Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Westfälische Wilhelms-Universität Münster
Primär- und Sekundär-prävention in der Kardiologie Westfälische Wilhelms-Universität Münster Dr. Jan Heidrich, MSc Institut für Epidemiologie und Sozialmedizin Universitätsklinikum Münster Münster Herzzentrum Münster Prof. Dr. med. Holger Reinecke Medizinische Klinik und Poliklinik C Universitätsklinikum Münster Münster

2
Prävention in der Kardiologie
WWU Münster (Endokarditisprophylaxe) Antikoagulation bei idiopathischem Vorhofflimmern Plötzlicher Herztod (Risikogruppen, Frühdefibrillation) Verhaltensweisen/“Lifestyle“ Primäre und sekundäre Prävention der Arteriosklerose Life-Style Veränderungen Stellenwert von Medikamenten in der Primärprävention Medikamentöse Sekundärprävention
 Antikoagulation bei idiopathischem Vorhofflimmern. Plötzlicher Herztod (Risikogruppen, Frühdefibrillation) Verhaltensweisen/ Lifestyle Primäre und sekundäre Prävention der Arteriosklerose. Life-Style Veränderungen. Stellenwert von Medikamenten in der Primärprävention. Medikamentöse Sekundärprävention.")
3
Epidemiologie How do we treat pts with a typical ECG pattern?
WWU Münster Epidemiologie How do we treat pts with a typical ECG pattern? Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.
 Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.")
4
Zeitlicher Trend der kardiovaskulären Mortalität in Deutschland Sterbefälle pro Einwohner

5
Inzidenz der KHK in Deutschland 2003 MONICA/KORA Herzinfarkt-Register
Quelle: Löwel et al 2006

6
Hochrechnung der Post-Infarkt-Patienten
Hochrechnung der Post-Infarkt-Patienten* auf die 30–79-jährige deutsche Bevölkerung, 1997/1998, Frauen, Männer, Gesamt Nationaler Gesundheitssurvey 1998 * Zahl der prävalenten Post-Infarkt Patienten = Zahl der Patienten, die einen Herzinfarkt zur Zeit des Survey überlebt hatten. Quelle: Wiesner G, et al. Zum Herzinfarktgeschehen in der BRD. Gesundheitswesen 1999; 61: S72–78

7
Ursachen des Rückgangs der KHK Mortalität
42% des Rückganges durch Therapiemaßnahmen 58% des Rückganges durch Reduktion von Risikofaktoren auf Bevölkerungsebene Unal et al. Circulation 2004

8
Vergleich von Studien Rückgang der KHK-Mortalität durch

9
Vergleich von vermiedenen/ verschobenen Todesfällen und gewonnenen Lebensjahren durch Veränderungen der Risikofaktoren und Behandlung in England und Wales

10
Pathophysiologie How do we treat pts with a typical ECG pattern?
WWU Münster Pathophysiologie How do we treat pts with a typical ECG pattern? Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.
 Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.")
11
How do we treat pts with a typical ECG pattern?
Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.
 Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.")
12
Wo beginnt Prävention? Prävention Jahre Erkrankung Früherkennung
WWU Münster Prävention Erkrankung Früherkennung – CRP, EBT, MS-CT Risikostratifizierung Jahre

13
Risikofaktoren How do we treat pts with a typical ECG pattern?
WWU Münster Risikofaktoren How do we treat pts with a typical ECG pattern? Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.
 Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.")
14
WWU Münster Risikofaktoren...

15
Risikofaktoren und Prävention Risikofaktoren
WWU Münster Risikofaktoren und Prävention Risikofaktoren modifizierbar Rauchen Übergewicht/Ernährung Körperliche Inaktivität Exzessiver Alkoholmißbrauch Hypertonus Dylipidämien hohes LDL-Cholesterin niedriges HDL-Cholesterin hohe Triglyceride hohes Lipoprotein(a) Diabetes mellitus Hyperhomocysteinämie nicht modifizierbar positive Eigenanamnese positive Familienanamnese Alter Geschlecht Neuerer Risikofaktor Nierenfunktionseinschränkung How do we treat pts with a typical ECG pattern? Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.
 Diabetes mellitus. Hyperhomocysteinämie. nicht modifizierbar. positive Eigenanamnese. positive Familienanamnese. Alter. Geschlecht. Neuerer Risikofaktor. Nierenfunktionseinschränkung. How do we treat pts with a typical ECG pattern Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.")
16
Primärprävention How do we treat pts with a typical ECG pattern?
WWU Münster Primärprävention How do we treat pts with a typical ECG pattern? Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.
 Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.")
17
Primärprävention: Fallvorstellung
WWU Münster 42jähriger Mann RF: Rauchen seit 22 LJ, 183 cm/95 kg, RR 145/90 mmHg, GC 245, LDL 165, HDL 32, Vater 63 J Myokardinfarkt Seit 8 Wochen sowohl bei Belastungen im Fitneßstudio als auch in Ruhe (Fernsehen) ca. 2-3x/Woche linksseitige Thoraxschmerzen EKG & Belastungs-EKG & Echo unauffällig
 ca. 2-3x/Woche linksseitige Thoraxschmerzen. EKG & Belastungs-EKG & Echo unauffällig.")
18
Weitere Risikofaktoren für KHK
Soziale Isolation Depression

19
Das KHK-Risiko ist multifaktoriell – Framingham Heart Study (FHS)
RR syst. Serum Cholesterin Diabetes Rauchen LVH (EKG) 105 195 105195 185 335 Gordon, Sorlie, Kannel: FHS 16year Follow-Up (1971) 6-Jahres-KHK-Risiko pro 100 Personen männl., 55 J. 10 20 30 40 50 60 70 80 3,7 8,4 10,6 28,1 15,7 54,5 36,3 26,7 21,8
 105 Gordon, Sorlie, Kannel: FHS 16year Follow-Up (1971) 6-Jahres-KHK-Risiko pro 100 Personen. männl., 55 J ,7. 8,4. 10,6. 28,1. 15,7. 54,5. 36,3. 26,7. 21,8.")
20
Stratifizierung mit Risikoscores

22
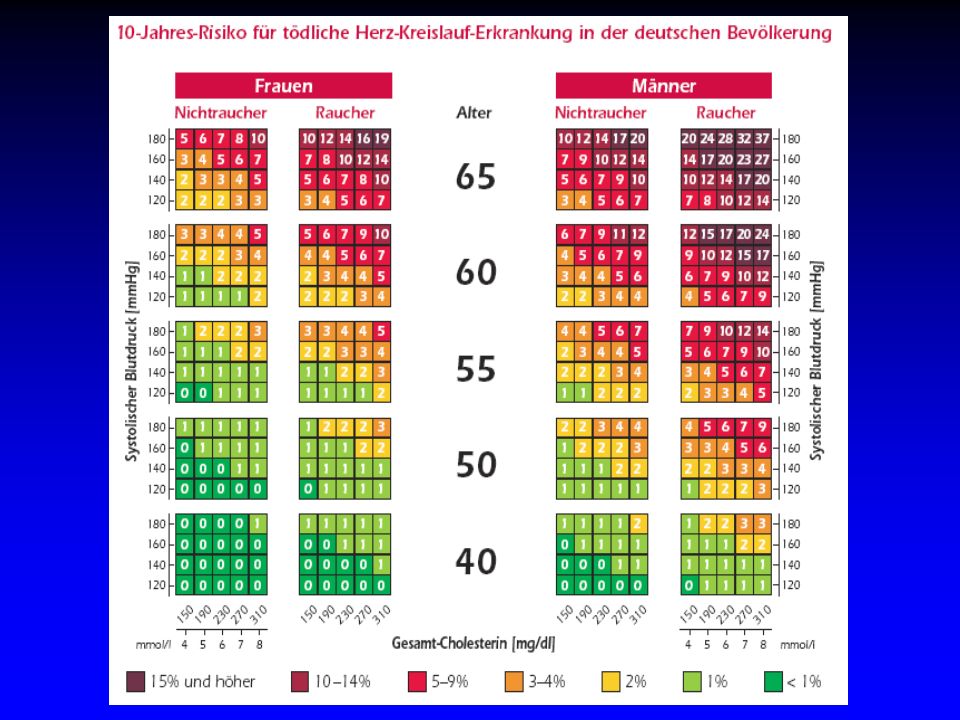
Anwendung der SCORE Risikotabellen
Relatives Risiko Für Differenz 60 mmg SBP RR = 10 / 3 ~ 3 Relatives Risiko Raucher vs. Nichtraucher RR = 10 / 5 = 2 Relatives Risiko pro 60 mm SBP plus Rauchen RR = 10 / 2 = 5

23
HEARTSCORE Die SCORE-Risikotabellen basieren auf Daten von 12 europäischen Studien mit: Teilnehmern ( Frauen, Männer) 2,7 Millionen Personenjahren Follow-up 7.934 tödlichen Herz-Kreislauf-Erkrankungen, davon wegen KHK Für Deutschland aktuelle Zahlen zu Risikofaktoren und Mortalität berücksichtigt Risikotabellen angepasst

24
Weitere gebräuchliche Risikoscores
Framingham Risk Score (USA, 1998) Basiert auf Daten von ~5.300 M/ W, Alter J. Mortalität + Morbidität Überschätzt Risiko für D und europäische Populationen QRISK (UK, 2007) Basiert auf Daten von 1.28 Mio M/ W, Alter J. aus hausärztlichen Praxen Neuester Score, umfangreich (z. B. SES) PROCAM (Münster, 1998) Basiert auf Daten von ~5.400 Männern, Alter Jahre, Angestellte aus der öffentlichen Verwaltung und Unternehmen; bis dato erweitert Abgeleitete Scores, z. B. Arriba-Herz
 Basiert auf Daten von ~5.300 M/ W, Alter J. Mortalität + Morbidität. Überschätzt Risiko für D und europäische Populationen. QRISK (UK, 2007) Basiert auf Daten von 1.28 Mio M/ W, Alter J. aus hausärztlichen Praxen. Neuester Score, umfangreich (z. B. SES) PROCAM (Münster, 1998) Basiert auf Daten von ~5.400 Männern, Alter Jahre, Angestellte aus der öffentlichen Verwaltung und Unternehmen; bis dato erweitert. Abgeleitete Scores, z. B. Arriba-Herz.")
25
CAVE zu Risikoscores Das Gesamt-Herz-Kreislauf-Risiko kann höher sein als in den Risikotabellen angegeben wird: wenn sich die Person der nächsten Alterskategorie nähert bei asymptomatischen Patienten mit prä-klinischen Zeichen von Atherosklerose (z.B. CT, Ultraschall) bei Patienten mit einer Familienanamnese für vorzeitige HKK bei Personen mit niedrigem HDL-Cholesterin, mit erhöhten Triglyceriden, mit gestörter Glukose-Toleranz und mit erhöhten Spiegeln von CRP, Fibrinogen, Homocystein, Apo B oder Lp(a) bei übergewichtigen Personen und solchen ohne körperliche Aktivität
 bei Patienten mit einer Familienanamnese für vorzeitige HKK. bei Personen mit niedrigem HDL-Cholesterin, mit erhöhten Triglyceriden, mit gestörter Glukose-Toleranz und mit erhöhten Spiegeln von CRP, Fibrinogen, Homocystein, Apo B oder Lp(a) bei übergewichtigen Personen und solchen ohne körperliche Aktivität.")
26
Einschätzung des kardiovaskulären Risikos durch
Allgemeinmediziner im Vergleich zur europäischen Risikotabelle Unterschätzung Übereinstimmung Überschätzung Roncaglioni et al. 2004

27
Zusammenfassung Risikoscores
Risikoscores sind geeignet, das absolute HKK-Risiko abzuschätzen und Hochrisikopatienten zu identifizieren Risikoscores beziehen sich ausschließlich auf die Primärprävention Scores ermöglicht eine anschauliche Darstellung des HKK-Risikos Risikoscores sind Hilfen in der Risikokommunikation/ Arzt-Patienten-Gespräch Grenzwerte (z. B. ≥5% für Hochrisikodefinition) können als Richtwerte für eine intensivere Betreuung (nicht notwendigerweise medikamentöse Behandlung) betrachtet werden Risiko kann von den aus Risikoscores berechnetem Risiko abweichen Risikoscores können eine Entscheidungshilfe in klinischen Praxis sein
 können als Richtwerte für eine intensivere Betreuung (nicht notwendigerweise medikamentöse Behandlung) betrachtet werden. Risiko kann von den aus Risikoscores berechnetem Risiko abweichen. Risikoscores können eine Entscheidungshilfe in klinischen Praxis sein.")
28
Was ist mit der Veränderung von Ernährung und Lebensstil zu erreichen?

29
Die „Lyon Diet Heart Study“: Überlebenskurven, kardiovaskuläre Todesfälle und nicht-tödliche Herzinfarkte (AMI) zusammengefasst Quelle: Lorgeril M et al. Lancet 1994; 343: 1458

30
Die sechs Gebote der Kreta-Ernährung
Mehr (Vollkorn) Brot Mehr Gemüse und Hülsenfrüchte Mehr Fisch (Seefisch) Rind-, Schweine- und Lammfleisch durch Geflügel ersetzen Kein Tag ohne Obst Butter und Sahne durch Rapsöl*-Margarine ersetzen * Fettsäurezusammensetzung ist sehr ähnlich dem Olivenöl; allerdings enthielt die Margarine 5% 18:3n-3 statt 0,6% in Olivenöl Quelle: Renaud SC. Prostagl. Leukotr. Essent. Fatty Acids 1997; 57: 423–427
 Brot. Mehr Gemüse und Hülsenfrüchte. Mehr Fisch (Seefisch) Rind-, Schweine- und Lammfleisch durch Geflügel ersetzen. Kein Tag ohne Obst. Butter und Sahne durch Rapsöl*-Margarine ersetzen. * Fettsäurezusammensetzung ist sehr ähnlich dem Olivenöl; allerdings enthielt die Margarine 5% 18:3n-3 statt 0,6% in Olivenöl. Quelle: Renaud SC. Prostagl. Leukotr. Essent. Fatty Acids 1997; 57: 423–427.")
31
Einhaltung der mediterranen Ernährung und Überlebenszeit in einer griechischen Kohorte von Männern und Frauen, Beobachtungszeit 44 Monate Quelle: Trichopoulou A et al. Mediterranean diet and mortality. N Engl J Med 2003; 348: 2593

32
Beziehung zwischen Alkohol und KHK
kkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkk Source: Corrao G et al. Alcohol and coronary heart disease: a meta-analysis. Addiction 2000; 95: 1505–1523

33
Beziehung zwischen Alkohol und KHK
Source: Corrao G et al. Alcohol and coronary heart disease: a meta-analysis. Addiction 2000; 95: 1505–1523

34
Beziehung zwischen Rauchen und KHK
Law 2003

35
Rückgang des vaskulären Risikos in Abhängigkeit von der Zeit nach Rauchstopp – Nurses‘ Health Study
Quelle: Kenfield et al. JAMA 2008; 299: 2037

36
Körperliche Aktivität
Körperliche Aktivität, (z.B. schnelles Gehen, Joggen, Radfahren, Schwimmen) möglichst täglich und nicht unter 30–45 Minuten führt bei (gesunden) Männern und Frauen zu einer Risikoreduktion von 30 bis 45% für Herz-Kreislauf-Krankheiten und für die Gesamtmortalität. Quellen: Physical activity and health: a report of the Surgeon General. Centre for Disease Control and Prevention. Atlanta, 1996 Blair SN et al. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA 1996; 276: 205–210
 möglichst täglich und nicht unter 30–45 Minuten führt bei (gesunden) Männern und Frauen zu einer Risikoreduktion von 30 bis 45% für Herz-Kreislauf-Krankheiten und für die Gesamtmortalität. Quellen: Physical activity and health: a report of the Surgeon General. Centre for Disease Control and Prevention. Atlanta, Blair SN et al. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA 1996; 276: 205–210.")
37
Frauen mit niedrigem Risikoverhalten
Primäre Prävention der KHK bei Frauen durch Ernährung und Lebensstil Frauen mit niedrigem Risikoverhalten Nicht-Rauchen BMI < 25 kg/m2 Moderate bis ausgeprägte körperliche Aktivität 30 Minuten/Tag Gehörten zu den oberen 40% der Kohorte bezüglich hoher Aufnahme von Ballaststoffen, n–3 Fettsäuren aus Meeresfisch, Folat, hohe P/S Ratio, geringer Anteil an Trans-Fettsäuren und geringe glykämische Belastung Alkohol 5 g/Tag Quelle: Stampfer MJ et al. N Engl J Med 2000; 343: 16–22

38
KHK-Risiko bei Frauen mit niedrigem Risikoverhalten in der „Nurses’ Health Study“ 1980–1994, Frauen, Alter 34–59 Jahre Quelle: Stampfer MJ et al. N Engl J Med 2000; 343: 16–22

39
Risikoreduktion durch mehrere Maßnahmen in der Praxis – Prioritäten setzen
Rel. Risiko Kumulativ Rauchstopp ca. 35% 65% Bewegung 65x(1-0.35)=43% Fisch/Omega ca. 15% 43x(1-0.15)=36% Med. BDr ca. 25% 36x(1-0.25)=27% ASS ca. 20% 27x(1-0.2)=22% Statine ca % 22x(1-0.2)=17% Modifiziert nach: Arriba; arriba-hausarzt.de
=43% Fisch/Omega. ca. 15% 43x(1-0.15)=36% Med. BDr ca. 25% 36x(1-0.25)=27% ASS. ca. 20% 27x(1-0.2)=22% Statine. ca % 22x(1-0.2)=17% Modifiziert nach: Arriba; arriba-hausarzt.de.")
40
Primärprävention: Vitamine Multiple Studien
WWU Münster Vitamin A (+-karotin): - Vitamin B (+Folsäure): keine Daten Vitamin C: 0 ( ) Vitamin E: 0 (HOPE, PPP, ) weitere Studien (Physician´s Health II, Su.Vi.MAX) Omenn GS et al., N Engl J Med 1996;334:1150 Study Group. N Engl J Med 1994;330:1029 Yusuf S et al., N Engl J Med 2000;342:142 Collaborative group, Lancet 2001;357:89
: - Vitamin B (+Folsäure): keine Daten. Vitamin C: 0 ( ) Vitamin E: 0 (HOPE, PPP, ) weitere Studien (Physician´s Health II, Su.Vi.MAX) Omenn GS et al., N Engl J Med 1996;334:1150 Study Group. N Engl J Med 1994;330:1029. Yusuf S et al., N Engl J Med 2000;342:142. Collaborative group, Lancet 2001;357:89.")
41
Primärprävention: ASS Metaanalyse von 4 Studien
WWU Münster US Physicians Study (1989), UK Doctors Study (1988), Thrombosis Prevention Trial (TPT, 1998), Hypertension optimal treatment (HOT, 1998) Studie Pat., mit ASS; nur HOT mit Frauen ASS mg, Beobachtungzeitraum 3,8-6,8 J Reduktion kardiovaskulärer Ereignisse um 15% Infarkte um 30% Gesamtsterblichkeit um 6% (n.s.) Anstieg von Schlaganfällen um 6% (n.s.). Koronares Risiko Nutzen/Risiko-Ratio>1,5%/J Sanmuganathan PS et al., Heart 2001;85:265
, UK Doctors Study (1988), Thrombosis Prevention Trial (TPT, 1998), Hypertension optimal treatment (HOT, 1998) Studie Pat., mit ASS; nur HOT mit Frauen. ASS mg, Beobachtungzeitraum 3,8-6,8 J. Reduktion kardiovaskulärer Ereignisse um 15% Infarkte um 30% Gesamtsterblichkeit um 6% (n.s.) Anstieg von Schlaganfällen um 6% (n.s.). Koronares Risiko Nutzen/Risiko-Ratio>1,5%/J. Sanmuganathan PS et al., Heart 2001;85:265.")
42
Primärprävention: Hypertonie Multiple Studien
WWU Münster Kleinere, zum grössten Teil ältere Studien (MAPHY, HAPPHY, Mr.FIT, IPPPS, Göteborg Trial,...) Design/Fragestellung ohne Berücksichtigung anderer RF aktuelle Studien mit Pat. mit multiplen RF (HOPE mit Ramipril) Signifikante Reduktion kardiovaskulärer Sterblichkeit und Schlaganfällen ältere Studien: Gesamtsterblichkeit idem/höher HOPE: Reduktion von KV-Tod 6,1 vs. 8,9%; MI 9, vs. 12,3%; Gesamtsterblichkeit 10,2 vs. 12,2% Yusuf S et al., N Engl J Med 2000;342:142
 Design/Fragestellung ohne Berücksichtigung anderer RF. aktuelle Studien mit Pat. mit multiplen RF (HOPE mit Ramipril) Signifikante Reduktion kardiovaskulärer Sterblichkeit und Schlaganfällen. ältere Studien: Gesamtsterblichkeit idem/höher. HOPE: Reduktion von KV-Tod 6,1 vs. 8,9%; MI 9,9 vs. 12,3%; Gesamtsterblichkeit 10,2 vs. 12,2% Yusuf S et al., N Engl J Med 2000;342:142.")
43
Statine – Allheilmittel für Herz und Hirn?
Primärprävention Gesamt-Sterblichkeit Behandlung –Kontrollarm Erreichtes LDL-C Herz Hirn WOSCOPS 140 mg/dl 3,2% 4,1% = n.a. AFCAPS 115 mg/dl 4,4% 4,6% ASCOT-LLA 80 mg/dl 3,6% 4,1%

44
Primärprävention Zusammenfassung
WWU Münster Wenn ein RF vorliegt und suboptimaler „Life Style“ Änderung „Life Style“: JA ! Medikamentöse Therapie: primär Nein ! Individuelle Risikostratifizierung (Scores) Wenn mehrere RF vorliegen (Diabetes) oder persönliches Risiko (10-)20% über 10 Jahre: Konsequente, medikamentöse Therapie
 Wenn mehrere RF vorliegen (Diabetes) oder persönliches Risiko (10-)20% über 10 Jahre: Konsequente, medikamentöse Therapie.")
45
Sekundär- (und Tertiär-) prävention
WWU Münster Sekundär- (und Tertiär-) prävention How do we treat pts with a typical ECG pattern? Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.
 prävention. How do we treat pts with a typical ECG pattern Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts. Management of asymptomatic pts is still matter of debate. According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present. (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis. (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder.")
46
Sekundärprävention: Fallvorstellung
WWU Münster 73jähriger Mann Myokardinfarkt vor 7 Jahren mit Koronarangiographie und PCI RF: Ex-Nikotin bis vor 7 Jahren, 165 cm/80 kg, RR 135/85 mmHg, GC 180, LDL 128, HDL 37 Seit 10 Tagen wieder Beklemmungsgefühl beim Ergometertraining EKG mit vorbest. Endstreckenveränderungen Belastungs-EKG bei 100 Watt nur HF 95/min Echo mit VW-Kontraktionsstörung (alt?)
")
47
Statine – Allheilmittel für Herz und Hirn?
Sekundärprävention Gesamt-Sterblichkeit Behandlung –Kontrollarm Erreichtes LDL-C Herz Hirn 4S 123 mg/dl 8,2% 11,5% n.a. MIRACL (16 Wochen) 72 mg/dl 4,2% 4,4% = PROVE-IT 62 mg/dl 2,2% 3,2%* = = * versus Pravastatin SPARCL 73 mg/dl 9,1% 8,9%
 72 mg/dl. 4,2% 4,4% = PROVE-IT. 62 mg/dl. 2,2% 3,2%* = = * versus Pravastatin. SPARCL. 73 mg/dl. 9,1% 8,9% ")
48
Sekundärprävention beta-Blocker
WWU Münster Langzeit-Beta-Blockade führt zur signifikanten Senkung des Risikos für Tod und Reinfarkt. Nutzen am größten bei selektiven ß-Blockern. Kein Nutzen bei ß-Blockern mit ISA. Meta-Analyse aller Langzeit-ß-Blocker-Studien zeigt 23% Reduktion der Gesamtsterblichkeit und 26% Reduktion des Herzinfarktes. Zu bevorzugen: Bisoprolol, Metoprolol, Carvedilol, Nebivolol

49
Sekundärprävention beta-Blocker
WWU Münster Klinische Verbesserung erst nach 3 Monaten Klinische Verbesserung Verschlechterung Klinische 1–2 3–4 5–6 7–8 9–10 11–12 Monate

50
Sekundärprävention ACE-Hemmer
WWU Münster Patienten mit stabiler KHK ohne manifeste CHF Primärer Endpunkt: % CV Mortalität, MI oder Kreislaufstillstand Years 2 4 6 8 10 12 14 1 3 5 n = Placebo Perindopril p = RRR: 20% Placebo annual event rate: 2.4%

51
Sekundärprävention Zusammenfassung
WWU Münster ACE-Hemmer ! Beta-Blocker ! ASS ! (Clopidogrel) Statin !
 Statin !")
52
Diabeteseinstellung

53
Antihypertensiva bei DM Blutdruckeinstellung !
WWU Münster Antihypertensiva bei DM Blutdruckeinstellung ! RR-Kontrolle ein Hauptziel bei Diabetes-Therapie - unabhängig von der eingesetzten Substanz ! How do we treat pts with a typical ECG pattern? Because of the reported high recurrence rate and an absence of alternative therapeutical options implantation of an ICD is the therapy of choice in symptomatic pts, Management of asymptomatic pts is still matter of debate, According to the literature implantation of an ICD seems warranted in asymptomic pts if sustained VT/VF is inducible during electrophysiological study and/or a positive family history of sudden cardiac death or syncopal attacks is present, (3) Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis, (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder, UKPDS 39. BMJ 1998;317:
 Brugada and colleagues emphasize the role of the EPS whereas Priori and coworkers did not find a positive predictive value for Inducibility regarding the pts‘ prognosis, (4) Only in pts without affected family members and not inducible during EPS it remains justified not to protect them with an icd and to follow these pts thoroughly with or without implantation of an event recorder, UKPDS 39. BMJ 1998;317:")
54
Design: randomisiert, plazebokontrolliert
Statine bei Diabetes Mellitus Collaborative Atorvastatin Diabetes Study (CARDS) WWU Münster 2.838 Patienten mit Typ 2-Diabetes Retinopathie, Albuminurie, Rauchen, oder Hypertonus aber: LDL-Cholesterin <150 Design: randomisiert, plazebokontrolliert Atorvastatin 10 mg / Plazebo Behandlungszeitraum über 6 Jahre (Abbruch nach 3,9 Jahren) Endpunkt: Akutes Koronarysndrom, Schlaganfall, Revaskularisation Primärer Endpunkt 12% auf 7% nach 4,7 Jahren Sterblichkeit gesenkt von 7% auf 5% nach 4,7 Jahren
 WWU Münster Patienten mit Typ 2-Diabetes Retinopathie, Albuminurie, Rauchen, oder Hypertonus aber: LDL-Cholesterin <150. Design: randomisiert, plazebokontrolliert. Atorvastatin 10 mg / Plazebo. Behandlungszeitraum über 6 Jahre (Abbruch nach 3,9 Jahren) Endpunkt: Akutes Koronarysndrom, Schlaganfall, Revaskularisation. Primärer Endpunkt 12% auf 7% nach 4,7 Jahren. Sterblichkeit gesenkt von 7% auf 5% nach 4,7 Jahren.")
55
Risikofaktoren und Prävention Empfehlungen der Leitlinien (I)
WWU Münster Primär Sekundär Rauchen „Aufhören“ Hypertonie <140/90 mmHg <125/80 mmHg Diabetes, Niereninsuffizienz Dyslipoprotein. GC 190 mg/dl GC 175 mg/dl LDL 115 mg/dl LDL <70 mg/dl isol. TGDiät* TG<150 mg/dl HDL>40 mg/dl ESC Task Force Report Prevention of CHD; European Heart Journal 2003; 24 (17):
:")
56
Risikofaktoren und Prävention Empfehlungen der Leitlinien (II)
WWU Münster Primär Sekundär Diabetes HbA1c <6,1 Gewicht BMI kg/m2 Aktivität 45 min, 4-5x/Woche Östrogene keine Indikation mehr Familie ggf. Familienscreening ESC Task Force Report Prevention of CHD; European Heart Journal 2003; 24 (17):
:")
57
Und die Kosten... ? WWU Münster

58
Vorlesungsfolien abrufbar:
Interner Bereich Benutzername: studi Passwort: praev09 Download Vorlesung Prävention

Ähnliche Präsentationen