Schlaganfall. 1,39* 1,31* ischämisch 1,44* hämorrhagisch 0,82 ns. Venöse Thromboembolien. 1,33 ns. 2,06* Übergewicht 3,80* Adipositas 5,61* Mammakarzinom. 0,77 ns. 1,24* Kolonkarzinom. 1,08. 0,61* Oberschenkelhals-Frakturen. 0,66*")
60
Relatives Risiko in der Nurses‘ Health Study
(NHS) und der WHI
 und der WHI.")
62
HRT Credo HRT stellt die beste und günstigste Therapie der Wechseljahresbeschwerden dar. Östrogene wirken osteoprotektiv. Östrogene reduzieren das Risiko kolorektaler Carcinome.

63
Mechanisms to resist and repair damage
Zelluläre Endokrinologische Lifestyle, Therapeutische (Hormonersatz, HRT, Alternatives)
")
64
Alternativen zur HRT Kräuterextrakte können klimakterische Beschwerden lindern – ähnlich wie ein Placebo. Phytoestrogene können die Knochenresorption verlangsamen; eine Senkung des Frakturrisikos wurde jedoch nicht gezeigt. a-adrenerge Agonisten (z.B. Clonidin) haben eine moderate Wirkung auf Hitzewallungen. hoch-dosierte Gestagene (5-10 mg NETA, mg MPA oder Megestrolacetat / Tag) führen zu einer wirksamen Reduktion der Hitzewallungen. Die Langzeit-Auswirkungen sind bisher nicht untersucht.
 haben eine moderate Wirkung auf Hitzewallungen. hoch-dosierte Gestagene (5-10 mg NETA, mg MPA oder Megestrolacetat / Tag) führen zu einer wirksamen Reduktion der Hitzewallungen. Die Langzeit-Auswirkungen sind bisher nicht untersucht.")
65
Alternativen zur HRT Tibolon bessert klimakterische Beschwerden und erhält den Knochen. Eine Senkung des Frakturrisikos konnte nicht gezeigt werden. Neuroaktive Medikamente (z.B. Selektive Serotonin-Wiederaufnahmehemmer: SSRIs) haben eine moderate Wirkung auf vasomoto-rische Beschwerden. Therapieversuch möglich, wenn eine HRT nicht geeignet ist. Gabapentin kann Hitzewallungen reduzieren.
 haben eine moderate Wirkung auf vasomoto-rische Beschwerden. Therapieversuch möglich, wenn eine HRT nicht geeignet ist. Gabapentin kann Hitzewallungen reduzieren.")
66
Conclusions Übe Nachsicht mit Störfällen

68
Zusammenfassung Menpause: subakuter Verlust der Ovarfunktion Endokrinologisch gesehen ein Absturz Zahlreiche Kompensations- und Reparaturmöglichkeiten:

69
Zusammenfassung Kompensations- und Reparaturmöglichkeiten: Lifestyle: Bewegung, Ernährung HRT (beachte die Packungsbeilage) Alternativen zur HRT

70
Zusammenfassung Absturz? Individuell gesehen Chance zu Veränderung / Persönlichkeitswachstum Zwingt zur Auseinandersetzung mit Thema Altern

71
Der wahre Sinn des Lebens besteht darin, Bäume zu pflanzen, unter deren Schatten man vermutlich selber nie sitzen wird Nelson Henderson

72
Übliches zur Menopause
Bruno Müller 3010 Bern

73
The International Menopause Society
The IMS Updated Recommendations on postmenopausal hormone therapy February 27, 2007 Climacteric 2007;10:181–94 73

74
Introducing The International Menopause Society The society for the study of all aspects of the climacteric in men and women Established in 1978 Registered as a non-profit organization in Geneva, Switzerland Central Office in Lancaster, UK 74

75
Introducing The International Menopause Society Officers and Board, 2005–2008
President: Amos Pines, Israel General Secretary: David Sturdee, UK Treasurer: Martin Birkhäuser, Switzerland Board members Mark Brincat, Malta Tobie De Villiers, South Africa Marco Gambacciani, Italy Kobchitt Limpaphayom, Thailand Frederick Naftolin, USA Santiago Palacios, Spain James Pickar, USA Regine Sitruk-Ware, USA Sven Skouby, Denmark Executive Director: Jean Wright, UK 75

76
Introducing The International Menopause Society The Society’s Journal, Climacteric
Editors-in-Chief: David W. Sturdee, UK and Alastair H. MacLennan, Australia Published in six issues per year plus Supplements Indexed in Index Medicus, Medline, Current Contents Impact factor: 2.299 11th of 52 journals in Obstetrics & Gynecology section 76

77
Introduction The following Recommendations express the views of the IMS on the principles of hormone therapy (HT) in the peri- and postmenopause periods Throughout the Recommendations, the term HT will be used to cover all therapies including estrogens, progestogens, combined therapies and tibolone The 2004 IMS Statement is still valid and serves as a basis for the current updated Recommendations Climacteric 2007;10:181–94 77
 in the peri- and postmenopause periods. Throughout the Recommendations, the term HT will be used to cover all therapies including estrogens, progestogens, combined therapies and tibolone. The 2004 IMS Statement is still valid and serves as a basis for the current updated Recommendations. Climacteric 2007;10:181–")
78
Introduction The IMS is aware of possible geographical variations related to different priorities of medical care, different prevalence of diseases, and country-specific attitudes of the public, the medical community and the health authorities toward menopause management, which may all impact on hormone therapy Climacteric 2007;10:181–94 78

79
Introduction The following recommendations, therefore, give a global and simple overview that serves as a common platform on issues related to the various aspects of hormone treatment These Recommendations were reviewed and discussed by representatives of more than 60 national and regional menopause societies from all continents These Recommendations can be easily adapted and modified according to local needs Climacteric 2007;10:181–94 79

80
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Hormone therapy should be part of an overall strategy including lifestyle recommendations regarding diet, exercise, smoking and alcohol for maintaining the health of postmenopausal women Climacteric 2007;10:181–94 80

81
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles HT must be individualized and tailored according to symptoms and the need for prevention, as well as personal and family history, results of relevant investigations, the woman’s preferences and expectations The risks and benefits of HT differ for women around the time of menopause compared to those for older women HT includes a wide range of hormonal products and routes of administration, with potentially different risks and benefits The term ‘class effect’, when associated with HT, is confusing and inappropriate Climacteric 2007;10:181–94 81

82
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Women experiencing spontaneous or iatrogenic menopause before the age of 45 and particularly before 40 are at higher risk for cardiovascular disease and osteoporosis They will benefit from hormone replacement, which should be given at least until the normal age of menopause Climacteric 2007;10:181–94 82

83
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Counseling should convey the benefits and risks of HT in simple terms, e.g. absolute numbers rather than as percentage changes from baseline expressed as a relative risk This allows a woman and her physician to make a well-informed decision about HT Climacteric 2007;10:181–94 83

84
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles HT should not be recommended without a clear indication for its use Climacteric 2007;10:181–94 84

85
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Women taking HT should have at least an annual consultation to include a physical examination, update of medical history, relevant laboratory and imaging investigations and a discussion on lifestyle There are no reasons to place mandatory limitations on the length of treatment Whether or not to continue therapy should be decided at the discretion of the well-informed hormone user and her health professional, dependent upon the specific goals and an objective estimation of benefits and risks Climacteric 2007;10:181–94 85

86
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Dosage should be titrated to the lowest effective dose Lower doses of HT than have been used routinely can maintain quality of life in a large proportion of users Long-term data on lower doses regarding fracture risk and cardiovascular implications are still lacking Climacteric 2007;10:181–94 86

87
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Progestogen should be added to systemic estrogen for all women with a uterus to prevent endometrial hyperplasia and cancer Natural progesterone and some progestogens have specific beneficial effects that could justify their use besides the expected actions on the endometrium Climacteric 2007;10:181–94 87

88
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Low-dose vaginal estrogens administered for the relief of urogenital atrophy do not require progestogen co-medication Direct delivery of progestogen to the endometrial cavity from the vagina or by an intrauterine system is logical and may minimize systemic effects Climacteric 2007;10:181–94 88

89
Part I. Governing principles
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part I. Governing principles Androgen replacement should be reserved for women with clinical signs and symptoms of androgen insufficiency In women with bilateral oophorectomy or adrenal failure, androgen replacement has significant beneficial effects, in particular on health-related quality of life and sexual function Climacteric 2007;10:181–94 89

90
Part II. Benefits of hormone therapy: General
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: General HT remains the most effective therapy for vasomotor and estrogen-deficient urogenital symptoms Other menopause-related complaints, such as joint and muscle pains, mood swings, sleep disturbances and sexual dysfunction (including reduced libido) may improve during HT Climacteric 2007;10:181–94 90
 may improve during HT. Climacteric 2007;10:181–")
91
Part II. Benefits of hormone therapy: General
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: General Quality of life and sexuality are key factors to be considered in the management of the aging individual The administration of individualized HT (including androgenic preparations when appropriate) improves both sexuality and overall quality of life Climacteric 2007;10:181–94 91
 improves both sexuality and overall quality of life. Climacteric 2007;10:181–")
92
Part II. Benefits of hormone therapy: Postmenopausal osteoporosis
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: Postmenopausal osteoporosis HT is effective in preventing the bone loss associated with the menopause and decreases the incidence of all osteoporosis-related fractures, including vertebral and hip, even in patients at low risk Although the magnitude of decline in bone turnover correlates with estrogen dosage, even lower than standard-dose preparations maintain a positive influence on bone indices in most women Climacteric 2007;10:181–94 92

93
Part II. Benefits of hormone therapy: Postmenopausal osteoporosis
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: Postmenopausal osteoporosis HT is an appropriate first-line therapy in postmenopausal women presenting with an increased risk for fracture, particularly under the age of 60 years and for the prevention of bone loss in women with premature menopause The protective effect of HT on bone mineral density declines after cessation of therapy at an unpredictable rate, although some degree of fracture protection may remain after cessation of HT Climacteric 2007;10:181–94 93

94
Part II. Benefits of hormone therapy: Postmenopausal osteoporosis
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: Postmenopausal osteoporosis The initiation of standard-dose HT is not recommended for the sole purpose of the prevention of fractures after the age of 60 years The continuation of HT after the age of 60 for the sole purpose of the prevention of fractures should take into account the possible long-term effects of the specific dose and method of administration of HT, compared to other proven therapies Climacteric 2007;10:181–94 94

95
Part II. Benefits of hormone therapy: Cardiovascular disease
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: Cardiovascular disease Cardiovascular disease is the principal cause of morbidity and mortality in postmenopausal women Major primary prevention measures (besides smoking cessation, and diet control) are weight loss, blood pressure reduction, and diabetes and lipid control There is evidence that HT may be cardioprotective if started around the time of menopause and continued long-term (often referred to as the ‘window of opportunity’ concept) Climacteric 2007;10:181–94 95
 are weight loss, blood pressure reduction, and diabetes and lipid control. There is evidence that HT may be cardioprotective if started around the time of menopause and continued long-term (often referred to as the ‘window of opportunity’ concept) Climacteric 2007;10:181–")
96
Part II. Benefits of hormone therapy: Cardiovascular disease
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: Cardiovascular disease HT markedly reduces the risk of diabetes and, through improved insulin resistance, it has positive effects on other related risk factors for cardiovascular disease such as the lipid profile and metabolic syndrome In women less than 60 years old, recently menopausal, without prevalent cardiovascular disease, the initiation of HT does not cause early harm, and may reduce cardiovascular morbidity and mortality Continuation of HT beyond the age of 60 should be decided as a part of the overall risk-benefit analysis Climacteric 2007;10:181–94 96

97
Part II. Benefits of hormone therapy: Other
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part II. Benefits of hormone therapy: Other HT may reduce the risk of colon cancer HT initiated around the time of menopause or by younger postmenopausal women is associated with a reduced risk of Alzheimer’s disease HT has benefits for connective tissue, skin, joints and intervertebral disks Climacteric 2007;10:181–94 97

98
Part III. Potential serious adverse effects of HT
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part III. Potential serious adverse effects of HT Studies on the risks of postmenopausal hormone use have mainly focused on breast and endometrial cancer, venous thromboembolism (pulmonary embolism or deep vein thrombosis), stroke and coronary events Climacteric 2007;10:181–94 98
, stroke and coronary events. Climacteric 2007;10:181–")
99
Part III. Potential serious adverse effects of HT: Breast cancer
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part III. Potential serious adverse effects of HT: Breast cancer The incidence of breast cancer varies in different countries. Therefore, currently available data cannot necessarily be generalized Climacteric 2007;10:181–94 99

100
Part III. Potential serious adverse effects of HT: Breast cancer
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part III. Potential serious adverse effects of HT: Breast cancer The degree of association between breast cancer and postmenopausal HT remains controversial. Women should be reassured that the possible risk of breast cancer associated with HT is small (less than 0.1% per annum) Climacteric 2007;10:181–94 100
 Climacteric 2007;10:181–")
101
Part III. Potential serious adverse effects of HT: Breast cancer
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part III. Potential serious adverse effects of HT: Breast cancer For combined HT, observational data from the Million Women Study suggested that breast cancer risk was increased as early as the first year, raising serious reservations on possible methodologic flaws On the contrary, randomized controlled data from the Women‘s Health Initiative (WHI) Study indicate that no increased risk is observed in women initiating HT, for up to 7 years. It should be noted that the majority of subjects in the WHI Study were overweight or obese Climacteric 2007;10:181–94 101
 Study indicate that no increased risk is observed in women initiating HT, for up to 7 years. It should be noted that the majority of subjects in the WHI Study were overweight or obese. Climacteric 2007;10:181–")
102
Part III. Potential serious adverse effects of HT: Breast cancer
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part III. Potential serious adverse effects of HT: Breast cancer Data from the WHI and Nurses’ Health Study suggest that long-term estrogen-only administration for 7 and 15 years, respectively, does not increase the risk of breast cancer in American women. Recent European observational studies suggest that risk may increase after 5 years There are insufficient data to evaluate the possible differences in the incidence of breast cancer using different types and routes of estrogen, natural progesterone and progestogens, and androgen administration Climacteric 2007;10:181–94 102

103
Part III. Potential serious adverse effects of HT: Breast cancer
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part III. Potential serious adverse effects of HT: Breast cancer Baseline mammographic density correlates with breast cancer risk. This does not necessarily apply to the increase in mammographic density induced by HT The combined estrogen–progestogen therapy-related increase in mammographic density may impede the diagnostic interpretation of mammograms Climacteric 2007;10:181–94 103

104
Part III. Potential serious adverse effects of HT: Endometrial cancer
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part III. Potential serious adverse effects of HT: Endometrial cancer Unopposed estrogen administration induces a dose-related stimulation of the endometrium Women with a uterus should have progestogen supplementation Continuous combined estrogen–progestogen regimens are associated with a lower incidence of endometrial hyperplasia and cancer than occurs in the normal population Direct intrauterine delivery systems may have advantages Regimens containing low-/ultra-low-dose estrogen and progestogen cause less endometrial stimulation and less bleeding Climacteric 2007;10:181–94 104

105
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY
Part III. Potential serious adverse effects of HT: Thromboembolism and cardiovascular events The HT-related risk for serious venous thromboembolic events increases with age (although minimal until age 60) and is also positively associated with obesity and thrombophilia By avoiding first-pass hepatic metabolism, transdermal estrogen may avert the risk associated with oral HT The impact on the risk of a thromboembolic event may also be affected by progestogen, depending on the type Climacteric 2007;10:181–94 105
 and is also positively associated with obesity and thrombophilia. By avoiding first-pass hepatic metabolism, transdermal estrogen may avert the risk associated with oral HT. The impact on the risk of a thromboembolic event may also be affected by progestogen, depending on the type. Climacteric 2007;10:181–")
106
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY
Part III. Potential serious adverse effects of HT: Thromboembolism and cardiovascular events Late starters of standard-dose HT may have a transient slightly increased risk for coronary events The risk of stroke is correlated with age. HT may increase the risk of stroke after the age of 60 Safety data from studies of low-dose and ultra-low-dose regimens of estrogen and progestogen are encouraging Climacteric 2007;10:181–94 106

107
Part IV: Alternative treatments
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part IV: Alternative treatments The efficacy and safety of complementary alternative medicines have not been demonstrated and further studies are required Selective serotonin reuptake inhibitors, selective noradrenaline reuptake inhibitors and gabapentin are effective in reducing vasomotor symptoms in short-term studies. Their long-term safety needs further evaluation Climacteric 2007;10:181–94 107

108
Part IV: Alternative treatments
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part IV: Alternative treatments There are no medical or scientific reasons to recommend unregistered ‘bioidentical hormones’ The measurement of hormone levels in the saliva is not clinically useful These ‘customized’ hormonal preparations have not been tested in studies, and their purity and risks are unknown Climacteric 2007;10:181–94 108

109
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY
Part V: Conclusions There is urgent need for further research, especially into the relative merits of lower doses, regimens and routes of administration Climacteric 2007;10:181–94 109

110
Part V: Conclusions The safety of HT largely depends on age
IMS UPDATED RECOMMENDATIONS ON POSTMENOPAUSAL HORMONE THERAPY Part V: Conclusions The safety of HT largely depends on age Women younger than 60 years should not be concerned about the safety profile of HT New data and re-analyses of older studies by women’s age show that, for most women, the potential benefits of HT given for a clear indication are many and the risks are few when initiated within a few years of menopause Climacteric 2007;10:181–94 110

111
Adjunctive slides The following slides may be useful for presentation in regard to the IMS Recommendations Some slides demonstrate data on which the statements are based. This is not, however, a full slide presentation on specific topics. The IMS is now in the process of developing an Educational Slide Kit on the main issues of adult women’s health and menopause 111

112
Dose response to estrogen therapy Number of moderate–severe hot flushes
80 70 60 50 40 30 20 10 Placebo 0.25 mg E2 0.5 mg E2 1 mg E2 2 mg E2 Significantly (p < 0.05) different from placebo * Number * * * * * * Adapted from Notelovitz M, et al. Obstet Gynecol 2000;95:726 112
 different from placebo. * Number. * * * * * * Adapted from Notelovitz M, et al. Obstet Gynecol 2000;95:")
113
Ultra-low-dose oral therapy Effect on number of moderate to severe hot flushes by week
* significantly (p = 0.001) different from placebo * * * * * * * * * * Adapted from Panay N, et al. Climacteric 2007;10:120–31 113
 different from placebo. * * * * * * * * * * Adapted from Panay N, et al. Climacteric 2007;10:120–")
114
HOPE Study Number of hot flushes in 13 cycles
10 CEE CEE/MPA Placebo Placebo 0.625 0.625/2.5 0.45 8 0.45/2.5 0.3 0.45/1.5 0.3/1.5 Mean number 6 4 2 1 2 3 4 5 6 7 8 9 10 11 12 13 Cycle * compared to basal levels basal level: mean incidence of hot flushes = 12.3 (11.3–13.8) Level I Adapted from Utian W, et al. Fertil Steril 2001;75:1065–79 114
 Level I. Adapted from Utian W, et al. Fertil Steril 2001;75:1065–")
115
Women's HOPE Study Changes in severity of hot flushes over 12 weeks (n = 241)
Placebo Placebo 0.625/2.5 0.625 0.45/2.5 0.45 0.45/1.5 0.3 0.3/1.5 Patients also reported the severity of their vasomotor symptoms by rating each hot flush as mild (1 point), moderate (2 points), or severe (3 points) and recording the hot flush score on their daily diary cards. Mild hot flushes were defined as a fleeting warm sensation without sweating that did not disrupt activity. Moderate hot flushes were defined as warm sensations with sweating that did not disrupt activity, and severe hot flushes were defined as hot sensations with sweating that did disrupt activity. Daily hot flush severity scores were calculated using the following equation: [(# of mild flushes 1) + (# of moderate hot flushes 2) + (# of severe hot flushes 3)] ÷ total of # hot flushes on that day. Treatment with all active study regimens resulted in significant decreases from baseline (P < .001) by the second week of treatment. Significant differences from baseline were observed in the placebo group by week 3 (P < .05). By the third week of treatment, all CEE and CEE/MPA groups reported significantly lower mean daily severity of hot flushes compared with placebo (P < .05). The benefits of CEE and CEE/MPA in reducing hot flush severity were maintained throughout the course of the study. Hot flush severity: 1 = mild, 2 = moderate, 3 = severe. Mean hot flush severity at baseline = 2.3 (range 2.2–2.4). EE = Efficacy-evaluable population included women who recorded taking study medication and had at least 7 moderate-to-severe flushes/week or at least 50 flushes per week at baseline Adapted from Utian W, et al. Fertil Steril 2001;75:1065–79 115 Utian WH, et al. Fertil Steril. 2001;75:
, moderate (2 points), or severe (3 points) and recording the hot flush score on their daily diary cards. Mild hot flushes were defined as a fleeting warm sensation without sweating that did not disrupt activity. Moderate hot flushes were defined as warm sensations with sweating that did not disrupt activity, and severe hot flushes were defined as hot sensations with sweating that did disrupt activity. Daily hot flush severity scores were calculated using the following equation: [(# of mild flushes 1) + (# of moderate hot flushes 2) + (# of severe hot flushes 3)] ÷ total of # hot flushes on that day. Treatment with all active study regimens resulted in significant decreases from baseline (P < .001) by the second week of treatment. Significant differences from baseline were observed in the placebo group by week 3 (P < .05). By the third week of treatment, all CEE and CEE/MPA groups reported significantly lower mean daily severity of hot flushes compared with placebo (P < .05). The benefits of CEE and CEE/MPA in reducing hot flush severity were maintained throughout the course of the study. Hot flush severity: 1 = mild, 2 = moderate, 3 = severe. Mean hot flush severity at baseline = 2.3 (range 2.2–2.4). EE = Efficacy-evaluable population included women who recorded taking study medication and had at least 7 moderate-to-severe flushes/week or at least 50 flushes per week at baseline. Adapted from Utian W, et al. Fertil Steril 2001;75:1065– Utian WH, et al. Fertil Steril. 2001;75:")
116
Unopposed ultra-low-dose transdermal estradiol
417 postmenopausal women (60–80 years) mean 67 ± 5 years Randomly assigned to placebo or transdermal 14 µg/day for 2 years Baseline serum E2 = 4.8 pg/ml On treatment E2 = 8.6 pg/ml Johnson SR, et al. Obstet Gynecol 2005;105:779–87 116
 mean 67 ± 5 years. Randomly assigned to placebo or transdermal 14 µg/day for 2 years. Baseline serum E2 = 4.8 pg/ml. On treatment E2 = 8.6 pg/ml. Johnson SR, et al. Obstet Gynecol 2005;105:779–")
117
Unopposed ultra-low-dose transdermal estradiol
Endometrial effects: Proliferation % vs. 1.1% p = 0.6 Bleeding % vs. 8.6% p = 0.3 Atypical hyperplasia × 1 Adenosarcoma × 1 Conclusions: ‘This therapy apparently causes little or no endometrial stimulation’ Johnson SR, et al. Obstet Gynecol 2005;105:779–87 117

118
WHI population characteristics
WHI EP arm WHI E arm Mean % Mean % Age (years) < – – Body mass index < – > Hypertensive Rossouw JE, et al. J Am Med Assoc 2002;288:321–33 The Women’s Health Initiative Steering Committee. J Am Med Assoc 2004;291:1701–12 118
 < – – Body mass index < – > Hypertensive Rossouw JE, et al. J Am Med Assoc 2002;288:321–33. The Women’s Health Initiative Steering Committee. J Am Med Assoc 2004;291:1701–")
119
Fracture risk in the WHI study
Hazard ratio (95% CI) Estrogen + progestin Estrogen hormone therapy hormone therapy Hip 0.67 (0.47–0.96)* 0.61 (0.41–0.91)* Vertebral 0.65 (0.46–0.92)* 0.62 (0.42–0.93)* Total 0.76 (0.69–0.83)* 0.70 (0.63–0.79)* The WHI trial was the first large RCT to prove that HT reduces the risk of all osteoporosis related fractures, even in patients at low risk of fracture The risk reduction was highly significant and comparable to most other bone specific drugs * significant Adapted from JAMA 2003;290:1729 and JAMA 2004;291:1701 119
 Estrogen + progestin Estrogen hormone therapy hormone therapy. Hip 0.67 (0.47–0.96)* 0.61 (0.41–0.91)* Vertebral 0.65 (0.46–0.92)* 0.62 (0.42–0.93)* Total 0.76 (0.69–0.83)* 0.70 (0.63–0.79)* The WHI trial was the first large RCT to prove that HT reduces the risk of all osteoporosis related fractures, even in patients at low risk of fracture The risk reduction was highly significant and comparable to most other bone specific drugs. * significant. Adapted from JAMA 2003;290:1729 and JAMA 2004;291:")
120
WHI: unopposed estrogen
Placebo (n = 5196) Hazard ratio (95% CI) p Total joint replacement 119 169 0.73 (0.58–0.93) 0.01 Hip joint replacement 28 53 0.55 (0.35–0.88) Knee joint 93 121 0.8 (0.61–1.05) 0.11 Compliance more than 80% Adapted from Cirillo, et al. Arthritis Rheumatism 2006 120
 Hazard ratio. (95% CI) p. Total joint. replacement (0.58–0.93) Hip joint replacement (0.35–0.88) Knee joint (0.61–1.05) Compliance more than 80% Adapted from Cirillo, et al. Arthritis Rheumatism")
121
WHI results: effect of HT on risk of colorectal cancer
Kaplan–Meier estimate HR = % nCI = 0.38– % aCI = 0.33–0.94 Placebo E + P In the WHI, 43 invasive colorectal cancers occurred in the E+P group during an average of 5.6 years of follow-up, and 72 occurred in the placebo group (HR, 0.56; 95% nCI, 0.38–0.81; 95% aCI, 0.33–0.94). This figure shows the Kaplan-Meier plots of the cumulative hazard of invasive colorectal cancer for both the E+P and placebo groups. As indicated by the plots, the difference in incidence began to emerge early in the first year of follow-up, suggesting an effect on established cancers. The invasive colorectal cancers in the E+P and placebo groups were similar in location, tumor grade, and histologic features (ie, adenocarcinoma, not otherwise specified; in adenomatous polyp; in tubulovillous adenoma; or in villous adenoma). However, cancers in the E+P group had a greater number of positive lymph nodes (mean ± SD, 3.2 ± 4.1 vs 0.8 ± 1.7; P = .002), compared with placebo, and were more advanced (regional or metastatic disease, 76.2% vs 48.5%; P = .004). The reasons for these differences are unknown. Exploratory analyses indicated that among those women in the E+P group who were diagnosed with colorectal cancer, those with antecedent vaginal bleeding had cancers with a greater number of positive nodes, compared with those women who did not have vaginal bleeding (3.8±4.3 vs 0.7±1.5, P = .006). Abdominal pain, a change in bowel habits, and rectal bleeding are common symptoms in patients who present with colorectal cancer. The authors speculated that vaginal bleeding may have delayed some women from seeking care and may possibly account for the higher incidence of advanced cancer in the E+P group. Given this possibility, wider implementation of bowel screening among postmenopausal women using HT was recommended. Adapted from Chlebowski RT, et al. N Engl J Med 2004;350:991–1004 121 Chlebowski RT, et al. N Engl J Med. 2004;350:
. This figure shows the Kaplan-Meier plots of the cumulative hazard of invasive colorectal cancer for both the E+P and placebo groups. As indicated by the plots, the difference in incidence began to emerge early in the first year of follow-up, suggesting an effect on established cancers. The invasive colorectal cancers in the E+P and placebo groups were similar in location, tumor grade, and histologic features (ie, adenocarcinoma, not otherwise specified; in adenomatous polyp; in tubulovillous adenoma; or in villous adenoma). However, cancers in the E+P group had a greater number of positive lymph nodes (mean ± SD, 3.2 ± 4.1 vs 0.8 ± 1.7; P = .002), compared with placebo, and were more advanced (regional or metastatic disease, 76.2% vs 48.5%; P = .004). The reasons for these differences are unknown. Exploratory analyses indicated that among those women in the E+P group who were diagnosed with colorectal cancer, those with antecedent vaginal bleeding had cancers with a greater number of positive nodes, compared with those women who did not have vaginal bleeding (3.8±4.3 vs 0.7±1.5, P = .006). Abdominal pain, a change in bowel habits, and rectal bleeding are common symptoms in patients who present with colorectal cancer. The authors speculated that vaginal bleeding may have delayed some women from seeking care and may possibly account for the higher incidence of advanced cancer in the E+P group. Given this possibility, wider implementation of bowel screening among postmenopausal women using HT was recommended. Adapted from Chlebowski RT, et al. N Engl J Med 2004;350:991– Chlebowski RT, et al. N Engl J Med. 2004;350:")
122
Effect of HRT/ERT on CHD in postmenopausal women
Timing of initiation <10 0.56 1019 0.92 CEE > 20 1.04 Hazard ratio (95% CI) Hazard ratios Years since menopause <10 0.89 1019 1.22 CEE + MPA Notes Nevertheless, analysis of hazard ratio according to the years since menopause suggests a different effect according to the timing of hormone initiation, more evident in the estrogen-only arm of the WHI. References Petitti DB, Sidney S, Quesenberry CP Jr. Hormone replacement therapy and the risk of myocardial infarction in women with coronary risk factors. Epidemiology 2000;11:603–6 Grodstein F, Manson JE, Colditz GA, et al. A prospective, observational study of postmenopausal hormone therapy and primary prevention of cardiovascular disease. Ann Intern Med 2000;133:933–41 Ferrara A, Quesenberry CP, Karter AJ, et al. Current use of unopposed estrogen and estrogen plus progestin and the risk of acute myocardial infarction among women with diabetes: the Northern California Kaiser Permanente Diabetes Registry, 1995–1998. Circulation 2003;107:43–8 Herrington DM. Hormone replacement therapy and heart disease: replacing dogma with data. Circulation 2003;107:2–4 > 20 1.71 Hazard ratio (95% CI) Data from WHI 122
 Hazard. ratios. Years since. menopause. < CEE + MPA. Notes. Nevertheless, analysis of hazard ratio according to the years since menopause suggests a different effect according to the timing of hormone initiation, more evident in the estrogen-only arm of the WHI. References. Petitti DB, Sidney S, Quesenberry CP Jr. Hormone replacement therapy and the risk of myocardial infarction in women with coronary risk factors. Epidemiology 2000;11:603–6. Grodstein F, Manson JE, Colditz GA, et al. A prospective, observational study of postmenopausal hormone therapy and primary prevention of cardiovascular disease. Ann Intern Med 2000;133:933–41. Ferrara A, Quesenberry CP, Karter AJ, et al. Current use of unopposed estrogen and estrogen plus progestin and the risk of acute myocardial infarction among women with diabetes: the Northern California Kaiser Permanente Diabetes Registry, 1995–1998. Circulation 2003;107:43–8. Herrington DM. Hormone replacement therapy and heart disease: replacing dogma with data. Circulation 2003;107:2–4. > Hazard ratio. (95% CI) Data from WHI")
123
Coronary events with ET or placebo by age at baseline
50–59 60–69 70–79 Coronary event CHD (MI or coronary death) p = 0.07 CABG or PCI p = 0.09 MI, coronary death, CABG, and PCI p = 0.09 MI, coronary death, CABG, PCI, and confirmed angina p = 0.11 Hazard ratio (95% CI) Adapted from Hsia J, et al. Arch Intern Med 2006;166:357–65 123
 p = CABG or PCI. p = MI, coronary death, CABG, and PCI. p = MI, coronary death, CABG, PCI, and confirmed angina. p = Hazard ratio (95% CI) Adapted from Hsia J, et al. Arch Intern Med 2006;166:357–")
124
HT and risk of cardiovascular disease by years since menopause
Hazard ratio CI Absolute excess risk (per 10,000 person-years) < 10 0.76 0.50–1.16 -6 10–19 1.10 0.84–1.45 4 > 20 1.28 1.03–1.58 17 For women with less than 10 years since menopause began, the hazard ratio (HR) for CHD was 0.76 (95% confidence interval [CI], ); 10 to 19 years, 1.10 (95% CI, ); and 20 or more years, 1.28 (95% CI, ) (P for trend=.02). The estimated for CHD for women within 10 years of menopause was −6 per person-years; forwomen10 to 19 years since menopause began, 4 per person-years; and for women 20 or more years from menopause onset, 17 per person-years. p for trend = 0.02 Adapted from Rossouw JE, et al. JAMA 2007;297:1465–77 124
 < – – – > – For women with less than 10 years since menopause began, the hazard ratio (HR) for CHD was 0.76 (95% confidence interval [CI], ); 10 to 19 years, 1.10 (95% CI, ); and 20 or more years, 1.28 (95% CI, ) (P for trend=.02). The. estimated for CHD for women within 10 years of menopause was −6. per person-years; forwomen10 to 19 years since menopause began, 4 per person-years; and for women 20 or more years from menopause onset, 17 per person-years. p for trend = Adapted from Rossouw JE, et al. JAMA 2007;297:1465–")
125
WHI CEE/MPA study: incidence of diabetes
Placebo Hazard ratio = 0.79 95% CI = 0.67–0.93 Incidence CEE/MPA CEE/MPA (n) Placebo (n) 8014 7627 7894 7618 7785 7403 7675 7271 7461 7049 5418 5049 2842 2528 1252 922 Margolis and colleagues examined the effect of CEE+MPA use on diabetes incidence and insulin resistance in 15,641 postmenopausal women enrolled in the WHI E+P Study. All women were aged 50 to 79 years at the time of study enrollment and all had an intact uterus. Diabetes incidence was determined based on self-report of treatment with insulin or oral hypoglycemic medication. Cumulative incidence of treated diabetes was 3.5% in the CEE+MPA group and 4.2% in the placebo group (HR, 0.79; 95% CI, 0.67–0.93; P = .004). This represents an absolute reduction of 15 cases of incident-treated diabetes per 10,000 women per year of treatment. The HR was unchanged after adjusting for changes in BMI and waist circumference. Time (years) Adapted from Margolis KL, et al. Diabetologia 2004;47:1175–87 Margolis KL, et al. Diabetologia. 2004;47: 125
 Placebo (n) Margolis and colleagues examined the effect of CEE+MPA use on diabetes incidence and insulin resistance in 15,641 postmenopausal women enrolled in the WHI E+P Study. All women were aged 50 to 79 years at the time of study enrollment and all had an intact uterus. Diabetes incidence was determined based on self-report of treatment with insulin or oral hypoglycemic medication. Cumulative incidence of treated diabetes was 3.5% in the CEE+MPA group and 4.2% in the placebo group (HR, 0.79; 95% CI, 0.67–0.93; P = .004). This represents an absolute reduction of 15 cases of incident-treated diabetes per 10,000 women per year of treatment. The HR was unchanged after adjusting for changes in BMI and waist circumference. Time (years) Adapted from Margolis KL, et al. Diabetologia 2004;47:1175–87. Margolis KL, et al. Diabetologia. 2004;47:")
126
Annual risks and benefits after 7 years of estrogen-only HT
Stroke 12 n = 10,739 VTE* 7 * = NS Increase Per 10,000 woman-years 5 CVD* 7 Breast cancer* Decrease 6 Hip fractures 6 Vertebral fractures . . , 57 All fractures Adapted from JAMA 2004;291:1701–12 MacLennan A, Sturdee D. Climacteric 2004 126

127
WHI E-only clinical outcomes when initiated age 50–59 Annual change in risk (all NS)
Increase Stroke 0.1 VTE 1 Per 10,000 woman-years Decrease 1 Breast cancer 3 CVD 3 Total deaths 2 Colorectal cancer 7 Global Index Adapted from JAMA 2004;291:1701–12 MacLennan A, Sturdee D. Climacteric 2004 127

128
Age-specific incidence of venous thrombosis WHI study; RCT 16,608 women
Age (years) 50–59 60–69 70–79 Placebo E + P Placebo E + P Placebo E + P Number of cases Annualized rate/ person-years Hazard ratio 95% CI 1.2– – – – –14.4 Cushman M, et al. JAMA 2004;292:1573–80 128
 50–59 60–69 70–79. Placebo E + P Placebo E + P Placebo E + P. Number of cases Annualized rate/ person-years. Hazard ratio % CI 1.2– – – – –14.4. Cushman M, et al. JAMA 2004;292:1573–")
129
Venous thrombosis and body mass index WHI study; RCT 16,608 women age 50–79 years
< –30 > 30 Placebo E + P Placebo E + P Placebo E + P Number of cases Annualized rate/ person-years Hazard ratio 95% CI 0.9– – – – –10.1 Cushman M, et al. JAMA 2004;292:1573–80 129

130
VTE: route of administration and progestogens ESTHER study
Route/progestogen Odds ratio 95% CI Oral 4.2 1.5–11.6 Transdermal 0.9 0.4–2.1 Micronized progesterone 0.7 0.3–1.9 Pregnanes 0.4–2.3 Norpregnanes 3.9 1.5–10.0 Canonico M, et al. Circulation 2007;115:820–2 130

131
Relation of years since menopause to progression of atherosclerosis
Adventitia Plaque Fibrous cap MMP-9 Necrotic core Fibrous cap Plaque Plaque Fibrous cap Necrotic core Media Internal elastic lamina Fatty streak/plaque 5 to < 10 19% 10 to < 15 21% ≥ 15 43% < 5 17% Years postmenopause % of WHI enrollees Given that the time of initiation of HT may influence its beneficial or adverse effects on the progression of atherosclerotic lesions, the number of years after menopause that women initiate HT may be very important in determining the outcome of therapy. In this slide, the box shows the percentage of enrollees in WHI within a particular range of years postmenopause; for example, the majority (64%) of the women randomized in WHI were more than 10 years postmenopause. In addition, more than 35% of the women randomized to E+P had hypertension, 50% had a history of smoking, and the majority were obese, all of which are risk factors for CHD. Thus, the majority of women in WHI likely had subclinical or undiagnosed atherosclerosis, which might have limited the efficacy of E+P. 131
 of the women randomized in WHI were more than 10 years postmenopause. In addition, more than 35% of the women randomized to E+P had hypertension, 50% had a history of smoking, and the majority were obese, all of which are risk factors for CHD. Thus, the majority of women in WHI likely had subclinical or undiagnosed atherosclerosis, which might have limited the efficacy of E+P")
132
Postmenopausal hormone use and coronary heart disease, NHS 1976–2000 Timing of hormone initiation with respect to age Excluding postmenopausal women with prevalent CHD RR (95% CI) 50–59 years 60 + years Adjusted for age, body mass index, hypercholesterolemia, hypertension, parental coronary heart disease, diabetes, cigarette smoking, dietary data, husband’s education, alcohol intake, physical activity, vitamin E or multivitamin supplementation, aspirin use Adapted from Grodstein F, et al. J Womens Health 2006;15:35–44 132
 50–59 years years Adjusted for age, body mass index, hypercholesterolemia, hypertension, parental coronary heart disease, diabetes, cigarette smoking, dietary data, husband’s education, alcohol intake, physical activity, vitamin E or multivitamin supplementation, aspirin use. Adapted from Grodstein F, et al. J Womens Health 2006;15:35–")
133
Coronary heart disease events associated with hormone therapy in younger and older women: a meta-analysis 23 trials, with 39,049 participants followed for 191,340 patient-years Odds ratio for total mortality < 60 years* 0.68 (CI, 0.48–0.96) > 60 years 1.03 (CI, 0.91–1.16) * Statistical significance Adapted from Salpeter SR, et al. J Gen Intern Med 2006;21:363–6 133
 > 60 years (CI, 0.91–1.16) * Statistical significance. Adapted from Salpeter SR, et al. J Gen Intern Med 2006;21:363–")
134
Summary of published results on incidence of endometrial cancer in relation to use of hormone therapy (HT) Type of HT Relative risk (95% CI) Unopposed estrogen < 1 year 1.4 (1.0–1.8) 1–4 years 2.8 (2.3–3.5) 5–9 years 5.9 (4.7–7.5) 10+ years 9.5 (7.4–12.3) Sequential E + P; ever vs. never 1.3 (1.1–1.4) CCEPT from WHI 0.8 (0.5–1.4) CCEPT, continuous combined estrogen and progestogen; E, estrogen; P, progestogen Adapted from Grady D, et al. Obstet Gynecol 1995;85:304–13 Beral V, et al. J Epidemiol Biostat 1999;4:191–215 Anderson GL, et al. JAMA 2003;290:1739–44 134
 Unopposed estrogen < 1 year 1.4 (1.0–1.8) 1–4 years 2.8 (2.3–3.5) 5–9 years 5.9 (4.7–7.5) 10+ years 9.5 (7.4–12.3) Sequential E + P; ever vs. never 1.3 (1.1–1.4) CCEPT from WHI 0.8 (0.5–1.4) CCEPT, continuous combined estrogen and progestogen; E, estrogen; P, progestogen. Adapted from Grady D, et al. Obstet Gynecol 1995;85:304–13 Beral V, et al. J Epidemiol Biostat 1999;4:191–215 Anderson GL, et al. JAMA 2003;290:1739–")
135
Endometrial hyperplasia rates after 1 and 2 years of low-dose estrogen + progestogen
Women’s HOPE Study Year 1 Year 2 Hyperplasia rate (%) 0.00 0.00 0.00 0.00 0.00 0.00 0.625 mg 0.45 mg 0.3 mg 0.625/ 2.5 mg 0.45/ 2.5 mg 0.45/ 1.5 mg 0.3/ 1.5 mg Placebo As part of the Women’s Health, Osteoporosis, Progestin, Estrogen (Women’s HOPE) Study, the endometrial safety of 2 years of treatment with lower doses of continuous-combined CEE and MPA was evaluated in 822 healthy postmenopausal women with intact uteri (mean age, 52 years) who were enrolled in this randomized, double-blind, placebo-controlled, multicenter study. Patients were randomly assigned to one of eight treatments: CEE 0.625, CEE 0.625/MPA 2.5, CEE 0.45, CEE 0.45/MPA 2.5, CEE 0.45/MPA 1.5, CEE 0.3, CEE 0.3/MPA 1.5 (all doses mg/day), or placebo for 2 years. Endometrial biopsies were evaluated at baseline and years 0.5, 1, 1.5, and 2 using a centralized protocol. As shown in the bar chart, no cases of endometrial hyperplasia were seen in the four CEE/MPA groups. For the CEE-alone groups, a dose-related increase in incidence from 3.17% (CEE 0.3 mg) to 27.27% (CEE mg) was seen at 2 years. The number of cases increased from Year 1 to Year 2, even in the low-dose CEE 0.3 group. Thus, 2 years of treatment with lower doses of CEE/MPA provided endometrial protection comparable to that seen with commonly prescribed doses. These results are especially relevant with recent guidance from the FDA to use the lowest effective dose of HT for the shortest duration needed to achieve treatment goals. CEE CEE/MPA CEE, conjugated equine estrogens; MPA, medroxyprogesterone acetate Adapted from Pickar JH, et al. Fertil Steril 2003;80:1234–40 135 Pickar JH, et al. Fertil Steril. 2003;80:
 mg mg. 0.3 mg / 2.5 mg. 0.45/ 2.5 mg. 0.45/ 1.5 mg. 0.3/ 1.5 mg. Placebo. As part of the Women’s Health, Osteoporosis, Progestin, Estrogen (Women’s HOPE) Study, the endometrial safety of 2 years of treatment with lower doses of continuous-combined CEE and MPA was evaluated in 822 healthy postmenopausal women with intact uteri (mean age, 52 years) who were enrolled in this randomized, double-blind, placebo-controlled, multicenter study. Patients were randomly assigned to one of eight treatments: CEE 0.625, CEE 0.625/MPA 2.5, CEE 0.45, CEE 0.45/MPA 2.5, CEE 0.45/MPA 1.5, CEE 0.3, CEE 0.3/MPA 1.5 (all doses mg/day), or placebo for 2 years. Endometrial biopsies were evaluated at baseline and years 0.5, 1, 1.5, and 2 using a centralized protocol. As shown in the bar chart, no cases of endometrial hyperplasia were seen in the four CEE/MPA groups. For the CEE-alone groups, a dose-related increase in incidence from 3.17% (CEE 0.3 mg) to 27.27% (CEE mg) was seen at 2 years. The number of cases increased from Year 1 to Year 2, even in the low-dose CEE 0.3 group. Thus, 2 years of treatment with lower doses of CEE/MPA provided endometrial protection comparable to that seen with commonly prescribed doses. These results are especially relevant with recent guidance from the FDA to use the lowest effective dose of HT for the shortest duration needed to achieve treatment goals. CEE. CEE/MPA. CEE, conjugated equine estrogens; MPA, medroxyprogesterone acetate. Adapted from Pickar JH, et al. Fertil Steril 2003;80:1234– Pickar JH, et al. Fertil Steril. 2003;80:")
136
Effect of CEE, CEE/MPA on vaginal maturation* Women's HOPE Study
† % Superficial cells (median) † † ‡ ‡ Treatment groups 0.625 mg 0.625/ 2.5 mg 0.45 mg 0.45/ 2.5 mg 0.45/ 1.5 mg 0.3 mg 0.3/ 1.5 mg Placebo CEE CEE/MPA This study evaluated the efficacy of both CEE and CEE plus MPA in relieving symptoms of vaginal atrophy in 2,673 women enrolled in the Women’s HOPE study.1 Vaginal atrophy was assessed by vaginal maturation index (VMI), which was reported as the proportion of vaginal superficial cells, relative to the number of parabasal and intermediate cells, in a lateral vaginal wall smear. The percentage of superficial cells was increased significantly from baseline at cycles 6 and 13 in all CEE and CEE/MPA groups (P < .001), but not in placebo. Changes from baseline were significantly greater in the CEE group compared with the CEE 0.625/MPA 2.5 group (P < .05), the CEE 0.45 group (P < .05), and the CEE 0.3 group (P < .001). No differences in median changes in VMI were detected between the CEE 0.45 and the CEE 0.45/MPA 1.5 groups or between the CEE 0.3 and CEE 0.3/MPA 1.5 groups. The values for the median change from baseline in VMI were similar in the CEE 0.625/MPA 2.5 and CEE 0.45/MPA 1.5 groups. In summary, lower doses of CEE alone and CEE/MPA were effective in improving the VMI in postmenopausal women. There was no change in VMI in the placebo group. CEE, conjugated equine estrogens; MPA, medroxyprogesterone acetate *p < 0.05 vs. baseline and placebo for all active treatment groups; †p < 0.05 vs. CEE 0.625; ‡p < 0.05 vs. CEE 0.3/MPA 1.5 Adapted from Utian WH, et al. Fertil Steril 2001;75:1065–79 Utian WH, Shoupe D, Bachmann G, Pinkerton JV, Pickar JH. Relief of vasomotor symptoms and vaginal atrophy with lower doses of conjugated equine estrogens and medroxyprogesterone acetate. Fertil Steril. 2001;75: 136
 † † ‡ ‡ Treatment groups mg / 2.5 mg mg. 0.45/ 2.5 mg. 0.45/ 1.5 mg. 0.3 mg. 0.3/ 1.5 mg. Placebo. CEE. CEE/MPA. This study evaluated the efficacy of both CEE and CEE plus MPA in relieving symptoms of vaginal atrophy in 2,673 women enrolled in the Women’s HOPE study.1. Vaginal atrophy was assessed by vaginal maturation index (VMI), which was reported as the proportion of vaginal superficial cells, relative to the number of parabasal and intermediate cells, in a lateral vaginal wall smear. The percentage of superficial cells was increased significantly from baseline at cycles 6 and 13 in all CEE and CEE/MPA groups (P < .001), but not in placebo. Changes from baseline were significantly greater in the CEE group compared with the CEE 0.625/MPA 2.5 group (P < .05), the CEE 0.45 group (P < .05), and the CEE 0.3 group (P < .001). No differences in median changes in VMI were detected between the CEE 0.45 and the CEE 0.45/MPA 1.5 groups or between the CEE 0.3 and CEE 0.3/MPA 1.5 groups. The values for the median change from baseline in VMI were similar in the CEE 0.625/MPA 2.5 and CEE 0.45/MPA 1.5 groups. In summary, lower doses of CEE alone and CEE/MPA were effective in improving the VMI in postmenopausal women. There was no change in VMI in the placebo group. CEE, conjugated equine estrogens; MPA, medroxyprogesterone acetate. *p < 0.05 vs. baseline and placebo for all active treatment groups; †p < 0.05 vs. CEE 0.625; ‡p < 0.05 vs. CEE 0.3/MPA 1.5. Adapted from Utian WH, et al. Fertil Steril 2001;75:1065–79. Utian WH, Shoupe D, Bachmann G, Pinkerton JV, Pickar JH. Relief of vasomotor symptoms and vaginal atrophy with lower doses of conjugated equine estrogens and medroxyprogesterone acetate. Fertil Steril. 2001;75:")
137
HT use and risk of colorectal cancer
Jacobs et al. 1994*† Newcomb and Storer 1995*† Folsom et al. 1995*† Troisi et al. 1997‡ Kampman et al. 1997† Grodstein et al. 1998† Paganini-Hill 1999‡ Hully et al. 2002† Chlebowski et al. 2004† Meta-analysis: Nanda et al. 1999*† Meta-analysis: Grodstein et al. 1999‡§ Several studies have indicated that HT use can reduce risk of colorectal cancer.1-11 The above figure represents risk estimates from 2 randomized controlled trials, 7 observational studies, and 2 meta-analyses. Risk assessments are age-adjusted or multivariate, as indicated. Also as indicated, some of these studies reported risk assessments for colon cancer only.1-3,10 Although the exact mechanism of E's protective effect is unclear, there are theories concerning this association. One theory suggests that secondary bile acids are carcinogenic, and hormone use decreases bile acids.12 Another theory involves activity of ERs in the colon. ER- is the predominant ER subtype in the human colon, and decreased levels of ER- are associated with colon tumors in women. Estrogen use increases ER-, and may thereby prevent new tumors.13 al-Azzawi and Wahab also reported that ER activity may suppress tumor growth by preventing a "methylation imbalance" that leads to tumor progression14: Aggregates of cytosine and guanosine, known as CpG islands, are found in the promoter regions of many genes. Normally, CpG islands are free of methylation. However, methylation of CpG islands "silences" the gene, leading to reduced expression or inactivation of genes downstream. Complete methylation of the ER CpG island occurs in colonic cancer tissue, resulting in deregulation of colon tumor cell growth. Estrogen therapy may prevent colon cancer by interfering with CpG methylation, thereby contributing to tumor suppression. Relative risk (95% CI) *Statistic refers to colon cancer risk only; †Multivariate risk analysis; ‡Risk assessment adjusted for age only; §Meta-analysis includes two studies of colorectal cancer mortality Council on Hormone Education 1Jacobs EJ, et al. Cancer Causes Control. 1994;5: 2Newcomb PA, Storer BE. J Natl Cancer Inst. 1995;87: 3Folsom AR, et al. Am J Public Health. 1995;85: 4Troisi R, et al. Cancer Causes Control. 1997;8:130-8. 5Kampman E, et al. Cancer Causes Control. 1997;8: 6Grodstein F, et al. Ann Intern Med. 1998;128: 7Paganini-Hill A. Dis Colon Rectum. 1999;42: 8Hulley S, et al. JAMA. 2002;288:58-66. 9Writing Group for the WHI Investigators. JAMA. 2002;288: 10Nanda K, et al. Obstet Gynecol. 1999;93:880-8. 11Grodstein F, et al. Am J Med. 1999;106: 12Kamano T, et al. Dis Colon Rectum. 1999;42: 13Campbell-Thompson M, et al. Cancer Res. 2001;61: 14al-Azzawi F, Wahab M. Climacteric. 2002;5:3-14. 137
 *Statistic refers to colon cancer risk only; †Multivariate risk analysis; ‡Risk assessment adjusted for age only; §Meta-analysis includes two studies of colorectal cancer mortality. Council on Hormone Education. 1Jacobs EJ, et al. Cancer Causes Control. 1994;5: Newcomb PA, Storer BE. J Natl Cancer Inst. 1995;87: Folsom AR, et al. Am J Public Health. 1995;85: Troisi R, et al. Cancer Causes Control. 1997;8: Kampman E, et al. Cancer Causes Control. 1997;8: Grodstein F, et al. Ann Intern Med. 1998;128: Paganini-Hill A. Dis Colon Rectum. 1999;42: Hulley S, et al. JAMA. 2002;288: Writing Group for the WHI Investigators. JAMA. 2002;288: Nanda K, et al. Obstet Gynecol. 1999;93: Grodstein F, et al. Am J Med. 1999;106: Kamano T, et al. Dis Colon Rectum. 1999;42: Campbell-Thompson M, et al. Cancer Res. 2001;61: al-Azzawi F, Wahab M. Climacteric. 2002;5:")
138
Randomized controlled trials: breast cancer results
HERS II WHI E+P E+P E Follow-up 6.8 years 6.2 years 7.1 years RR of BC (ITT) 95% CI 0.8– – –1.04 RR of BC (adherent) 95% CI – –0.97 Adapted from Hulley, JAMA 1998, Chlebowski, JAMA 2002, JAMA 2003, Stefanick, JAMA 2006 138
 % CI 0.8– – –1.04. RR of BC (adherent) % CI 1.13– –0.97. Adapted from Hulley, JAMA 1998, Chlebowski, JAMA 2002, JAMA 2003, Stefanick, JAMA")
139
Body mass index: the risk with hormone therapy is (more) apparent in lean women
BMI > 24.4 kg/m2 – no additional risk Schairer C, et al. JAMA 2000;283:485–91 BMI > 26 kg/m2 – no additional risk Rosenberg L, et al. Arch Intern Med 2006;166:760–5 Inverse relationship between the risk and BMI with estrogen or combined hormone therapy Million Women Study. Reeves GK, et al. Lancet Oncol 2006;7:910–18 80% of users have a BMI < 25 E3N-EPIC. Fournier A, et al. Int J Cancer 2005;114:448–54 139

140
Hormone therapy in women with breast cancer
Contradictory results between two randomized controlled trials HABITS: 434 patients, stopped after 2.1 years HR: 3.3 (1.5–7.4) Lancet 2004;363:453–5 Stockholm: 378 patients, stopped after 4.1 years HR: 0.82 (0.35–1.9) JNCI 2005;97:533–5 Heterogeneity between the two studies: Type of treatment Proportion of tamoxifen-treated women (52% vs. 21%) Node-positive patients 140
 Lancet 2004;363:453–5. Stockholm: 378 patients, stopped after 4.1 years. HR: 0.82 (0.35–1.9) JNCI 2005;97:533–5. Heterogeneity between the two studies: Type of treatment. Proportion of tamoxifen-treated women (52% vs. 21%) Node-positive patients")
141
Low-dosage micronized 17β-estradiol + calcium prevent bone loss in postmenopausal women
Effect of micronized 17β-estradiol + calcium on spinal bone mineral density Estradiol 2.0 mg * 3 Estradiol 1.0 mg * 2 Estradiol 0.5 mg * 1 Placebo Mean annual % change from baseline -1 Low-dosage micronized 17 beta-estradiol prevents bone loss in postmenopausal women. Ettinger B, Genant HK, Steiger P, Madvig P. Am J Obstet Gynecol 1992 Feb;166(2): Division of Research, Kaiser Permanente Medical Care Program, Oakland, CA With the use of a double-blind, randomized, dose-ranging design, we tested during an 18-month period the degree of protection against postmenopausal bone loss afforded by micronized 17 beta-estradiol in dosages of 0.5, 1.0, and 2.0 mg. All subjects received supplementation to ensure a minimum of 1500 mg calcium daily. Fifty-one subjects completed at least 1 year of follow-up bone density measurements by quantitative computed tomography and by single- and dual-photon absorptiometry. In the placebo group spinal trabecular bone density decreased 4.9% annually (p less than 0.001), whereas in those taking micronized 17 beta-estradiol bone density tended to increase (annual increases of 0.3% in the 0.5 mg micronized 17 beta-estradiol group, 1.8% in the 1.0 mg micronized 17 beta-estradiol group, and 2.5% in the 2.0 mg micronized 17 beta-estradiol group). After completing the double-blind phase, 41 subjects completed an additional 18 months of follow-up while taking 1.0 mg micronized 17 beta-estradiol. During this time one third of the subjects were randomly assigned to discontinue calcium supplements. Among those who previously received placebo, trabecular bone density increased 4.3% annually, whereas among those who had used micronized 17 beta-estradiol, trabecular bone density response was inversely related to the dosage previously used. Additionally and independently, the level of calcium intake showed a statistically significant correlation with the change in spinal trabecular bone density (r = 0.37, p = 0.02). We conclude that micronized 17 beta-estradiol has a continuous skeletal dose-response effect in the range of 0.5 to 2.0 mg and that calcium intake positively modifies the skeletal response to 1.0 mg micronized 17 beta-estradiol. -2 -3 -4 -5 *p < vs. placebo Adapted from Ettinger B, et al. Am J Obstet Gynecol 1992;166:479–88 141
: Division of Research, Kaiser Permanente Medical Care Program, Oakland, CA With the use of a double-blind, randomized, dose-ranging design, we tested during an 18-month period the degree of protection against postmenopausal bone loss afforded by micronized 17 beta-estradiol in dosages of 0.5, 1.0, and 2.0 mg. All subjects received supplementation to ensure a minimum of 1500 mg calcium daily. Fifty-one subjects completed at least 1 year of follow-up bone density measurements by quantitative computed tomography and by single- and dual-photon absorptiometry. In the placebo group spinal trabecular bone density decreased 4.9% annually (p less than 0.001), whereas in those taking micronized 17 beta-estradiol bone density tended to increase (annual increases of 0.3% in the 0.5 mg micronized 17 beta-estradiol group, 1.8% in the 1.0 mg micronized 17 beta-estradiol group, and 2.5% in the 2.0 mg micronized 17 beta-estradiol group). After completing the double-blind phase, 41 subjects completed an additional 18 months of follow-up while taking 1.0 mg micronized 17 beta-estradiol. During this time one third of the subjects were randomly assigned to discontinue calcium supplements. Among those who previously received placebo, trabecular bone density increased 4.3% annually, whereas among those who had used micronized 17 beta-estradiol, trabecular bone density response was inversely related to the dosage previously used. Additionally and independently, the level of calcium intake showed a statistically significant correlation with the change in spinal trabecular bone density (r = 0.37, p = 0.02). We conclude that micronized 17 beta-estradiol has a continuous skeletal dose-response effect in the range of 0.5 to 2.0 mg and that calcium intake positively modifies the skeletal response to 1.0 mg micronized 17 beta-estradiol *p < vs. placebo. Adapted from Ettinger B, et al. Am J Obstet Gynecol 1992;166:479–")
142
Osteoporosis and bone strength
Genetics Architecture Diet Turnover rate Exercise Damage accumulation Hormones Degree of mineralization Bone density + Bone quality Bone strength Adapted from The NIH Consensus Development Panel on Osteoporosis. JAMA 2001;285:785–95 142

143
Different effects of estrogen therapy on connective tissue
Genital organs (improved) Cerebral changes (Alzheimer’s decreased) Estrogen therapy Decreased skin thickness (reversed) CVS effects (including carotids) Bone loss (stopped and reversed) Cartilage 143
 Cerebral changes. (Alzheimer’s decreased) Estrogen. therapy. Decreased. skin thickness. (reversed) CVS effects. (including carotids) Bone loss. (stopped and reversed) Cartilage")
144
Cartilage, an estrogen-responsive tissue
300 300 *** 200 200 *** CTX-II (ng/mmol) CTX-II (ng/mmol) 100 100 Pre- menopause Post- menopause No HRT HRT *p < 0.001 Adapted from Mouritzen, et al. Ann Rheum Dis 2003;62:332–6 144
 CTX-II (ng/mmol) Pre- menopause. Post- menopause. No HRT. HRT. *p < Adapted from Mouritzen, et al. Ann Rheum Dis 2003;62:332–")
145
Selective serotonin and/or noradrenaline reuptake inhibitors
Newer SNRI formulations: Extended release venlafaxine 51% reduction in hot flushes/sweats Less nausea Desvenlafaxine succinate – in development Selective NA & 5HT reuptake inhibitor Good plasma / brain ratios in animal models Evans ML, et al. Obstet Gynecol 2005;105:161–6 Deecher DC, et al. J Pharmacol Exp Ther 2006;318:657–65 145

146
Lower estrogen levels are associated with increased prevalence of sexual problems
Estrogen has many roles within the human body, including maintenance of vaginal health. Estrogen deficiency, as a result of natural or surgical menopause, is often associated with altered sexual function.1 Sarrel2 correlated the presence of sexual problems with levels of estradiol. When levels of estradiol were below 50 pg/mL, women reported greater levels of vaginal dryness, dyspareunia, pain from intercourse, and burning. When estradiol levels were brought to above 50 pg/mL, these symptoms abated.2 n = 93; significance not reported Adapted from Sarrel PM. J Womens Health Gend Based Med 2000;9:S25–32 Sarrel PM. Obstet Gynecol 1990;75:S26–30 1Sarrel PM. Effects of hormone replacement therapy on sexual psychophysiology and behavior in postmenopause. J Womens Health Gend Based Med. 2000;9:S25-S32. 2Sarrel PM. Sexuality and menopause. Obstet Gynecol. 1990;75:26S-30S. 146

147
Postmenopausal hormone therapy and Alzheimer's disease risk: interaction with age
MIRAGE study: 426 cases, 545 family controls Significant interaction between age and HT use on AD risk (p = 0.03). Protective association was seen only in the youngest age tertile (50–63 years; odds ratio = 0.35, 95% CI= 0.19–0.66) HT may protect younger women from AD or reduce the risk of early-onset forms of AD, or HT used during the early postmenopause may reduce AD risk 1.00 0.50 Relative risk 0.10 Never 50–63 years 64–71 years 72–99 years HT use Adapted from Henderson VW, et al.; MIRAGE Study Group. J Neurol Neurosurg Psychiatry 2005;76:103–5 147
. Protective association was seen only in the youngest age tertile (50–63 years; odds ratio = 0.35, 95% CI= 0.19–0.66) HT may protect younger women from AD or reduce the risk of early-onset forms of AD, or HT used during the early postmenopause may reduce AD risk Relative risk Never. 50–63. years. 64–71. years. 72–99. years. HT use. Adapted from Henderson VW, et al.; MIRAGE Study Group. J Neurol Neurosurg Psychiatry 2005;76:103–")
148
Effect of hormone therapy Incidence of Alzheimer’s disease The Cache County Memory Study
0.12 0.10 0.08 0.06 0.04 0.02 Women HRT non-users HRT use < 3 years HRT use 3–10 years HRT use > 10 years Men Discrete annual hazard Age (years) Adapted from Zandi PP, et al. JAMA 2002;288:2123–9 148
 Adapted from Zandi PP, et al. JAMA 2002;288:2123–")
149
Exercise in the menopause
Any physical activity is better than being sedentary Regular exercise reduces total and cardiovascular mortality Better metabolic profile, balance, muscle strength, cognition and quality of life are observed in physically active persons. Heart events, stroke, fractures and breast cancer are significantly less frequent Benefits far outweigh possible adverse consequences: the more – the better, but too much may cause harm Summarizing the topic of exercise in the menopause, here are my conclusions: 149

150
Exercise in the menopause: optimal exercise prescription
At least 30 minutes of moderate intensity exercise, at least three times weekly Two additional weekly training sessions of resistance exercise may provide further benefit Injury to the musculo-articulo-skeletal system should be avoided What is the optimal exercise prescription? Thank you for your kind attention 150

151
AHA 2006 Diet and Lifestyle Recommendations 1
Balance calorie intake and physical activity to achieve or maintain a healthy body weight Consume a diet rich in vegetables and fruits Choose whole-grain, high-fiber foods Consume fish, especially oily fish, at least twice a week Circulation 2006;114:82 151

152
AHA 2006 Diet and Lifestyle Recommendations 2
Limit intake of saturated fat to < 7% of energy, trans fat to < 1% and cholesterol to < 300 mg/day by choosing lean meats and vegetable alternatives, selecting fat-free, 1% fat and low-fat products Choose and prepare foods with little or no salt Increase fiber intake (beans, whole grain, other fruits and vegetables) If you consume alcohol, do so in moderation Quit smoking Circulation 2006;114:82 152
 If you consume alcohol, do so in moderation. Quit smoking. Circulation 2006;114:")
Ähnliche Präsentationen