Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
GERHARD RACZ A.Ö. KH OBERWART INTERNE ABTEILUNG
HERZINFARKT 2007 GERHARD RACZ A.Ö. KH OBERWART INTERNE ABTEILUNG

2
EPIDEMIOLOGIE Herz-Kreislauferkrankungen häufigste Todesursachen in Industrieländern (48 %) Spitalsstatistik 2002: Herzinfarkte jährlich stationär im KH Sterblichkeit im Mittel bei 13 % (Frauen 21 %) 25-30 % versterben vor Arztkontakt
 % versterben vor Arztkontakt.")
3
STATISTIK ZUR THERAPIE
1/3 Akut-PCI 1/3 Lyse 1/3 Keine Reperfusion (höchste Spitalssterblichkeit (18-25 %)
")
4
DEFINITIONEN Myokardinfarkt:
Erhöhung kardialer Nekrosemarker (Trop, CK-MB) in Zusammenhang mit typischer klinischer Symptomatik, entsprechenden EKG-Veränderungen o. angiographischem Befund
 in Zusammenhang mit typischer klinischer Symptomatik, entsprechenden EKG-Veränderungen o. angiographischem Befund.")
5
DEFINITIONEN NSTEMI: MCI ohne ST-Streckenhebung im Ruhe-EKG STEMI:
MCI mit typischen ST-Streckenhebungen im Ruhe-EKG

6
DEFINITIONEN Instabile Angina pectoris:
AP in Ruhe innerhalb der letzten 48 h o. neu aufgetretene AP bzw. deutliche Verschlechterung einer stabilen AP mit Beschwerden bereits bei leichtester Belastung

7
Atherosclerotic Lesion in a Human Artery
Figure 1. Atherosclerotic Lesion in a Human Artery. Panel A shows a cross-sectioned coronary artery from a patient who died of a massive myocardial infarction. It contains an occlusive thrombus superimposed on a lipid-rich atherosclerotic plaque. The fibrous cap covering the lipid-rich core has ruptured (area between the arrows), exposing the thrombogenic core to the blood. Trichrome stain was used, rendering luminal thrombus and intraplaque hemorrhage red and collagen blue. Panel B is a high-power micrograph of the area in Panel A indicated by the asterisk and shows that the contents of the atheromatous plaque have seeped through the gap in the cap into the lumen, suggesting that plaque rupture preceded thrombosis (the asterisk indicates cholesterol crystals). (Panels A and B courtesy of Dr. Erling Falk, University of Aarhus, Aarhus, Denmark.) Panel C illustrates the consequences of the activation of immune cells in a coronary plaque. Microbes, autoantigens, and various inflammatory molecules can activate T cells, macrophages, and mast cells, leading to the secretion of inflammatory cytokines (e.g., interferon-{gamma} and tumor necrosis factor) that reduce the stability of plaque. The activation of macrophages and mast cells also causes the release of metalloproteinases and cysteine proteases, which directly attack collagen and other components of the tissue matrix. These cells may also produce prothrombotic and procoagulant factors that directly precipitate the formation of thrombus at the site of plaque rupture. Hansson G. N Engl J Med 2005;352:
, exposing the thrombogenic core to the blood. Trichrome stain was used, rendering luminal thrombus and intraplaque hemorrhage red and collagen blue. Panel B is a high-power micrograph of the area in Panel A indicated by the asterisk and shows that the contents of the atheromatous plaque have seeped through the gap in the cap into the lumen, suggesting that plaque rupture preceded thrombosis (the asterisk indicates cholesterol crystals). (Panels A and B courtesy of Dr. Erling Falk, University of Aarhus, Aarhus, Denmark.) Panel C illustrates the consequences of the activation of immune cells in a coronary plaque. Microbes, autoantigens, and various inflammatory molecules can activate T cells, macrophages, and mast cells, leading to the secretion of inflammatory cytokines (e.g., interferon-{gamma} and tumor necrosis factor) that reduce the stability of plaque. The activation of macrophages and mast cells also causes the release of metalloproteinases and cysteine proteases, which directly attack collagen and other components of the tissue matrix. These cells may also produce prothrombotic and procoagulant factors that directly precipitate the formation of thrombus at the site of plaque rupture. Hansson G. N Engl J Med 2005;352:")
8
The Cytokine Cascade Figure 5. The Cytokine Cascade. Activated immune cells in the plaque produce inflammatory cytokines (interferon-{gamma}, interleukin-1, and tumor necrosis factor [TNF]), which induce the production of substantial amounts of interleukin-6. These cytokines are also produced in various tissues in response to infection and in the adipose tissue of patients with the metabolic syndrome. Interleukin-6, in turn, stimulates the production of large amounts of acute-phase reactants, including C-reactive protein (CRP), serum amyloid A, and fibrinogen, especially in the liver. Although cytokines at all steps have important biologic effects, their amplification at each step of the cascade makes the measurement of downstream mediators such as CRP particularly useful for clinical diagnosis. Hansson G. N Engl J Med 2005;352:
, which induce the production of substantial amounts of interleukin-6. These cytokines are also produced in various tissues in response to infection and in the adipose tissue of patients with the metabolic syndrome. Interleukin-6, in turn, stimulates the production of large amounts of acute-phase reactants, including C-reactive protein (CRP), serum amyloid A, and fibrinogen, especially in the liver. Although cytokines at all steps have important biologic effects, their amplification at each step of the cascade makes the measurement of downstream mediators such as CRP particularly useful for clinical diagnosis. Hansson G. N Engl J Med 2005;352:")
9
KLINIK Plötzlicher Brustschmerz (ev. mit Ausstrahlung) - Vernichtungsschmerz Vegetative Symptome: Kaltschweißigkeit, Blässe, Übelkeit, Erbrechen

10
DIFFERENTIALDIAGNOSEN
Kardiovaskuläre Erkrankungen: (Tachykarde) Rhythmusstörungen Perikarditis Myokarditis Aortendissektion Hypertensive Krise Akute Linksherzinsuffizienz
 Rhythmusstörungen. Perikarditis. Myokarditis. Aortendissektion. Hypertensive Krise. Akute Linksherzinsuffizienz.")
11
DIFFERENTIALDIAGNOSEN
Pulmonale Erkrankungen: Lungenembolie Pleuritis Pneumothorax Skeletterkrankungen: Rippenfraktur/Prellung BWS-Erkrankungen Tietze-Syndrom Gastrointestinalerkrankungen: Ösophagitis/Ruptur Ulcus (Perforation) Akute Pankreatitis Gallenkolik Andere: Herpes zoster Tumorerkrankungen
 Akute Pankreatitis. Gallenkolik. Andere: Herpes zoster. Tumorerkrankungen.")
12
UA/NSTEMI Diagnostische Maßnahmen:
- Ruheschmerz über 20 min. Dauer Transport ins KH unter ärztlicher Aufsicht - Im KH sofortige Untersuchung durch einen Arzt - 12-Kanal-EKG vom NA prähospital - Erneute EKG-Registrierung bei jeder neuen Schmerzepisode sowie nach 6 Stunden - Sofortige Blutabnahme zur Messung von Troponin I oder T - Neg. Troponin + Schmerz < 4 h Wiederholung der Troponin-Bestimmung nach insgesamt 6 h nach Schmerzbeginn

13
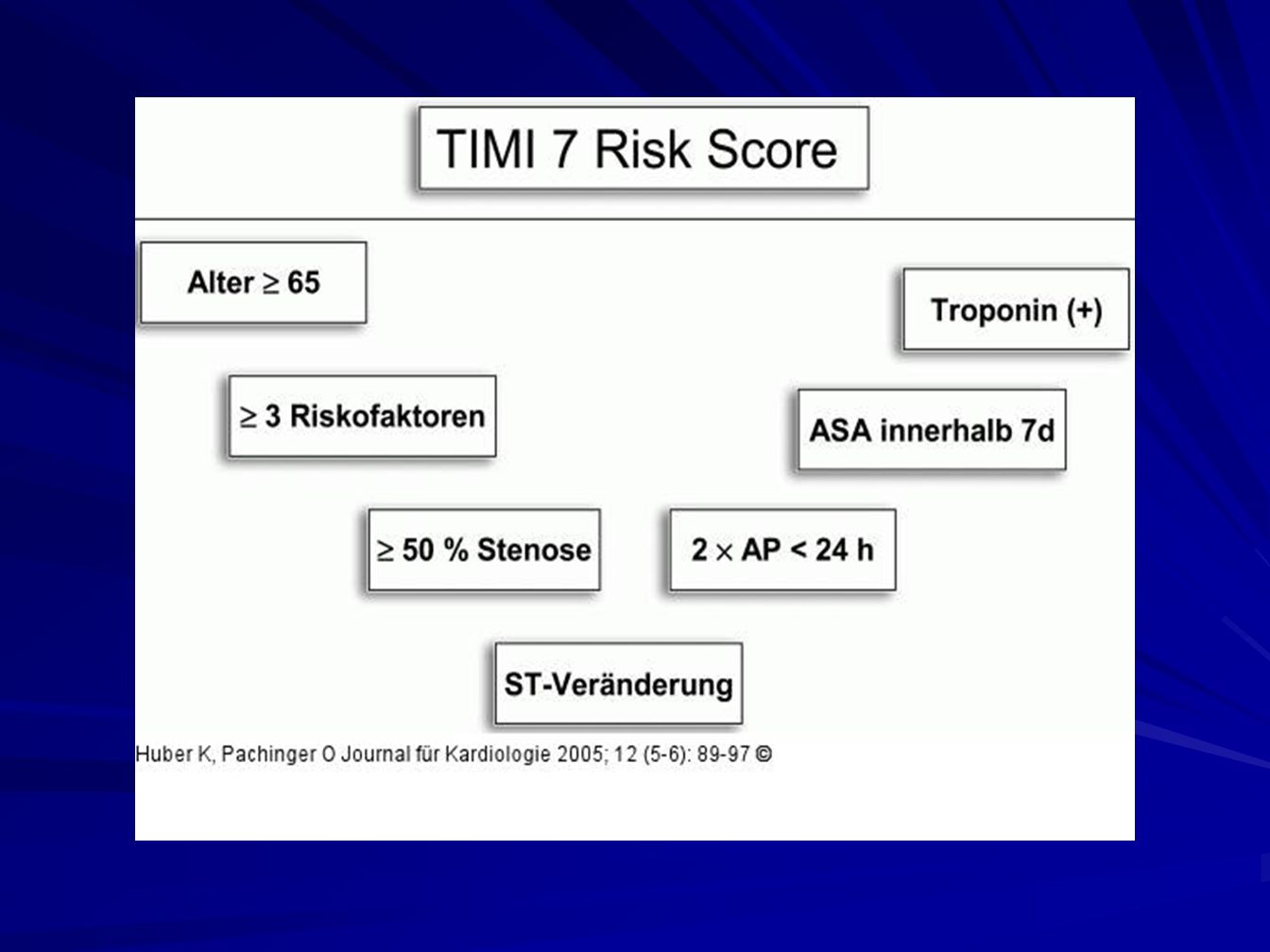
UA/NSTEMI Hochrisikopatienten: Troponinerhöhung
ST-Senkung (> 0,1 mV) im EKG Hämodynamische Instabilität Kammerflimmern/flattern, VT Diabetes mellitus
 im EKG. Hämodynamische Instabilität. Kammerflimmern/flattern, VT. Diabetes mellitus.")
14
UA/NSTEMI Besonderheiten der Troponinmessung
Erhöhte Werte frühestens nach 4 h Nicht-ACS induzierte Erhöhungen: Herzinsuffizienz Hypertensive Krise Tachykardien Myo- Perikarditis Lungenembolie Niereninsuffizienz Labor-Fehler

15
GENERELLE THERAPIEEMPFEHLUNGEN
Allgemeinmaßnahmen: Lagerung mit 30 Grad angehobenem Oberkörper Herz-Lungen-Auskultation Periphere Verweilkanüle RR-Messung 12-Kanal-EKG Rhythmusmonitoring

16
GENERELLE THERAPIEEMPFEHLUNGEN
Primärtherapie: - O2 über Nasensonde/Maske (4-8 l/min) - Glyceroltrinitrat 0,4-0,8 mg s.l., ev. Infusion 1-6 mg/h - Morphin 3-5 mg i.v. - Bei Übelkeit/Erbrechen Antiemetika - Acetylsalicylsäure (> 250 mg i.v.) - Heparin 70 U/kg, max IE i.v. oder Enoxaparin 30 mg i.v. + 1mg/kg s.c.
 - Glyceroltrinitrat 0,4-0,8 mg s.l., ev. Infusion 1-6 mg/h. - Morphin 3-5 mg i.v. - Bei Übelkeit/Erbrechen Antiemetika. - Acetylsalicylsäure (> 250 mg i.v.) - Heparin 70 U/kg, max IE i.v. oder. Enoxaparin 30 mg i.v. + 1mg/kg s.c.")
17
SPEZIELLE THERAPIEEMPFEHLUNGEN (ESC-GUIDELINES)
PCI spätestens nach 48 h (so früh wie möglich) Alle Patienten Clopidogrel „loading dose“ 300 mg Loading dose 600 mg noch nicht in den Leitlinien (Studien dazu schon beendet, z.B. ISAR-REACT 2) Bei Hochrisikopatienten: GPIIb/IIIa-Blocker
 Alle Patienten Clopidogrel „loading dose 300 mg. Loading dose 600 mg noch nicht in den Leitlinien (Studien dazu schon beendet, z.B. ISAR-REACT 2) Bei Hochrisikopatienten: GPIIb/IIIa-Blocker.")
20
STEMI Klinik ähnlich, aber keine Besserung auf Nitrogabe
Maskierte Symptomatik bei Frauen und Diabetikern Beschwerden in den Tagen und Wochen zuvor

21
STEMI - DIAGNOSTIK 12-Ableitungs-EKG !!!
- ST-Streckenhebung von > 0,1 mV in mindestens 2 zusammenhängenden Extremitätenableitungen o. - ≥ 0,2 mV in mindestens 2 zusammenhängenden BWA o. - LSB mit infarkttypischer Symptomatik Messung von Biomarkern unwichtig für Therapieentscheidung

22
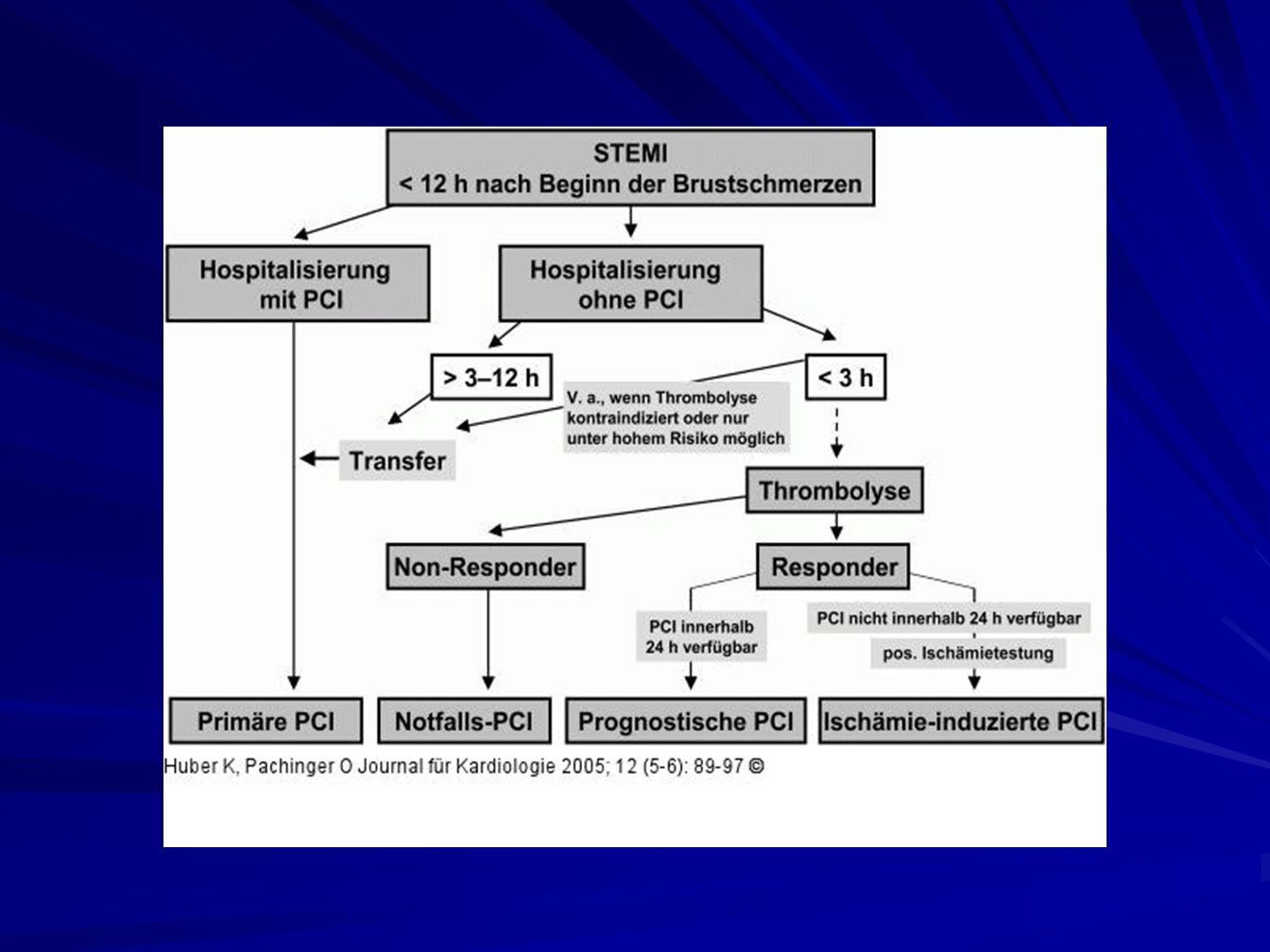
STEMI - THERAPIE Primäre PCI ist bevorzugte Behandlungsstrategie
Voraussetzung: Zeitlimits Fibrinolyse zweitbeste Option falls diese Limits nicht eingehalten werden (können)
")
24
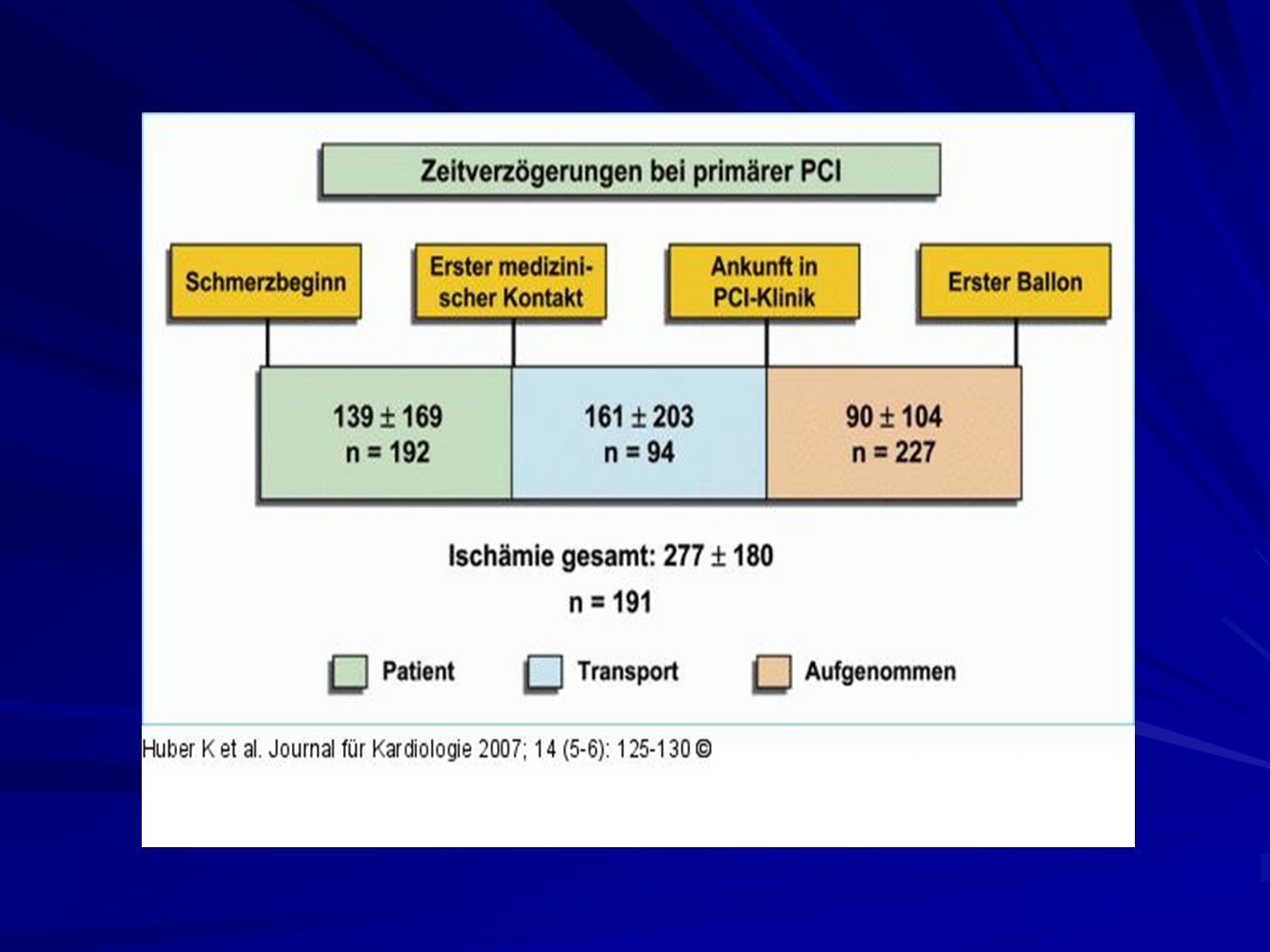
ZEITLIMITS BEI REPERFUSIONSTHERAPIE
Erstkontakt bis prästationäre Fibrinolyse („contact to needle“): < 30 Minuten Einleitung der Fibrinolyse stationär (“door to needle”): < 30 Minuten Maximal tolerabler Zeitverlust PCI vs. Lyse: < 60 Minuten Erstkontakt bis zur PCI (“contact to balloon”): < 90 Minuten
: < 30 Minuten. Einleitung der Fibrinolyse stationär ( door to needle ): < 30 Minuten. Maximal tolerabler Zeitverlust PCI vs. Lyse: < 60 Minuten. Erstkontakt bis zur PCI ( contact to balloon ): < 90 Minuten.")
26
FIBRINOLYSE - KONTRAINDIKATIONEN
ABSOLUT: - Schlaganfall in den letzten 6 Monaten (hämorrhagisch zeitunabhängig) - Trauma, Operation, Kopfverletzung innerhalb der letzten 3 Wochen - Neoplasma o. neurolog. ZNS- Erkrankung - Magen-Darm-Blutung innerhalb des letzten Monats - Bekannte Blutungsdiathese - Dissezierendes Aortenaneurysma
 - Trauma, Operation, Kopfverletzung innerhalb der letzten 3 Wochen. - Neoplasma o. neurolog. ZNS- Erkrankung. - Magen-Darm-Blutung innerhalb des letzten Monats. - Bekannte Blutungsdiathese. - Dissezierendes Aortenaneurysma.")
27
FIBRINOLYSE - KONTRAINDIKATIONEN
RELATIV: - TIA in den letzten 6 Monaten - Orale Antikoagulantientherapie - Schwangerschaft - Nicht-komprimierbare Gefäßpunktionen - Therapierefraktäre Hypertonie (> 180 mmHg) - Aktives Ulcusleiden - Floride Endokarditis - Fortgeschrittene Lebererkrankung - Traumatische Reanimationsmaßnahmen
 - Aktives Ulcusleiden. - Floride Endokarditis. - Fortgeschrittene Lebererkrankung. - Traumatische Reanimationsmaßnahmen.")
28
BEGLEITTHERAPIE ZUR LYSE
Aspirin 250 – 500 mg i.v. Heparin: Bolus 60 IE/kg, max IE Keine niedermolekularen Heparine (erhöhte Blutungsneigung); ev. Reduktion der Dosis auf 75 % (ExTRACT-TIMI-25) Clopidogrel (Studien nur bei Patienten unter 75 Jahren)
; ev. Reduktion der Dosis auf 75 % (ExTRACT-TIMI-25) Clopidogrel (Studien nur bei Patienten unter 75 Jahren)")
30
BEURTEILUNG DES LYSEERFOLGS
Patient beschwerdefrei, kreislaufstabil Rückgang der ST-Hebungen um mindestens 50 % innerhalb von 90 Minuten

31
Kaplan-Meier Estimates of the Cumulative Rate of the Composite Primary End Point (Death, Recurrent Myocardial Infarction, Severe Heart Failure, or Cerebrovascular Event) within Six Months Figure 1. Kaplan-Meier Estimates of the Cumulative Rate of the Composite Primary End Point (Death, Recurrent Myocardial Infarction, Severe Heart Failure, or Cerebrovascular Event) within Six Months. PCI denotes percutaneous coronary intervention, and CI confidence interval. Gershlick A et al. N Engl J Med 2005;353: In conclusion, the trial found that rescue PCI after failed thrombolytic treatment was associated with a statistically significant reduction in the incidence of major adverse cardiac and cerebrovascular events, as compared with either repeated thrombolysis or conservative management. These results indicate that rescue PCI, with transfer to a tertiary site if required, should be considered for patients in whom thrombolysis for myocardial infarction with ST-segment elevation fails to achieve reperfusion
 within Six Months. PCI denotes percutaneous coronary intervention, and CI confidence interval. Gershlick A et al. N Engl J Med 2005;353: In conclusion, the trial found that rescue PCI after failed thrombolytic treatment was associated with a statistically significant reduction in the incidence of major adverse cardiac and cerebrovascular events, as compared with either repeated thrombolysis or conservative management. These results indicate that rescue PCI, with transfer to a tertiary site if required, should be considered for patients in whom thrombolysis for myocardial infarction with ST-segment elevation fails to achieve reperfusion.")
32
STEMI Spitalsmortalität in Wien

33
DANKE FÜR DIE AUFMERKSAMKEIT

Ähnliche Präsentationen
















 bei Herzinsuffizienz>")




