Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Fuzzy Sets und Medizin Graphik : Josef Partykiewicz ,Deutsches Ärzteblatt

2
Zeitlicher Verlauf und Organisationsplan der klinischen Untersuchung
Classen/Diehl/Kochsiek: Innere Medizin, München, Wien, Baltimore: Urban & Schwarzenberg, 41998, S. 433.

3
Medizinische Diagnose
Erkrankungen Symptome Symptome Labortestergebnisse Allgemeiner Zustand Röntgenuntersuchungs-ergebnisse Körperlicher Zustand Anamneseinformationen Ultraschalluntersuchungsergebnisse

4
Ludwik Fleck ( ) Über einige besondere Merkmale des ärztlichen Denkens (1927) „Das ärztliche Wissen, dessen Bereich so ausgedehnt wie seine Geschichte alt ist, hat zum Entstehen eines besonderen Stils geführt, die eigenen Probleme zu erfassen, einer besonderen Art, sich zu den ärztlichen Phänomenen zu verhalten, d. h. zu einem besonderen Denktyp.“ „Während der Naturwissenschaftler typische, normale Phänomene sucht, studiert der Arzt gerade die nicht typischen, nicht normalen, krankhaften Phänomene. Und dabei trifft er auf diesem Weg sofort auf einen gewaltigen Reichtum und Individualität dieser Phänomene, die die Vielheit ohne klare, abgegrenzte Einheiten begleiten, voller Übergangs- und Grenzzustände.“

5
Ludwik Fleck ( ) „Es gibt keine genaue Grenze zwischen dem, was gesund ist, und dem, was krank ist, und nirgends trifft man wirklich ein zweites Mal auf dasselbe Krankheitsbild. Aber diese unerhört reiche Vielheit immerfort anderer und anderer Varianten muss gedanklich bezwungen werden, denn dies ist die Erkenntnisaufgabe der Medizin.“ „Es entsteht ein riesiger Reichtum an Material. Die Aufgabe der Medizin ist, in diesem ursprünglichen Chaos irgendwelche Gesetze, Zusammenhänge, irgendwelche Typen höherer Ordnung zu finden.“

6
F. A. Nash (1954) What happens in the doctor‘s mind when he is faced with a patient? This will depend on his experience, on his book knowledge, and on his mental endowment ... 1) ... subconscious process of immediate recognition ... 2) ... Recall descriptions from books or from memories of practice of several diseases that might fit the patient‘s story ... 3) The doctor may take a main or significant symptom or sign, and using it as an intellectual straw to cling to, or start from, in a sea of memories and observations ... F. A. Nash: Differential Diagnosis. An Apparatus to Assist the Logical Faculties. The Lancet, 24. April 1954, S. 874f
 ... subconscious process of immediate recognition ... 2) ... Recall descriptions from books or from memories of practice of several diseases that might fit the patient‘s story ... 3) The doctor may take a main or significant symptom or sign, and using it as an intellectual straw to cling to, or start from, in a sea of memories and observations ... F. A. Nash: Differential Diagnosis. An Apparatus to Assist the Logical Faculties. The Lancet, 24. April 1954, S. 874f.")
8
Ledley und Lusted (1959) How do you make a medical diagnosis?
First, I obtain the case facts from the patient’s history, physical examination, and laboratory tests. Second, I evaluate the relative importance of the different signs and symptoms. Some of the data may be of first-order importance and other data of less importance. Third, to make a differential diagnosis I list all the diseases which the specific case can reasonable resemble. Then I exclude one disease after another from the list until it becomes apparent that the case can be fitted into a definite disease category, or that it may be one of several possible diseases, or else that its exact nature cannot be determined. R. S. Ledley, L. B. Lusted: Reasoning Foundations of Medical Diagnosis, Science, 1959, Volume 130, S

9
Ledley und Lusted (1959) Attribute eines Patienten, etwa das Anzeichen
„Fieber“ oder die Krankheit „Lungenentzündung“: Kleinbuchstaben x, y, ..., Aussagen über das Attribut: Großbuchstaben X, Y, .... Steht Y für die Aussage „Der Patient hat das Attribut y.“, so ist deren Negation die Aussage Y : „Der Patient hat nicht das Attribut y.“ „logisches UND“ (X·Y, XY) : „Der Patient hat die Attribute x und y.“, „logisches ODER“ (X+Y , XY ): „Der Patient hat Attribut x oder Attribut y oder beide.“ „Implikation“X Y: „Wenn der Patient das Attribut x hat, dann hat er Attribut y.“
 : „Der Patient hat die Attribute x und y. , „logisches ODER (X+Y , XY ): „Der Patient hat Attribut x oder. Attribut y oder beide. „Implikation X Y: „Wenn der Patient das Attribut x hat, dann hat er Attribut y.")
10
Ledley und Lusted (1959) Betrachtung von Aussagen über das Vorliegen von Symptomen und deren Wahrheitswerte z. B. „Symptom S1 liegt vor“, (wahr / falsch) „Symptom S2 liegt vor“, (wahr / falsch) „Symptom S3 liegt vor“, (wahr / falsch) Eine Krankheit wird dann als ein bestimmter Ausdruck von Aussagen über Symptome aufgefasst.
 „Symptom S2 liegt vor , (wahr / falsch) „Symptom S3 liegt vor , (wahr / falsch) Eine Krankheit wird dann als ein bestimmter Ausdruck von Aussagen über Symptome aufgefasst.")
11
Ledley und Lusted (1959) Examples If a patient has disease 2,
he must have symptom 1 D(2) S(1) If a patient has disease 1 and not disease 2, then he must have symptom 2 D(1)·D(2) S(2) then he cannot have symptom 2 D(1)·D(2) S(2) If a patient has either or both of the symptoms, then he must have one or both of the diseases S(1)+S(2) D(1)+D(2)
 S(1) If a patient has disease 1 and not disease 2, then he must have symptom 2 D(1)·D(2) S(2) then he cannot have symptom 2 D(1)·D(2) S(2) If a patient has either or both of the. symptoms, then he must have. one or both of the diseases S(1)+S(2) D(1)+D(2)")
12
The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.

13
Lipkin und Hardy (1958) The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.

14
Lipkin und Hardy (1958) The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.

15
Lipkin und Hardy (1958) The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.

16
Lipkin und Hardy (1958) The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.

17
Lipkin und Hardy (1958) The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.

18
Medizinische Diagnose mittels Aussagenlogik

19
Medizinisches Wissen aus einem Lehrbuch
The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions. Classen/Diehl/Kochsiek: Innere Medizin, München, Wien, Baltimore: Urban & Schwarzenberg, 41998, S. 433.

20
Medizinische Diagnose mittels Aussagenlogik
Beispiel: Symptom S1: Fieber, Gewichtsverlust, Nachtschweiß, Symptom S2: LDH-Anstieg (Laktatdehydrogenase) Symptom S3: Lymphknotenvergrößerung Für eine bestimmte Kombination dieser Symptome könnte das hochmaligne Non-Hodgkin-Lymphom (NHL) (in erster Näherung) vorliegen: Ohne Lymphknotenvergrößerung keine positive Diagnose, Entweder Symptom 1 oder Symptom 2 müssen hinzukommen. The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.
 Symptom S3: Lymphknotenvergrößerung. Für eine bestimmte Kombination dieser Symptome könnte das hochmaligne Non-Hodgkin-Lymphom (NHL) (in erster Näherung) vorliegen: Ohne Lymphknotenvergrößerung keine positive Diagnose, Entweder Symptom 1 oder Symptom 2 müssen hinzukommen. The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.")
21
Medizinische Diagnose mittels Aussagenlogik
Aussagen über das Vor-liegen von Symptomen Aussagen über das Vorliegen der Krankheit als logischer Ausdruck von Symptomen S1 S2 S3 (S1 ⋁ S2 ) ⋀ S3 S1 S3 S2
 ⋀ S3. S S3. S2.")
22
Vision über computerunterstützte Medizin (1965)
„The waiting room of the future will serve eight doctors; it will be completely sound proof. The furniture will consist of contour chairs with built-in gentle massage. Color television will delight the eye, and soft music will allay anxiety. Silent air conditions will waft delicately scented odors and soft drink dispensers, operating at the touch of a button, will deliver cool libation with or without a Miltown tablet. For those who prefer literature, magazine articles will be softly read by wire. History-taking will be painless. A group of preferential questions will be asked by tape and the answer punched on a card. Nothing will be left to chance, and by cybernetics, the card will be quickly deposited in a slot which will provide the three most probable historic diagnoses.“ Gerry Feigan M. D.: Triple Bromides, San Francisco Medical Society Bulletin, June 1965)
")
23
Vision über computerunterstützte Medizin (1965)
„Das Wartezimmer der Zukunft bedient acht Ärzte. Es ist völlig schalldicht. Das Mobiliar enthält anschmiegsame Stühle mit eingebauter sanfter Massage. Farbfernsehen erfreut das Auge und sanfte Musik beruhigt die Ängste. Leise Klimatisierung wird feine Düfte verbreiten und soft drinks, die auf Knopfdruck serviert werden, bieten kühle Erfrischungen Für jene, die Literatur vorziehen, werden Magazinartikel per Telegraphie ruhig vorgelesen. Die Anamnese ist schmerzlos. Ausgewählte Fragen werden vom Tonband gestellt, und die Antwort in eine Karte gestanzt. Nichts bleibt dem Zufall überlassen, und die Karte wird schnell mit Hilfe der Kybernetik in einem Schlitz deponiert, woraufhin die drei wahrscheinlichsten früheren Diagnosen ausgegeben werden.“ Gerry Feigan M. D.: Triple Bromides, San Francisco Medical Society Bulletin, June 1965)
")
26
Computer Assisted Diagnostic System 1970: CADIAG-I

28
„I‘ll be damned. It says ‛Cogito ergo sum.’ “ The New Yorker, 1958

29
Well, it‘s on its own now. We‘ve told it all we know.
(1958)
")
30
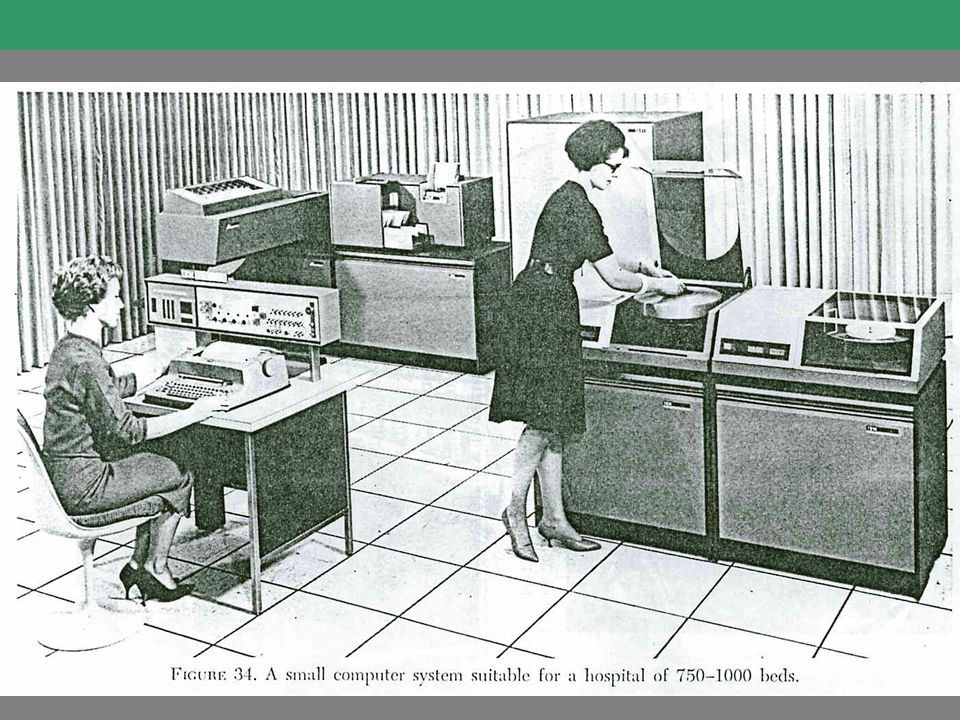
Das Wiener Computer Assisted Diagnostic System von 1968 - Hardware

31
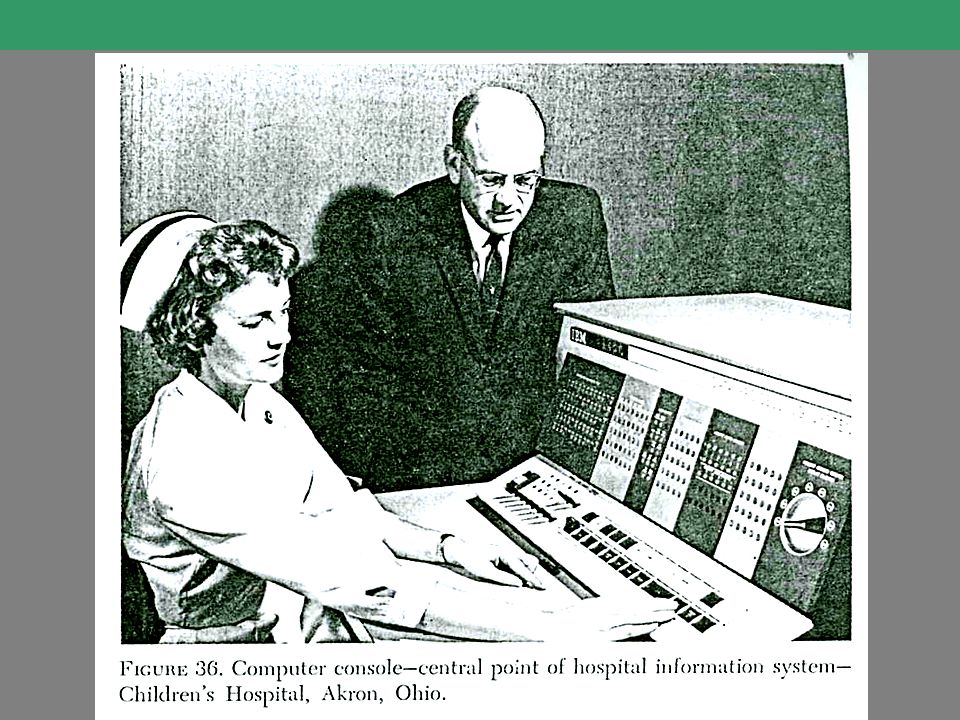
Das Wiener Computer Assisted Diagnostic System von 1968

32
Das Wiener Computer Assisted Diagnostic System von 1968

33
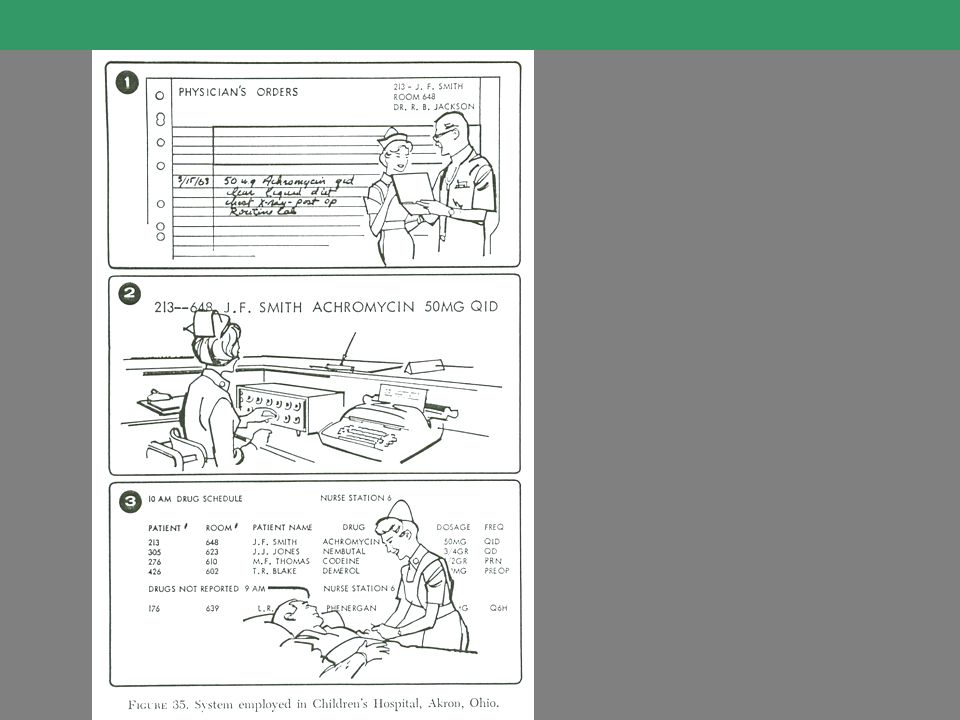
Das Wiener Computer Assisted Diagnostic System von 1968

34
Das Wiener Computer Assisted Diagnostic System von 1968

35
Das Wiener Computer Assisted Diagnostic System von 1968

36
Das Wiener Computer Assisted Diagnostic System von 1968

37
Das Wiener Computer Assisted Diagnostic System von 1968

38
..... MedframeCADIAG IV Adlassnig et al. 1996 ..... CADIAG II/RHEUMA -/COLON CADIAG II/GALL -/PANC CADIAG I Study CADIAG II Study CADIAG II Consult 1983 CADIAG I Consult CADIAG I Adlassnig et al. CADIAG II Adlassnig et al. 1980 1969 Gangl et al. 1968 Spindelberger & Grabner 1959 Ledley & Lusted

39
Das Wiener Computer Assisted Diagnostic System
Negation Konjunktion Disjunktion Außerdem: Symptom S ist obligat und beweisend für Krankheit K: S K Symptom S ist fakultativ und beweisend für Krankheit K S K Symptom S ist obligat und nicht beweisend für Krankheit K: S K Symptom S schließt Krankheit K aus: S K

40
Logische Grundlagen Mehrwertige Logik
Emil Leon Post ( ) The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions. Jan Łukasiewicz ( )
 The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions. Jan Łukasiewicz ( )")
41
Logische Grundlagen Mehrwertige Logik
„Eine Aussage, von welcher wir nicht wissen, ob sie wahr oder falsch ist, könnte überhaupt keinen Wert haben im Hinblick auf Wahrheit oder Falschheit, sondern einen dritten, unbestimmten Wert haben. Man könnte z. B. meinen, daß die Aussage `Ich werde in einem Jahr in Warschau sein´ weder wahr noch falsch ist und den dritten, unbestimmten Wert hat, den wir mit dem Symbol `1/2´ bezeichnen können. Man könnte aber auch noch weiter gehen und den Aussagen unendlich viele Werte zuschreiben, die zwischen der Falschheit und der Wahrheit liegen.“ The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions. Jan Łukasiewicz: Elemente der mathematischen Logik, Warschau 1929.

42
Mehrwertige Logik von Jan Łukasiewicz, 1921
1 ½ 1 ½ 1 ½ 1 ½ The need to restrain healthcare cost increases, implies a rearrangement of healthcare levels modifying the role of primary care, community care and home care. Many patients, who are presently treated in hospitals, could be adequately treated at a health centre closer to their home, by a team with whom they have had a long-standing personal relationship. Furthermore, many could even be treated at home. Many situations do not need to be dealt with by the highly specialised staff and technology available at hospitals. Population ageing is generating a dramatic increase in the number of chronic patients demanding healthcare assistance from healthcare models not designed to provide them with efficient solutions.

43
Computer Assisted Diagnostic System 1970: CADIAG-I

44
Computer Assisted Diagnostic System 1970: CADIAG-I

45
Computer Assisted Diagnostic System 1970: CADIAG-I

46
Computer Assisted Diagnostic System 1970: CADIAG-I

47
Fields, B. N. et al. (1996) Fields virology
Fields, B.N. et al. (1996) Fields virology. Lippincott-Raven Publishers, Philadelphia.
 Fields virology. Lippincott-Raven Publishers, Philadelphia.")
49
Symptome-Diagnosen-Relation
Erkrankungen S D Symptome Erkrankungen Symptome

50
Medizinische Diagnose
Erkrankungen Symptome Symptome Labortestergebnisse Allgemeiner Zustand Röntgenuntersuchungs-ergebnisse Körperlicher Zustand Anamneseinformationen Ultraschalluntersuchungsergebnisse

51
L. A. Zadeh, 1962: From Cercuit Theory to System Theory
In fact, there is a fairly wide gap between what might be regarded as „animate“ system theorists and „inanimate“ system theorists at the present time, and it is not at all certain that this gap will be narrowed, much less closed, in the near future. There are some who feel that this gap reflects the fundamental inadequacy of the conventional mathematics – the mathematics of precisely-defined points, functions, sets, probability measures, etc. - for coping with the analysis of biological systems, and that to deal effectively with such systems, which are generally orders of magnitude more complex than man-made systems, we need a radically different kind of mathematics, the mathematics of fuzzy or cloudy quantities which are not describable in terms of probability distributions. Indeed, the need for such mathematics is becoming increasingly apparent even in the realm of inanimate systems, for in most practical cases the a priori data as well as the criteria by which the performance of a man-made system is judged are far from being precisely specified or having accurately-known probability distributions.

52
Alonso Perez-Ojeda, 1976

53
Alonso Perez-Ojeda, 1976

55
Computer Assisted Diagnostic System II: CADIAG-II

56
Ludwik Fleck ( ) Über einige besondere Merkmale des ärztlichen Denkens (1927) „Das ärztliche Wissen, dessen Bereich so ausgedehnt wie seine Geschichte alt ist, hat zum Entstehen eines besonderen Stils geführt, die eigenen Probleme zu erfassen, einer besonderen Art, sich zu den ärztlichen Phänomenen zu verhalten, d. h. zu einem besonderen Denktyp.“ „Während der Naturwissenschaftler typische, normale Phänomene sucht, studiert der Arzt gerade die nicht typischen, nicht normalen, krankhaften Phänomene. Und dabei trifft er auf diesem Weg sofort auf einen gewaltigen Reichtum und Individualität dieser Phänomene, die die Vielheit ohne klare, abgegrenzte Einheiten begleiten, voller Übergangs- und Grenzzustände.“

57
Computer Assisted Diagnostic System II: CADIAG-II

58
Computer Assisted Diagnostic System II: CADIAG-II

59
Computer Assisted Diagnostic System II: CADIAG-II

60
Computer Assisted Diagnostic System II: CADIAG-II

61
Computer Assisted Diagnostic System II: CADIAG-II
Beispiele Example 1 (indicating): IF elevated amylase level in serum THEN acute pancreatitis WITH (O = very often [O = 0.90], B = strong [C = 0.70]). Example 2 (necessary and sufficient): IF rheumatoid arthritis and splenomegaly and leukopenia less than 4 giga/l THEN Felty’s Syndrom WITH (O = always [O = 1.00], C = confirming [C = 1.00]).
: IF elevated amylase level in serum. THEN acute pancreatitis. WITH (O = very often [O = 0.90], B = strong [C = 0.70]). Example 2 (necessary and sufficient): IF rheumatoid arthritis and. splenomegaly and. leukopenia less than 4 giga/l. THEN Felty’s Syndrom. WITH (O = always [O = 1.00], C = confirming [C = 1.00]).")
62
Computer Assisted Diagnostic System II: CADIAG-II Beispiele
Example 1: IF (ultrasonic of pancreas is pathological) THEN (pancreatic cancer) WITH (0.75 = often, 0.25 = weak) Example 2: IF (tophi) THEN (gout) WITH (0.25 = seldom, 1.00 = always) Example 3: IF (lower back pain limitation of motion of the lumbar spine diminished chest expansion male patient age between 20 and 40 years) THEN (ankylosing spondylitis) WITH (υ, 0.90 = very strong)
 THEN (pancreatic cancer) WITH (0.75 = often, 0.25 = weak) Example 2: IF (tophi) THEN (gout) WITH (0.25 = seldom, 1.00 = always) Example 3: IF (lower back pain limitation of motion of the lumbar spine diminished chest expansion male patient age between 20 and 40 years) THEN (ankylosing spondylitis) WITH (υ, 0.90 = very strong)")
63
Komposition von Relationen
Y q Es seien X, Y (gewöhnliche) Mengen. Eine Relation q von X in Y ist eine Teilmenge des Cartesischen Produktes X Y und eine Relation r von Y in Z ist eine Teilmenge des Cartesischen Produktes Y Z: t := q r ist eine Relation von X in Z, t := q r = {(x,z)| y : (x,y) q (y,z) r} X Y r Z Y X Z t
 Mengen. Eine Relation q von X in Y ist eine Teilmenge des Cartesischen Produktes X Y und. eine Relation r von Y in Z ist eine Teilmenge des Cartesischen Produktes Y Z: t := q r ist eine Relation von X in Z, t := q r = {(x,z)| y : (x,y) q (y,z) r} X. Y. r. Z. Y. X. Z. t.")
64
Komposition von Relationen
Seien X, Y (gewöhnliche) Mengen und sei X Y deren Cartesisches Produkt. L(X): die Menge aller Fuzzy sets in X. L(Y): die Menge aller Fuzzy sets in Y. L(XY): die Menge aller Fuzzy sets in X Y. Eine Relation der beiden Mengen X und Y ist Teilmenge von X Y. Eine Fuzzy Relation R von X und Y ist Fuzzy-Teilmenge von L(X Y). Seien drei Mengen X, Y, Z und zwei Fuzzy-Relationen gegeben : Q in L(X Y), R in L(Y Z). Wie lassen sich die Fuzzy-Relationen Q und R zu einer neuen Fuzzy-Relation T L(X Z) kombinieren?
 Mengen und sei X Y deren Cartesisches Produkt. L(X): die Menge aller Fuzzy sets in X. L(Y): die Menge aller Fuzzy sets in Y. L(XY): die Menge aller Fuzzy sets in X Y. Eine Relation der beiden Mengen X und Y ist Teilmenge von X Y. Eine Fuzzy Relation R von X und Y ist Fuzzy-Teilmenge von L(X Y). Seien drei Mengen X, Y, Z und zwei Fuzzy-Relationen gegeben : Q in L(X Y), R in L(Y Z). Wie lassen sich die Fuzzy-Relationen Q und R. zu einer neuen Fuzzy-Relation T L(X Z) kombinieren")
65
T(x,z) = maxxX min {Q(x,y); R(y,z)}, yY
Lotfi Zadeh, 1973: Komposition von Fuzzy-Relationen (“und”) min V (“oder”) max Q ist Fuzzy-Relation von X und Y, d. h. Q ist Fuzzy-Teilmengen von L(XY), R ist Fuzzy-Relation von Y und Z, d. h. R ist Fuzzy-Teilmenge von L(Y Z). T = Q R ist Fuzzy-Relation von X und Z, d.h.: T ist Fuzzy-Teilmenge von L(X Z) mit Zugehörigkeitsfunktion T(x,z) = maxxX min {Q(x,y); R(y,z)}, yY Outline of a New Approach to the Analysis of Complex Systems and Decision Processes
 min. V ( oder ) max. Q ist Fuzzy-Relation von X und Y, d. h. Q ist Fuzzy-Teilmengen von L(XY), R ist Fuzzy-Relation von Y und Z, d. h. R ist Fuzzy-Teilmenge von L(Y Z). T = Q R ist Fuzzy-Relation von X und Z, d.h.: T ist Fuzzy-Teilmenge von L(X Z) mit Zugehörigkeitsfunktion. T(x,z) = maxxX min {Q(x,y); R(y,z)}, yY. Outline of a New Approach to the Analysis. of Complex Systems and Decision Processes.")
66
Medizinisches Wissen Medical Knowledge is a network of relations of symptoms and diseases. Perez-Ojeda (1976) Medical knowledge is a network of fuzzy relations of symptoms and diseases. Elie Sanchez: (1979) S : Menge von Symptomen, D : Menge von Krankheiten, P : Menge von Patienten Q : Fuzzy-Relation von P und S, R : Fuzzy-Relation von S und D, T : Fuzzy-Relation von P und D. Max-min Komposition: T = Q R mit Zugehörigkeitsfunktion:
 Medical knowledge is a network of fuzzy relations of symptoms and diseases. Elie Sanchez: (1979) S : Menge von Symptomen, D : Menge von Krankheiten, P : Menge von Patienten. Q : Fuzzy-Relation von P und S, R : Fuzzy-Relation von S und D, T : Fuzzy-Relation von P und D. Max-min Komposition: T = Q R mit Zugehörigkeitsfunktion:")
67
Symptome-Diagnosen-Patienten-Fuzzy-Relation
Erkrankungen Symptome Patienten

68
Computer Assisted Diagnostic System II: CADIAG-II
Inferenz When Pk has Si with PS(Pk,Si) and when Si implies Dj with SDc(Si, Dj), then Pk has Dj with PD(Pk, Dj). When Pk has Si mit PS(Pk,Si), and when Si implies Sj with SSc(Si, Sj) and when Sj implies Di with SDc(Sj, Di) and when Di implies Dj with DDc(Di, Dj)
 and. when Si implies Dj with SDc(Si, Dj), then Pk has Dj with PD(Pk, Dj). When Pk has Si mit PS(Pk,Si), and. when Si implies Sj with SSc(Si, Sj) and. when Sj implies Di with SDc(Sj, Di) and. when Di implies Dj with DDc(Di, Dj)")
69
Computer Assisted Diagnostic System II: CADIAG-II
Ergebnisse Rheumatology more than 200 disease profiles, more than findings more than finding-disease-relationships more than 160 complex rules Hepatology and Gastroenterology more than 100 disease profiles, more than findings more than symptom-disease-relationships more than 40 complex rules

70
Computer Assisted Diagnostic System II: CADIAG-II
Evaluation

71
..... MedframeCADIAG IV Adlassnig et al. 1996 ..... CADIAG II/RHEUMA -/COLON CADIAG II/GALL -/PANC CADIAG I Study CADIAG II Study CADIAG II Consult 1983 CADIAG I Consult CADIAG I Adlassnig et al. CADIAG II Adlassnig et al. 1980 1969 Gangl et al. 1968 Spindelberger & Grabner 1959 Ledley & Lusted

72
Results With CADIAG-II/RHEUMA
Computer Assisted Diagnostic System II: CADIAG-II Results With CADIAG-II/RHEUMA Clinical diagnosis Cases Confirmed Hypothesis Confirmed or Hyp. Rheumatoid arthritis (100%) Gout (74%) Ankylosing spondylitis (100%) Psoriatic arthritis (80%) Sjögren’s disease (100%) SLE (100%) Reiter’s disease (0%) Scleroderma (40%) Total (93%)
 Gout (74%) Ankylosing spondylitis (100%) Psoriatic arthritis (80%) Sjögren’s disease (100%) SLE (100%) Reiter’s disease (0%) Scleroderma (40%) Total (93%)")
73
Computer Assisted Diagnostic System II: CADIAG-II
Clinical diagnosis Cases Confirmed Hypothesis Confirmed or Hyp. Pancreatic cancer (90%) Chronic pancreatitis (90%) Acute pancreatitis (80%) Pancreatic pseudocyst & chronic pancreatitis & 4 4 (100%) acute pancreatitis & 2 2 (100%) Zollinger-Ellison syndrome (100%) Insulinoma (100%) Total (91%)
 Chronic pancreatitis (90%) Acute pancreatitis (80%) Pancreatic pseudocyst & chronic pancreatitis & 4 4 (100%) acute pancreatitis & 2 2 (100%) Zollinger-Ellison syndrome (100%) Insulinoma (100%) Total (91%)")
Ähnliche Präsentationen






 Volkszählung in den USA>")







 András Bárdossy IWS Universität Stuttgart.>")





