Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Thomas Danne Kinderkrankenhaus auf der Bult, Hannover, Germany Diabetes Control: Goals and reality – European perspective

2
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Targets are important We don´t need age-dependent or individual targets No phases of diabetes have less risk for late complications It is feasible to reach target HbA1c < 7.5% for half of the children with diabetes with access to intensive insulin treatment Is HbA1c the right target ? Agenda

3
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Plasma blood glucose and A1C goals for type 1 diabetes by age group Values by ageBefore meals Bedtime/overnight A1C Rationale Toddlers and preschoolers (<6 years) 100–180110–200 7.5) High risk and vulnerability to hypoglycemia School age (6–12 years) 90–180100–180 <8% Risks of hypoglycemia and relatively low risk of complications prior to puberty Adolescents and young adults (13–19 years) 90–13090–150 <7.5%* Risk of hypoglycemia Developmental and psychological issues Key concepts in setting glycemic goals: Goals should be individualized and lower goals may be reasonable based on benefit–risk assessment Blood glucose goals should be higher than those listed above in children with frequent hypoglycemia or hypoglycemia unawareness Postprandial blood glucose values should be measured when there is a disparity between preprandial blood glucose values and A1C levels Silverstein J, Klingensmith G, Copeland K, Plotnick L, Kaufman F, Laffel L, Deeb L, Grey M, Anderson B, Holzmeister LA, Clark N; American Diabetes Association. Care of children and adolescents with type 1 diabetes: a statement of the American Diabetes Association. Diabetes Care. 2005 Jan;28(1):186-212.
:")
4
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus

5
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus

6
SWEDEN: A change in HbA1c reference affects metabolic control: Targets are important ! 222320192017181712171413N = 9.5 9.0 8.5 8.0 7.5 7.0 6.5 6.0 5.5 394244393741 3932373836272932 33 403637384240 3536413538444232364033 909192939495969798990001 Mono S HPLC DCA 2000 DCCT calibration DCA 2000 Swedish calibration 1.4% diff. 1.1% diff. Years p=n.sp=0.003p=0.01 HbA1c, % Hanas R. Psychological impact of changing the scale of reported HbA1c results affects metabolic control. Diabetes Care 2002;25:2110-1. p=n.sp=0.04p=n.s (significance vs. year before change) àData from 49 patients born 1971-1989
 àData from 49 patients born")
7
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Childrens Hospital, Leicester Royal Infirmary, United Kingdom Clinique Pédiatrique, Centre Hospitalier de Luxembourg, Luxembourg Department of Endocrinology & Diabetes, Royal Children's Hospital, Australia Barn- och ungdomskliniken, Universitetssjukhuset Södra Grev Rosengatan Sweden IJsselland ziekenhuis, The Netherlands Endocrinology and Diabetes Research Group, Hospital de Cruces, Spain Clinica Pediatrica, Ospedale Policlinico, Italy The Hospital for Sick Children, University of Toronto, Canada Diabetes-Zentrum, Kinderkrankenhaus auf der Bult, Germany Hôpital Universitaire des Enfants Reine Fabiola Diabetology Clinic, Belgium Department of Paediatrics Trinity College, National Childrens Hospital, Ireland Peijas Hospital, Finland Children's Hospital of Los Angeles, USA Pediatric Clinic, Medical Faculty Department of Endocrinology & Genetics, Republic of Macedonia Paediatric Dept. L, Glostrup University Hospital, Denmark Dept. of Pediatrics, Haukeland Hospital, Norway National Center of Childhood Diabetes, Schneider Children's Medical Center of Israel, Royal Hospital for Sick Children, Glasgow, Scotland University Childrens Hospital, Zurich, Switzerland Department of Paediatrics, Nihon University School of Medicine, Tokyo, Japan Centro di Diabetologia, University of Parma, Italy Department of Psychology, University of Wollongong, Australia NovoNordisk, Denmark Hvidore-Adolescent-Study 2008

8
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Hvidore-Adolescent-Study 2008 2,269 potential study patients visited outpatient department during recruitment phase 2062 (91%) adolescents filled out the questionnaire 2036 (90%) gave a sample for a central HbA1c determination age 14.4 ±2.3 years; 50.6% male; Diabetes duration 6.1± 3.5 years mean HbA1c = 8.2% ± 1.4 significant differences between centers (F = 12.3; p<0.001) Center average HbA1c ranged between 7.4 to 9.3% 152 diabetes-professionals answered the tam questionnaire (pediatric diabetologists (46%) and diabetes nurse educators (32%) of 21 centres 6 had no dietitian, 11 had no psychosocial team member, while 3 centers had a psychologist/psychiater and social worker a part of their team.
 adolescents filled out the questionnaire 2036 (90%) gave a sample for a central HbA1c determination age 14.4 ±2.3 years; 50.6% male; Diabetes duration 6.1± 3.5 years mean HbA1c = 8.2% ± 1.4 significant differences between centers (F = 12.3; p<0.001) Center average HbA1c ranged between 7.4 to 9.3% 152 diabetes-professionals answered the tam questionnaire (pediatric diabetologists (46%) and diabetes nurse educators (32%) of 21 centres 6 had no dietitian, 11 had no psychosocial team member, while 3 centers had a psychologist/psychiater and social worker a part of their team.")
9
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus 7 8 9 10 adjusted HbA1c (%)123456789101112131415161718192021 mean HbA1c of adolescents in center (adjusted for age, diabetes duration and gender): 8.2 ± 1.4% 8.2 ± 1.4 % Hvidore Group (2008) submitted 7,4 7,6 7,7 7,8 7,9 8,0 8,1 8,2 8,3 8,4 8,6 8,8 9,0 9,1 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 8355672227610 557796985 < 7.0 7.0 – 7.4% 7.5 – 7.9% 8.0 – 9.0 % no target 22512590 175 2253012550225225 2257090225175 125 Number of adolescents in treated in center 123456789101112131415161718192021Center number Number of team members answering target HbA1c of teammembers Team-Target and HbA1c
 mean HbA1c of adolescents in center (adjusted for age, diabetes duration and gender): 8.2 ± 1.4% 8.2 ± 1.4 % Hvidore Group (2008) submitted 7,4 7,6 7,7 7,8 7,9 8,0 8,1 8,2 8,3 8,4 8,6 8,8 9,0 9,1 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% < – 7.4% 7.5 – 7.9% 8.0 – 9.0 % no target Number of adolescents in treated in center Center number Number of team members answering target HbA1c of teammembers Team-Target and HbA1c")
10
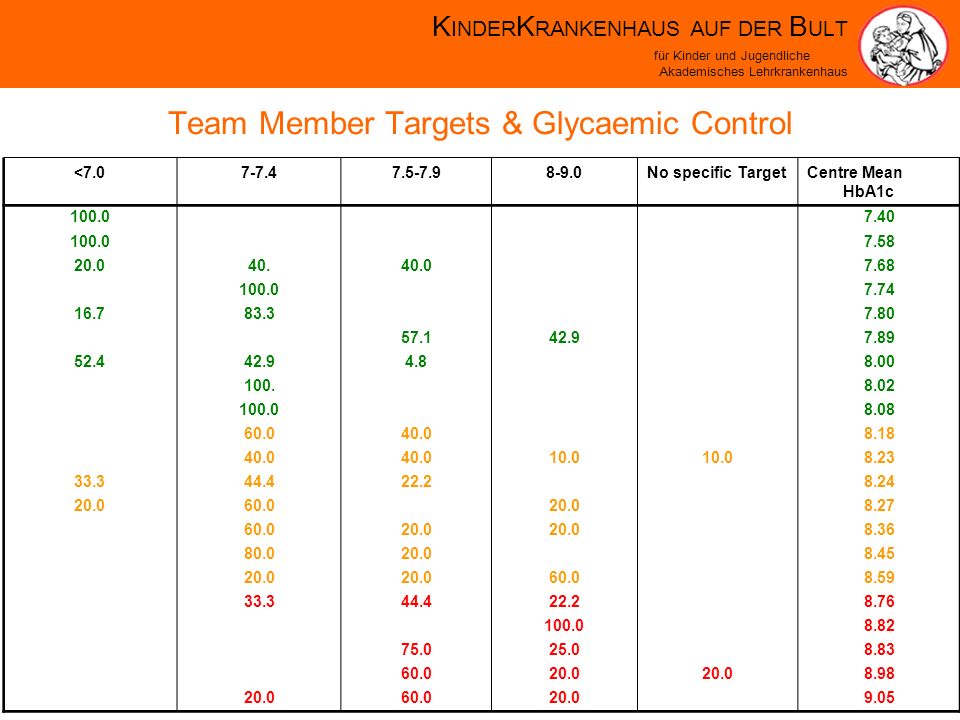
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Team Member Targets & Glycaemic Control <7.07-7.47.5-7.98-9.0No specific Target Centre Mean HbA1c 100.0 7.40 100.0 7.58 20.040.40.0 7.68 100.0 7.74 16.783.3 7.80 57.142.9 7.89 52.442.94.8 8.00 100. 8.02 100.0 8.08 60.040.0 8.18 40.0 10.0 8.23 33.344.422.2 8.24 20.060.0 20.0 8.27 60.020.0 8.36 80.020.0 8.45 20.0 60.0 8.59 33.344.422.2 8.76 100.0 8.82 75.025.0 8.83 60.020.0 8.98 20.060.020.0 9.05
11
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus 18 10.6 2.0 127 9.6 1.4 466 8.7 1.1 694 8.0 1.1 600 7.5 1.3 N mean SD parents happy 31 8.4 2.3 18 8.9 1.3 189 8.9 1.3 627 8.3 1.3 1056 7.9 1.3 N mean SD parents ideal 13 10.5 2.1 141 9.6 1.5 473 8.6 1.2 691 8.1 1.2 639 7.4 1.2 N meanl SD adolescent happy 47 8.1 1.6 25 8.9 1.0 205 8.8 1.3 713 8.4 1.3 975 7.9 1.4 N meanl SD adolescent ideal Don´t know 8.0 – 9.07.5-7.97.0-7.4<7.0target Relationship between targets of parents and adolescents and achieved HbA1c

12
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Betatp Step 1 Age.0693.077.002 Gender -.054-2.517.012 Diabetes Dration.1235.432.000 Insulin dose (Units/kg).1396.414.000 Insulin Regimen (BD Freemix).0502.247.025 Center rank.33715.251.000.0412.025.043 -.060-3.136.002.0663.236.001.0904.627.000.0472.362.018.1647.596.000 Betatp Adolescent Target happy with.29811.910.000 Parents Target happy with.24410.339.000 Adolescent Target Ideal -.060-2.757.006 Team Target - coherent -.096-2.728.006 Step 2 Multiple Regressionsanalysis proves the role of targets and team interaction for center differences
 Insulin Regimen (BD Freemix) Center rank Betatp Adolescent Target happy with Parents Target happy with Adolescent Target Ideal Team Target - coherent Step 2 Multiple Regressionsanalysis proves the role of targets and team interaction for center differences")
13
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Hvidore-Group 2008 A lower target HbA1c and a bigger consistency between team members within a center is associated with a lower average center HbA1c. Clear and consistent setting of targets is associated with the Outcome in adolescents with diabetes. Differences in treatment targets are an important factor contributing to center differences

14
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Influencing Microangiopathy Through Lowering The HbA1c In Randomised Studies DCCT Type of Diabetes1 Number of patients1441 Progress. Retinopathy 1,5 Kummamoto 110 2 UKPDS 3867 Progress. Nephropathy Progress. Neuropathy 5 (4-7) 4 (3-11) 10 (6-50) 7 (6-11) 5 (4-19) 5 (4-7) 5 (3-16) Follow-up (years)6,5610 HbA1c-change9,1->7,29,1->7,07,9->7,0 Parameter NNT Duration of study (95% CI)
 4 (3-11) 10 (6-50) 7 (6-11) 5 (4-19) 5 (4-7) 5 (3-16) Follow-up (years)6,5610 HbA1c-change9,1->7,29,1->7,07,9->7,0 Parameter NNT Duration of study (95% CI).")
15
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Rate of Background-Retinopathy (per 100 patient-years) < 77-88-99-1010-11> 11 0 2 4 6 8 10 Average HbA1c (%) Danne et. al, Diab Care 17: 1390-96, 1994 Berlin Retinopathy-Study (1977-94): Continuous Exponential Relationship between retinopathy and long-term-HbA1c Virtually all children with diabetes from West-Berlin N= 494, 262 boys, 232 girls Median age at onset: 11 (1 to 17) years Annual fluoresceine angiograms Median follow-up: 9 years
: Continuous Exponential Relationship between retinopathy and long-term-HbA1c Virtually all children with diabetes from West-Berlin N= 494, 262 boys, 232 girls Median age at onset: 11 (1 to 17) years Annual fluoresceine angiograms Median follow-up: 9 years.")
16
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Should risk of severe hypoglycemia influence the targets in young children ?

17
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Adults with diabetes Parents of IDDM children (mean age 8.1 years) - without severe hypo - with severe hypo n=78 n=46 n=31 n=15 1.88 ± 0.6 2.94 ± 0.6 2.84 ± 0.6 3.18 ± 0.6 0.001 0.040 No influence: confidence to detect or treat hypoglycaemia in their children Average Hypoglycaemia Fear Score Maternal fear of Hypoglycemia in their Children with Insulin dependent Diabetes mellitus Clarke et al.; JPEM 11 (Suppl.1): 189-194, 1998
 - without severe hypo - with severe hypo n=78 n=46 n=31 n= ± ± ± ± No influence: confidence to detect or treat hypoglycaemia in their children Average Hypoglycaemia Fear Score Maternal fear of Hypoglycemia in their Children with Insulin dependent Diabetes mellitus Clarke et al.; JPEM 11 (Suppl.1): , 1998")
18
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Can my child die during a hypoglycaemia ? The dead in bed syndrome Author Study Age Group Total Dead in bed Age period (years) deaths (n) (years) Tattersall (1991) 1989 - 22 12 - 43 Thodarson (1995) 1981-90 0 - 40 240 16 7 - 35 Sartor (1995) 1977-85 0 - 28 33 9 15 - 23 Sudden death of young people with diabetes without complications found dead in bed out of apparent health the day before. Hypoglycaemia as a possible cause.
 deaths (n) (years) Tattersall (1991) Thodarson (1995) Sartor (1995) Sudden death of young people with diabetes without complications found dead in bed out of apparent health the day before. Hypoglycaemia as a possible cause..")
19
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Why do children with diabetes die ? Causes of death in children with insulin dependent diabetes 1990-96 Edge JAet al. Arch Dis Child (1999) 81: 318-23 116 deaths ca. 150600 Children w. Diabetes (0 to 19 years) 83 deaths related to DM 33 deaths not related to DM 26 at home (9 dead in bed) 8 on way to hospital 45 in hospital during DKA therapy 4 hypoglycemia possible 10 DKA 10 DKA likely
 81: deaths ca Children w. Diabetes (0 to 19 years) 83 deaths related to DM 33 deaths not related to DM 26 at home (9 dead in bed) 8 on way to hospital 45 in hospital during DKA therapy 4 hypoglycemia possible 10 DKA 10 DKA likely.")
20
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Influence of social factors on the mortality of adults with type 1 diabetes Robinson N. et. al.: Social Deprivation and Mortality in Adults with Diabetes Mellitus. Diab Med (1998) 15:205-212 Odds Ratio(95% CI) Low social status1.34(0.61-2.96) Left school before age 16 y3.98(1.96-8.06) social housing 2.57(1.37-4.91) unemployed 3.10(1.67-5.79) Risk factor 800 Patients with type 1 diabetes (Follow-up 8.4 years)
 15: Odds Ratio(95% CI) Low social status1.34( ) Left school before age 16 y3.98( ) social housing 2.57( ) unemployed 3.10( ) Risk factor 800 Patients with type 1 diabetes (Follow-up 8.4 years).")
21
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Same targets for all age paediatric age groups – the Hannover approach HbA1c below 7.5% prevent ketoacidosis prevent school failure prevent hypoglycemia

22
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus The ISPAD Vote September 28th,2007 Majority for age independent targets Target HbA1c < 8%: Target HbA1c < 7.5%: Target HbA1c < 7.0%:

23
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus But is the HbA1c the right target ?

24
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus The DCCT Research Group. The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the Diabetes Control and Complications Trial. Diabetes 1995; 44: 968-83
 to the risk of development and progression of retinopathy in the Diabetes Control and Complications Trial. Diabetes 1995; 44:")
25
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus 5 10 15 20 25 Time of diagnosis of background retinopathie (DMduration (years) <66-77-88-99-1010-1111-1212-13>13 -18.920.420.920.319.819.018.517.5 Longterm HbA1c (%) Median Age (Years) Danne et. al, Diab Care 17: 1390-96, 1994 HbA1c is a bad predictor of retinopathy in indvidual adolescents – the Berlin Retinopathy-Study

26
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus The new information with CGM: Glycemic variability Comparison blinded FreeStyle Navigator vs. HbA1c Glucose Mean vs. HbA1c Glucose S.D. vs. HbA1c r=0.801 p<0.0001 r=0.675 p=0.0004 German Diabetes Association 2008

27
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Hannover Navigator Study Other Measures of Glycemic Control MaskedUnmasked% Difference P-value Glucose Mean (mg/dL)Mean172164-4.5%0.0577 S.D.2724 N23 Glucose S.D. (mg/dL)Mean61.856.1-9.1%0.0037 S.D.11.914.2 N23 MAGE nadir to peak events (mg/dL) Mean135.2125.1-7.4%0.0462 S.D.28.928.1 N23 MAGE peak to nadir events (mg/dL) Mean140.6126.8-9.9%0.0017 S.D.28.329.7 N23
Mean % S.D N23 MAGE nadir to peak events (mg/dL) Mean % S.D N23 MAGE peak to nadir events (mg/dL) Mean % S.D N23.")
28
K INDER K RANKENHAUS AUF DER B ULT für Kinder und Jugendliche Akademisches Lehrkrankenhaus Children with diabetes need insulin, love and care …and clear targets

Ähnliche Präsentationen

>")










 Grüß Gott (AUT)/Guten Tag (DE) – f>")






 das Aktiv (Active Voice)>")