Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
Neue FIGO Klassifikation des Endometrium- und Zervixkarzinoms –
worauf müssen wir in Zukunft achten? Univ. Prof. Dr. Dr. h.c. Heinz Kölbl Universitätsklinik für Geburtshilfe und Frauenkrankheiten

2
Altersgipfel 70.-80. Lebensjahr 2-4% < 45 Jahre
Endometriumkarzinom Inzidenz 18-21/ Frauen Altersgipfel Lebensjahr 2-4% < 45 Jahre 4. häufigste Malignom der Frau (Deutschland, USA) As you can see there are approximately 36 thousand new cases of uterine cancer each year in the Unites States 1 out of every 44 women in America will eventually get uterine cancer....for a lifetime incidence of 2 to 3 % This compares to a lifetime risk of about 1 of 70 for ovarian cancer and approximately 1 of 9 for breast cancer. Leitlinien 2009 Endometriumkarzinom
 As you can see there are approximately 36 thousand new cases of uterine cancer each year in the Unites States. 1 out of every 44 women in America will eventually get uterine cancer....for a lifetime incidence of 2 to 3 % This compares to a lifetime risk of about 1 of 70 for ovarian cancer. and approximately 1 of 9 for breast cancer. Leitlinien 2009 Endometriumkarzinom")
3
Atypische Hyperplasie “Unbalancierte” Östrogene
Risikofaktoren Relatives Risiko Atypische Hyperplasie 29 Adipositas >50 BMI 10 Adipositas >30 BMI 3 “Unbalancierte” Östrogene 5-10 Tamoxifen 6-7 (11 BRCA) Menopause >52 4 Diabetes 2.8 Nullipara 2-5 Menarche <12 1.6-2 PCO 3-9 -Classic risk factors that relate to the Type I Estrogen dependent Em Ca & are shown here -Obesity causes peripherial Estrone production and also may cause an anovulatory state in the pre-menopausal patient who develops endometrial cancer -Note the effect of exogenous estrogen which increases the relative risk of endometrial cancer from 5 to 14 fold depending on the number of years of use. It is worth mentioning that these cases tend to be well differentiated and as a result they have a better prognosis than matched cases in which no exogenous estrogen was used. -Atypical hyperplasia is clearly a precursor lesion for EM Ca and it is the cellular Atypia which is the key as we will discuss shortly -Note the protective effect of OCP which are felt to prevent about 2000 cases of Em Ca in the US each year
 Menopause > Diabetes Nullipara Menarche < PCO Classic risk factors that relate to the Type I Estrogen dependent Em Ca & are shown here. -Obesity causes peripherial Estrone production and also may cause an anovulatory state in the pre-menopausal patient who develops endometrial cancer. -Note the effect of exogenous estrogen which increases the relative risk of endometrial cancer from 5 to 14 fold depending on the number of years of use. It is worth mentioning that these cases tend to be well differentiated and as a result they have a better prognosis than matched cases in which no exogenous estrogen was used. -Atypical hyperplasia is clearly a precursor lesion for EM Ca and it is the cellular Atypia which is the key as we will discuss shortly. -Note the protective effect of OCP which are felt to prevent about 2000 cases of Em Ca in the US each year.")
4
Typ I Typ II (~10%) Endometriumkarzinom
Anhaltende hohe Östrogenexposition Entstehung über Hyperplasien gute Differenzierung, diploid, Rez. pos Adipositas, Nulliparität Typ II (~10%) Atrophisches Endometrium ungünstige histologische Typen, aneuploid. Rez neg Multiparität, Normalgewicht Among the endometrial carcinomas, it has become more common to distinguish between the type I vs type II tumors. -The majority will fall into Type I- the classic Estrogen related cancer. E, younger, low grade, endometroid -Type II refers to those tumors which appear unrelated to estrogen- generally the high grade tumors and poor prognosis histologies in women without classic risk factors. -A third category of tumors are being recognized the genetic/familial cases like HNPCC (a defect in MSH mismatch repair genes) 40X risk of EM ca (5X Ov) pts as young as 16y/o
 Atrophisches Endometrium. ungünstige histologische Typen, aneuploid. Rez neg. Multiparität, Normalgewicht. Among the endometrial carcinomas, it has become more common to distinguish between the type I vs type II tumors. -The majority will fall into Type I- the classic Estrogen related cancer. E, younger, low grade, endometroid. -Type II refers to those tumors which appear unrelated to estrogen- generally the high grade tumors and poor prognosis histologies in women without classic risk factors. -A third category of tumors are being recognized the genetic/familial cases like HNPCC (a defect in MSH mismatch repair genes) 40X risk of EM ca (5X Ov) pts as young as 16y/o.")
5
Lynch II Syndrome: HNPCC (Hereditary Non-Polyposis Colon Cancer)
Autosomal dominant MMR (mismatch repair) Mutation Genetische Instabilität Fehler DNA-Replication hMSH2 (chrom 2) hMLH1 (chrom 3) Frühes Kolon-Ca: mittlere Alter 45.2 Jahre Endometrium-Ca: 2. häufigstes Malignom 40-60% Lebenszeitrisiko andere Malignome: Ovar (12%), Magen, Dünndarm, Pankreas, Gallenblase 2-9% aller Patientinnen mit Endometriums-Ca Other genetic mutations of interest in endometrial carcinoma are the mutations in mismatch repair genes- In these patients genetic instability leads to error-prone DNA replication. This leads to a cancer syndrome known as Lynch II which is characterized by the following: Early age of colon Ca with an average age of 45. Endometrial Ca is the second most common malignancy with a 20% cumulative incidence by age 70 Earlier age of onset than sporadic cases Other adenocarcinomas are common as well: ovary (3.5-8 fold), stomach, small bowel, pancreas, biliary tract.
 Mutation. Genetische Instabilität Fehler DNA-Replication. hMSH2 (chrom 2) hMLH1 (chrom 3) Frühes Kolon-Ca: mittlere Alter 45.2 Jahre. Endometrium-Ca: 2. häufigstes Malignom % Lebenszeitrisiko. andere Malignome: Ovar (12%), Magen, Dünndarm, Pankreas, Gallenblase. 2-9% aller Patientinnen mit Endometriums-Ca. Other genetic mutations of interest in endometrial carcinoma are the mutations in mismatch repair genes- In these patients genetic instability leads to error-prone DNA replication. This leads to a cancer syndrome known as Lynch II which is characterized by the following: Early age of colon Ca with an average age of 45. Endometrial Ca is the second most common malignancy with a. 20% cumulative incidence by age 70. Earlier age of onset than sporadic cases. Other adenocarcinomas are common as well: ovary (3.5-8 fold), stomach, small bowel, pancreas, biliary tract.")
6
Endometriumkarzinom – Histologie
Typ I Gute Prognose Endometrioid (87%) Adenosquamös (4%) Muzinös (1%) Typ II Schlechte Prognose Serös-papillär (3%) Clear Cell (2%) Undifferenziert (<2%) Squamös (sehr selten) -The vast majority of uterine cancers are carcinomas with most of those being endometrioid or adenosquamous histology -These histologies carry a relatively good prognosis. -about 5% of the carcinomas will be poor prognosis histologies like UPSC or clear cell carcinomas which spread in a more aggressively -The sarcomas also tend to carry a poor prognosis, an they comprise about 6% of uterine corpus CA in the US, but are about 2X as common in black women as compared to whites. As a result the prevalence ratio in at Downstate is roughly 85/15 carcinoma to sarcoma.
 Adenosquamös (4%) Muzinös (1%) Typ II Schlechte Prognose. Serös-papillär (3%) Clear Cell (2%) Undifferenziert (<2%) Squamös (sehr selten) -The vast majority of uterine cancers are carcinomas with most of those being endometrioid or adenosquamous histology. -These histologies carry a relatively good prognosis. -about 5% of the carcinomas will be poor prognosis histologies like UPSC or clear cell carcinomas which spread in a more aggressively. -The sarcomas also tend to carry a poor prognosis, an they comprise about 6% of uterine corpus CA in the US, but are about 2X as common in black women as compared to whites. As a result the prevalence ratio in at Downstate is roughly 85/15 carcinoma to sarcoma.")
7
Endometriumkarzinom - Symptomatik
> 95% der Patientinnen haben Symptome Postmenopausenblutung Menorrhagie, Metrorrhagie bis 20% auffällige EM-Zellen in Cervix-Zyto Symptomlose Pat. + EM-Zellen Sonographisches Screening Spezifität ohne HRT 60-92% PPV % EM-Dicke mm More than 95% of patients with Em cancer will report symptoms. Most commonly PMB, or in premenapausal women changes related to the quantity or duration of flow or to intermentrual bleeding. Endometrial biopsy is the main diagnostic tool either in the office or via D&C in the OR.

8
Postmenopausenblutung – Diagnostik
präoperativ gynäkologische Untersuchung transvaginale Sonographie Genitale ohne HRT EM > 10mm suspekt (AGO Leitlinie) Fraktionierte Abrasio Hysteroskopie (nicht obligat bei klinisch eindeutigem Karzinom) 80% Sensitivität, PPV ~ 80% keine sichere Diagnose Cervixinvasion More than 95% of patients with Em cancer will report symptoms. Most commonly PMB, or in premenapausal women changes related to the quantity or duration of flow or to intermentrual bleeding. Endometrial biopsy is the main diagnostic tool either in the office or via D&C in the OR.
 Fraktionierte Abrasio. Hysteroskopie (nicht obligat bei klinisch eindeutigem Karzinom) 80% Sensitivität, PPV ~ 80% keine sichere Diagnose Cervixinvasion. More than 95% of patients with Em cancer will report symptoms. Most commonly PMB, or in premenapausal women changes related to the quantity or duration of flow or to intermentrual bleeding. Endometrial biopsy is the main diagnostic tool either in the office or via D&C in the OR.")
9
Postmenopausenblutung
Risiko Corpusmalignom Alter Anzahl Malignom % <50 34 0.0 50-59 161 15 9.3 60-69 92 16.3 70-79 43 12 27.9 >80 5 3 60.0 While the overall incidence of cancer is 15% in this population, this will vary greatly according to the age of the patient. Most of our patients with this complaint will fall in the year old range and for them the chances of a cancer diagnosis will be in that 10-15% range. For our patients <50 we are still going to do a biopsy, but the chances are much less that their bleeding is from cancer and much more likely to be due to hormonal fluctuations of the perimenapause or a benign functional cause such as a polyp or fibroid. For the more elderly those >70 y/o the chances are obviously much greater that a cancer is present Hawwa et al., 1970

10
Endometriumshyperplasie
Spontaner Verlauf Typ Anzahl (n=170) Follow up Jahre) Anzahl Progress zum EM-Ca. % Progress zum EM-Ca % Persistenz % Regression Einfach 93 15.2 1 1% 19% 80% Komplex 29 13.5 3% 17% Atypie, einfach 13 11.4 8% 23% 69% Atypie, komplex 35 10 29% 14% 57% It is atypia that is the defining feature of the premalignant endometrial lesion. This classic paper by Kurman looked retrospectively at 150 patients with who had an initial diagnosis of endometrial hyperplasia between the years 1940 and The patients were not treated and had follow-up biopsy for only for symptomatic bleeding. 96 of the patients had at least one additional biopsy. It is from this paper that we know of the 1, 3, 8 and 29% progression rate that everyone memorizes for the CREOGs and board exams. Kurman and his colleagues then pooled these patients into two groups: one with atypia and the other without atypia. They concluded that the group without atypia has no greater risk of developing uterine cancer over 13 years than would be expected from the 2-3% lifetime risk that all women have. Kurman, et al. Cancer 1985
 Follow up. Jahre) Anzahl Progress zum. EM-Ca. % Progress zum. EM-Ca. % Persistenz. % Regression. Einfach % 19% 80% Komplex % 17% Atypie, einfach % 23% 69% Atypie, komplex % 14% 57% It is atypia that is the defining feature of the premalignant endometrial lesion. This classic paper by Kurman looked retrospectively at 150 patients with who had an initial diagnosis of endometrial hyperplasia between the years 1940 and The patients were not treated and had follow-up biopsy for only for symptomatic bleeding. 96 of the patients had at least one additional biopsy. It is from this paper that we know of the 1, 3, 8 and 29% progression rate that everyone memorizes for the CREOGs and board exams. Kurman and his colleagues then pooled these patients into two groups: one with atypia and the other without atypia. They concluded that the group without atypia has no greater risk of developing uterine cancer over 13 years than would be expected from the 2-3% lifetime risk that all women have. Kurman, et al. Cancer")
11
Endometriumshyperplasie - Behandlung
Hyperplasie ohne Atypien Prämenopausal/Kinderwunsch Zyklische Gestagene Zyklustag z.B MPA 60-80% Regression Nach 3-6 Monaten Kontrollabrasio Postmenopausal Hysterektomie evtl. Adnexektomie/Kontrollen Ursache ?? (HRT, Tumor, Adipositas) It is atypia that is the defining feature of the premalignant endometrial lesion. This classic paper by Kurman looked retrospectively at 150 patients with who had an initial diagnosis of endometrial hyperplasia between the years 1940 and The patients were not treated and had follow-up biopsy for only for symptomatic bleeding. 96 of the patients had at least one additional biopsy. It is from this paper that we know of the 1, 3, 8 and 29% progression rate that everyone memorizes for the CREOGs and board exams. Kurman and his colleagues then pooled these patients into two groups: one with atypia and the other without atypia. They concluded that the group without atypia has no greater risk of developing uterine cancer over 13 years than would be expected from the 2-3% lifetime risk that all women have.
 It is atypia that is the defining feature of the premalignant endometrial lesion. This classic paper by Kurman looked retrospectively at 150 patients with who had an initial diagnosis of endometrial hyperplasia between the years 1940 and The patients were not treated and had follow-up biopsy for only for symptomatic bleeding. 96 of the patients had at least one additional biopsy. It is from this paper that we know of the 1, 3, 8 and 29% progression rate that everyone memorizes for the CREOGs and board exams. Kurman and his colleagues then pooled these patients into two groups: one with atypia and the other without atypia. They concluded that the group without atypia has no greater risk of developing uterine cancer over 13 years than would be expected from the 2-3% lifetime risk that all women have.")
12
Endometriumshyperplasie - Behandlung
Hyperplasie mit Atypien Prämenopausal/Kinderwunsch hoch dosierte Gestagene 100mg MPA Mirena Nach 3 und 9 Monaten Kontrollabrasio, Postmenopausal/kein Kinderwunsch Hysterektomie evtl. mit Adnexektomie cave: simultanes Endometriumskarzinom Komplexe Hyperplasie mit Atypien im Abradat bis 20-40% EM-CA Adnexektomie erwägen It is atypia that is the defining feature of the premalignant endometrial lesion. This classic paper by Kurman looked retrospectively at 150 patients with who had an initial diagnosis of endometrial hyperplasia between the years 1940 and The patients were not treated and had follow-up biopsy for only for symptomatic bleeding. 96 of the patients had at least one additional biopsy. It is from this paper that we know of the 1, 3, 8 and 29% progression rate that everyone memorizes for the CREOGs and board exams. Kurman and his colleagues then pooled these patients into two groups: one with atypia and the other without atypia. They concluded that the group without atypia has no greater risk of developing uterine cancer over 13 years than would be expected from the 2-3% lifetime risk that all women have.

13
Endometriumkarzinom - FIGO Stadien
Stadium I (73%) begrenzt auf Corpus uteri Stadium II (11%) Cervix betroffen Stadium III (13%) A: Serosa oder Adnexe (a) B: Vaginalmetastasen, parametrane Beteiligung C1: pelv. LK-Metastasen C2: paraaortale LK-Metastasen Stadium IV (3%) A: Blase, Darm, B: inguinale LK-Metastasen, intraabd. und Fernmetastasen This summarizes the frequency with which each stage of endometrial cancer is encountered. Approximately 85% will be locally confined within the uterus and cervix leading to the overall good prognosis of this disease
 begrenzt auf Corpus uteri. Stadium II. (11%) Cervix betroffen. Stadium III. (13%) A: Serosa oder Adnexe (a) B: Vaginalmetastasen, parametrane Beteiligung. C1: pelv. LK-Metastasen. C2: paraaortale LK-Metastasen. Stadium IV. (3%) A: Blase, Darm, B: inguinale LK-Metastasen, intraabd. und Fernmetastasen. This summarizes the frequency with which each stage of endometrial cancer is encountered. Approximately 85% will be locally confined within the uterus and cervix leading to the overall good prognosis of this disease.")
14
Endometriumkarzinom – Prognose
5-Jahresüberleben Stadium % IA 91 IB 88 IC 81 IIA 77 IIB 67 IIIA 60 IIIB 41 IIIC 32 IVA 20 IVB 5 Mittleres Überleben 84% 5-Jahresüberleben Grade % 1 92 2 87 3 74 Prognosis for endometrial cancer is generally good, owing to the early stage at presentation of most patients the overall 5 yr survival for all grades, stages and histologies is 84% Stage of disease is by far the most important predictor of survival, followed by grade.

15
Endometriumkarzinom – Staging
präoperativ Rö-Thorax Sonographie Leber, Nieren, Genitale evtl. CA 125 Evtl. Zystokopie, Rektoskopie (Ausschluß Figo IVa) Nutzen CT, MRT, PET nicht erwiesen Operatives Staging Exploration Abdomen Hysterektomie/Adnexektomie Lymphonodektomie More than 95% of patients with Em cancer will report symptoms. Most commonly PMB, or in premenapausal women changes related to the quantity or duration of flow or to intermentrual bleeding. Endometrial biopsy is the main diagnostic tool either in the office or via D&C in the OR.
 Nutzen CT, MRT, PET nicht erwiesen. Operatives Staging Exploration Abdomen. Hysterektomie/Adnexektomie. Lymphonodektomie. More than 95% of patients with Em cancer will report symptoms. Most commonly PMB, or in premenapausal women changes related to the quantity or duration of flow or to intermentrual bleeding. Endometrial biopsy is the main diagnostic tool either in the office or via D&C in the OR.")
16
Endometriumkarzinom – Chirurg. Staging
klinisches Stadium I 30% “upstaged” durch Operation 5% Ovarialbefall 6% para-aortale LK 1/3 ohne pelvine LK 9% pelvine LK klinisches Stadium II/III 60% “upstaged” durch Operation Surgical staging replaced clinical staging in 1989 and has since proved more reliable, more accurate for prognosis and more useful for defining the need for adjuvant therapy than clinical staging. This is primarily because surgical staging more accurately defines the extent of a patient’s disease with respect to metastases, depth of invasion, cervical involvement, etc.

17
Chirurgisches Staging
Endometriumkarzinom Chirurgisches Staging Klinische Einschätzung N 5-yr OS (%) Stadium I 245 88 Stadium II/III 47 83 Chirurgische Einschätzung Stadium I/II 231 93 Stadium III 61 67 Surgical staging replaced clinical staging in 1989 and has since proved more reliable, more accurate for prognosis and more useful for defining the need for adjuvant therapy than clinical staging. This is primarily because surgical staging more accurately defines the extent of a patient’s disease with respect to metastases, depth of invasion, cervical involvement, etc. Lanciano et al: Radiother Oncol 28:189,1993
 Stadium I Stadium II/III Chirurgische Einschätzung. Stadium I/II Stadium III Surgical staging replaced clinical staging in 1989 and has since proved more reliable, more accurate for prognosis and more useful for defining the need for adjuvant therapy than clinical staging. This is primarily because surgical staging more accurately defines the extent of a patient’s disease with respect to metastases, depth of invasion, cervical involvement, etc. Lanciano et al: Radiother Oncol 28:189,1993.")
18
} Endometriumkarzinom Operatives Vorgehen: Stadium Ia*,b G1*,2*, 3 II
Spülzytologie Hysterektomie Adnexektomie bds. Pelv. u paraaortale Lymphonodektomie (*fakultativ) + rad. Hysterektomie + Omentektomie +Tumordebulking II IIIA-C
 + rad. Hysterektomie. + Omentektomie. +Tumordebulking. II. IIIA-C.")
19
Endometriumkarzinom Stadium III B (vaginaler Befall) zusätzlich partielle/totale Kolpektomie Stadium IVA vordere/hintere totale Exenteration Stadium M1 (FIGO IV B) evtl. Tumor-Debulking, HE Seröse und klarzellige Karzinome Omentektomie, Per.-Pe‘s Debulking
 evtl. Tumor-Debulking, HE. Seröse und klarzellige Karzinome. Omentektomie, Per.-Pe‘s. Debulking.")
20
Laparoskopische Operation
5 prospektiv/rand. Studien Laparoskopie N=253, Laparotomie N=245 OFS, DFS, Rezidivraten ohne signifikanten Unterschied Op-Zeiten Blutverlust Postoperative Komplikationen AGO/Leitlinie: Laparoskopische Lymphonodektomie plus LVAH scheint ähnlich sicher

21
Endometriumkarzinom – LK-Metastasen
Situation % positive LK G1, inneres 1/3 Myometrium kein extrauteriner Tumor <1% G2 or G3, inneres 1/3 Invasion, kein extrauteriner Tumor 5-9% pelvin 4% aortal G3 äußeres 1/3 Invasion oder extrauteriner Tumor 20-60% pelvin 10-30% aortal -While the grade of the tumor may be known in advance of surgery, the depth of invasion cannot be accurately known until the uterus is removed. -Because of the very low rate of lymph node metastases in patients with G1 tumors who have no or superficial myometrial invasion, LNS is not necessary and the risk from the procedure may outweigh the benefits -LNS is currently advocated by most oncologists in all other circumstances although some controversy exists with respect to small non invasive or minimally invasive G2 tumors

22
Lymphknotenmetastasen
Keine Vorhersage durch Ultraschall, CT oder MRT Inspektion/Palpation Sampling von ”verdächtigen” LK Nur 10 % befallener LK vergrößert Lokalisation 10-30% nur paraaortal pos. LK wenn pos pelvine LK 2/3 auch pos paraaortale LK

23
Lymphonodektomie bei Endometriumkarzinom
ASTEC-Study Group, The Lancet 2009 Benedetti Panici P, J Natl Canc Inst 2008

24
ASTEC-Study Group: Gesamtüberleben

25
SENTINEL-LNE beim Endometriumkarzinom ?
Detektionsrate 86% 1,9 – 3 SNL Knoten/Pat Geringe Korrelation zwischen praeop. Szintigraphie und intraop. Detektion Ersetzt LNE nicht Ballester Gynecol Oncol 2009; 112:348-52 Abu-Rustum Gynecol Oncol 2009; 113:163-9

26
25% aller Fälle Endometriumkarzinom - Rezidiv Lokalisation %
Fernmetastasen 51 Kleines Becken 32 Vagina 17 70-90% innerhalb von 2 Jahren 60-70% symptomatisch Vaginalzytologie <1% benefit In patients who receive post operative pelvic radiation, most recurrences will be out of the pelvis- distant lymph nodes or in the lungs In patients who have not received radiation, pelvic and vaginal recurrences are much more likely, comprising more than half of the cases

27
Endometriumkarzinom – Adjuvante Radiatio
pN0 FIGO Ia G1/2, IB G1 keine Radiatio Ia G3, Ib G2/3 Brachytherapie pT2 pT3, pT4 Teletherapie ± Brachytherapie Linearbeschleuniger (15MV Photonen) HDR Afterloading
 HDR Afterloading.")
28
Endometriumkarzinom – Adjuvante Radiatio
pN+ FIGO IIIC1 / Brachytherapie / pelvine Teletherapie FIGOIIIC2 Brachytherapie / pelvine + paraaortale Region Serös-papilläre Ca´s Chemotherapie (Tax/Carbo)
")
29
Endometriumkarzinom – Primäre Radiatio
nur bei primär inoperablen Patientinnen Teletherapie ± Brachytherapie

30
Statements - Chemotherapie
bei optimal operierten Patientinnen mit Stadium III oder IV ist die adjuvante Chemotherapie (Adriamycin plus Cisplatin) einer Strahlentherapie (Abdomenganzbestrahlung + pelvinem ± paraaortalem Boost) signifikant überlegen (LOE: 1b, GR: B) im Stadien II, G3 und III ist die adjuvante Chemotherapie eine sinnvolle Alternative zur Strahlentherapie
 einer Strahlentherapie (Abdomenganzbestrahlung + pelvinem ± paraaortalem Boost) signifikant überlegen (LOE: 1b, GR: B) im Stadien II, G3 und III ist die adjuvante Chemotherapie eine sinnvolle Alternative zur Strahlentherapie.")
31
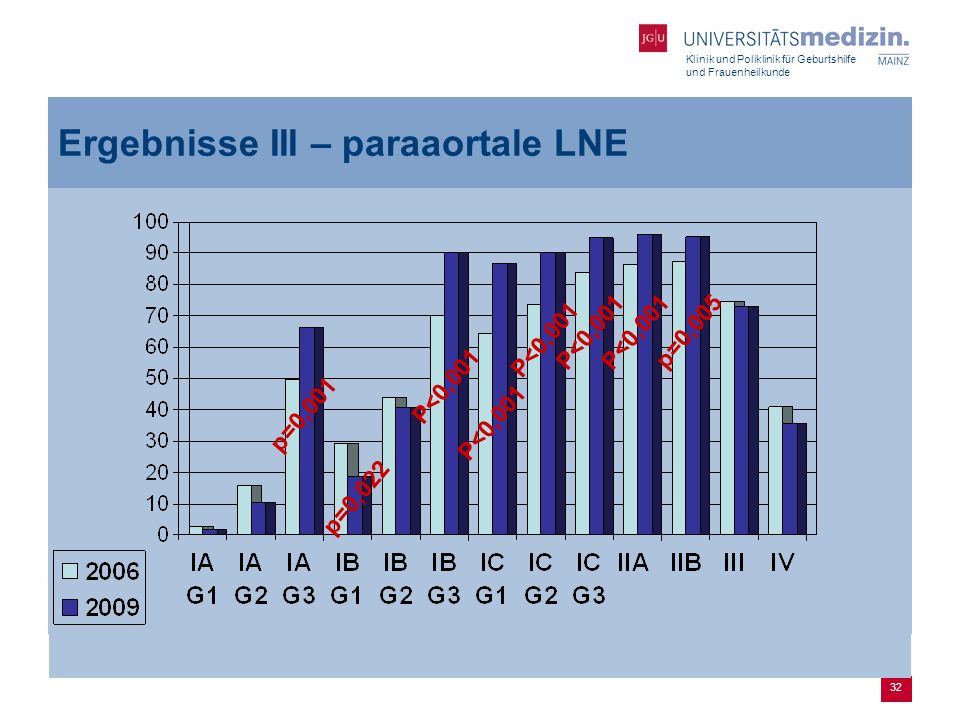
Fragestellungen Wird das Endometriumkarzinom in Deutschland leitliniengerecht therapiert? Verändert sich die Versorgung des Endometriumkarzinoms seit der Etablierung der S2-Leitlinie im Jahr 2006 und deren Aktualisierung im Jahr 2009? Leitlinienadresse: www-dggg.de 31 31

32
Ergebnisse III – paraaortale LNE
32 32
33
Zusammenfassung Endometriumkarzinom
4 häufigstes Malignom der Frau Kardinalsymptom: Blutung (Postmenopause) Überwiegend in frühen Stadien diagnostiziert mit guter Prognose Operative Therapie ist die Domäne in der Behandlung Lymphknoten-Staging für die Ausrichtung der adjuvanten Therapie erforderlich Bestrahlung senkt Inzidenz an Lokalrezidiven Chemotherapie dzt. noch untergeordnete Rolle – Studien!!!
 Überwiegend in frühen Stadien diagnostiziert mit guter Prognose. Operative Therapie ist die Domäne in der Behandlung. Lymphknoten-Staging für die Ausrichtung der adjuvanten Therapie erforderlich. Bestrahlung senkt Inzidenz an Lokalrezidiven. Chemotherapie dzt. noch untergeordnete Rolle – Studien!!!")
34
Staging und Therapie des
Zervixkarzinoms D. Böhm Klinik und Poliklinik für Geburtshilfe und Frauenheilkunde

35
Epidemiologie Zervixkarzinom
2006 (D): 5470 Neuerkrankungen 5-Jahres Überlebensraten beim invasiven Zervixkarzinomen liegen in Deutschland zwischen 63 und 71 % Inzidenz: 3,6 (Finnland) und 45 (Kolumbien) pro Frauen/Jahr Inzidenz in D: 14,1/ Frauen (rückläufig) Inzidenz hochgradiger Präkanzerosen 100x (1%, vervierfacht in den letzten Jahren)
: 5470 Neuerkrankungen. 5-Jahres Überlebensraten beim invasiven Zervixkarzinomen liegen in Deutschland zwischen 63 und 71 % Inzidenz: 3,6 (Finnland) und 45 (Kolumbien) pro Frauen/Jahr. Inzidenz in D: 14,1/ Frauen (rückläufig) Inzidenz hochgradiger Präkanzerosen 100x (1%, vervierfacht in den letzten Jahren)")
36
Zervixkarzinom und Vorstufen

37
Neuerkrankungs- und Sterberate in Deutschland 1980-2006
Krebs in Deutschland 2005/2006: Häufigkeiten und Trends, Krebsregister in Deutschland e.V., 7. Ausgabe, 2010

38
Diagnostik Leitsymptom: Kontaktblutung, Ausfluss
Staging nach FIGO erfolgt in Form einer klinischen Untersuchung Spekulumeinstellung zur Beurteilung der Ausdehnung des Tumors zur Scheide bimanuelle vaginale und rektovaginale Untersuchung Histologie durch gezielte Biopsie oder Kürettage

39
Bildgebende Diagnostik
Ultraschall der Nieren Rö-Thorax ggf. Zysto/Rektoskopie MRT-Becken ab FIGO IB2 empfohlen Ggf. Palpation/Ultraschall Scalenus-Region (Lymphknoten)
")
40
MRT präoperativ? ab Stadium IB2 MRT-Diagnostik in Ergänzung zur Tastuntersuchung empfohlen bessere Bestimmung von: Größe des Tumors Infiltrationstiefe Beziehung zu den Nachbarorganen CAVE: Lymphknotenstatus nicht sicher beurteilbar Sensitivität Tumorgröße 100 % Sensitivität LK 73 % , Spezifität LK 93 % Bedeutung PET derzeit unklar op. LK-Staging per LSK möglich

41
Prätherapeutisches Staging
prätherapeutische Stadieneinteilung entsprechend der FIGO-Klassifikation des Zervixkarzinoms ist von der klinischen Erfahrung des Untersuchers abhängig Ziel: Einschränkung der Radikalität operativer Maßnahmen Studie: Vergleich der klinischen Untersuchung vs. Histopathologischem Ergebnis N = 1092 Pateinten mit Zervix-Ca FIGO I+II Überbewertung durch klinische Untersuchung 23% Korrektes klinisches Stadium 61% Unterbewertung durch klinische Untersuchung 16% Baltzer J (1991) Management of cervix cancer – yes or no to postoperative radiation treatment after Wertheim operation? Zentralbl Gynakol 113:661–665
 Management of cervix cancer – yes or no to postoperative radiation treatment after Wertheim operation Zentralbl Gynakol 113:661–665.")
42
Neue FIGO-Klassifikation: 01.01.2010
neue FIGO-Klassifikation verbindlich seit 1. Januar 2010 Stadieneinteilung weiterhin klinisch Stadium 0 entfällt, Carcinoma in situ zählt zu CIN III Aktuelle Stadieneinteilung nicht in derzeit gültiger S2K-Leitlinie enthalten

43
Neue FIGO-Klassifikation: 01.01.2010
Stadium I: unverändert Stadium II: TU infiltriert außerhalb des Uterus (BW nicht erreicht, unteres Vaginaldrittel frei) Stadium IIA1: Parametrien frei, TU ≤ 4 cm Stadium IIA2: Parametrien frei, TU > 4 cm Stadium IIB: unverändert Stadium III: unverändert Stadium IV: unverändert
 Stadium IIA1: Parametrien frei, TU ≤ 4 cm. Stadium IIA2: Parametrien frei, TU > 4 cm. Stadium IIB: unverändert. Stadium III: unverändert. Stadium IV: unverändert.")
44
Stadienverteilung nach FIGO
% N IA1 + IA2 15% 800 IB 38% 2100 IIA 8% 440 IIB 18% 990 III IV 7% 380 Tumormanual Zervixkarzinom TUZ München 2010 (n=1248)
")
45
Operatives Staging Laparoskopie zur Bestimmung der lokoregionären Tumorausdehnung bei unklarer Ausdehnung: Abklärung einer Tumorinfiltration von Harnblasen- und Rektumwand Ausschluss bzw. Bestätigung von paraaortalen und/oder pelvinen Lymphknotenmetastasen Ergebnisse finden für die Stadieneinteilung bis heute noch keine Berücksichtigung in Leitlinie Laparoskop. Staging: kurze Liegedauer, wenig Komplikationen, rascherer Beginn adj. Therapiemaßnahmen

46
Grundlagen der Therapie
in Frühstadien und bei prämenopausalen Patientinnen wird die Operation empfohlen mit dem Ziel: R0 Resektion Grenze der Operabilität: unsichere Stadieneinteilung durch klinische Untersuchung (FIGO IIb) Operation und primäre Radiochemotherapie führen in den Stadien Ib und IIa zu gleichwertigen Langzeitergebnissen bei unterschiedlichen Rezidivmuster und Nebenwirkungsprofil Landoni F, et al, Lancet 1997 FIGO III: Indikation zur primären Radiochemotherapie
 Operation und primäre Radiochemotherapie führen in den Stadien Ib und IIa zu gleichwertigen Langzeitergebnissen bei unterschiedlichen Rezidivmuster und Nebenwirkungsprofil. Landoni F, et al, Lancet FIGO III: Indikation zur primären Radiochemotherapie.")
47
Möglichkeiten der Operative Therapie: FIGO I-II
Konisation Trachelektomie Radikale Hysterektomie mit pelviner/paraaortaler LNE (Wertheim-Meigs) Vaginal Abdominal Laparoskopisch Roboter-assistiert Exenteration
 Vaginal. Abdominal. Laparoskopisch. Roboter-assistiert. Exenteration.")
48
Vor- und Nachteile der OP
Vorteile Eierstöcke bleiben erhalten keine Strahlenfolgen: Enteritis, Kolitis, Vaginalstenose, Strahlenzystitis Operatives Staging Nachteile Blasenentleerungsstörungen Rektumentleerungsstörungen Lymphödeme der Beine Blasen-Scheiden-Fistel Verkürzung der Scheide

49
Stadienadaptiertes Vorgehen: IA1
IA1: (Invasionstiefe <3 mm, Oberflächenausdehnung <7 mm) Pelviner LK-Befall: 2% fertilitätserhaltend: Konisation Einfache Hysterektomie IA1 + Risikofaktoren (L1,V1, G3) fertilitätserhaltend: Konisation, Trachelektomie + pelvine LNE Oder: einfache Hysterektomie + pelvine LNE
 Pelviner LK-Befall: 2% fertilitätserhaltend: Konisation. Einfache Hysterektomie. IA1 + Risikofaktoren (L1,V1, G3) fertilitätserhaltend: Konisation, Trachelektomie + pelvine LNE. Oder: einfache Hysterektomie + pelvine LNE.")
50
FIGO IA2 und IB1 IA2 (Invasionstiefe 3-7 mm, Ober-flächenausdehnung <7 mm) IB1: < 4 cm Pos. Lymphknoten: >10% Radikale HE mit pelviner LNE ggf. paraaortale LNE bei pos. LK’s ggf. bei Kinderwunsch: radikale Trachelektomie mit pelviner LNE (< 2cm) IB1 Klinisch sichtbare Läsion ≤ 4 cm in der größten Ausdehnung
 IB1. Klinisch sichtbare Läsion ≤ 4 cm in der größten Ausdehnung.")
51
Trachelektomie Milliken DA, Shepherd JH. Fertility preserving surgery for carcinoma of the cervix. Curr Opin Oncol Sep;20(5):
:")
52
FIGO IB2 - IIB Radikale HE mit pelviner und paraortaler LNE bis kaudal A. mesenterica inf. Bei pos. LK’s paraaortal bis Nierenstiel Bei Befall hoher paraaortaler LK’s Abbruch der OP Risiko der Radio-Chemotherapie postoperativ Addition der Komplikationen Ggf. Resektion größerer LK-Metastasen

53
Radikale Hysterektomie + LNE (Wertheim-Meigs)
stadienabhängig in Anlehnung an Wertheim, Meigs und Okabayashi durchgeführt pelvine Lymphonodektomie (mind. 20) ggf. paraaortale Lymphonodektomie (mind. 10) Terminologie der Radikalität: Piver (1974) Radikale Hysterektomie Absetzen der Parametrien stadienabhängig mit ausreichenden Sicherheitsabstand zum Tumor Absetzen von Parakolpium und Vagina mit ausreichendem vaginalen Sicherheitsabstand PIVER I: Totale extrafasziale Hysterektomie PIVER II: Modifiziert radikale Hysterektomie mit Resektion von Parametrium und parazervikalem Gewebe medial des Ureters PIVER III: Resektion des Parametriums bis zur Becken-wand, lange Scheidenmanschette, totale Mobilisierung des Ureters PIVER IV: zusätzlich längere Scheidenmanschette und Resektion der A.ves. sup. PIVER V: zusätzlich partielle Resektion des distalen Ureters oder der Blase
 ggf. paraaortale Lymphonodektomie (mind. 10) Terminologie der Radikalität: Piver (1974) Radikale Hysterektomie. Absetzen der Parametrien stadienabhängig mit ausreichenden Sicherheitsabstand zum Tumor. Absetzen von Parakolpium und Vagina mit ausreichendem vaginalen Sicherheitsabstand. PIVER I: Totale extrafasziale Hysterektomie. PIVER II: Modifiziert radikale Hysterektomie mit Resektion von Parametrium und parazervikalem Gewebe medial des Ureters. PIVER III: Resektion des Parametriums bis zur Becken-wand, lange Scheidenmanschette, totale Mobilisierung des Ureters. PIVER IV: zusätzlich längere Scheidenmanschette und Resektion der A.ves. sup. PIVER V: zusätzlich partielle Resektion des distalen Ureters oder der Blase.")
54
Ist eine Radio-Chemotherapie gleichwertig?
Prospektiv-randomisierte Studie FIGO IB – IIA 170 Frauen operiert: PIVER III 167 Frauen radiotherapiert Nachbeobachtungszeit 87 Monate 118/170 (68,7%) der primär operierten Frauen bekamen zusätzlich Radiotherapie bei Risikofaktoren (Stadium IIB, < 3mm freier Resektionsrand, R1, LN+) Landoni F et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet 1997:350:535 – 40 Overall actuarial survival by treatment group and cervical diameter.
 der primär operierten Frauen bekamen zusätzlich Radiotherapie bei Risikofaktoren (Stadium IIB, < 3mm freier Resektionsrand, R1, LN+) Landoni F et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet 1997:350:535 – 40. Overall actuarial survival by treatment group and cervical diameter.")
55
Ist eine Radio-Chemotherapie gleichwertig?
Landoni F et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet 1997:350:535 – 40 Overall and disease-free actuarial survival by treatment group

56
Fortgeschrittenes Zervixkarzinom
FIGO III: Ausbreitung bis Beckenwand, Befall des distalen Vaginaldrittels; Hydronephrose, stumme Niere. Primäre Radio-Chemotherapie FIGO IV: Ausbreitung über das kleine Becken hinaus oder Befall der Blase/Rektum Exenteration +/- adjuvante RCTX (individuelle Entscheidung)
")
57
Sentinel-LNE beim Zervixkarzinom
< 20mm: 249 Pat. vs. > 20mm: 305 Pat. Detektionsrate: Tumoren < 20mm: 94% (signifikant) Tumoren > 20mm: 83,6% NPV signifikant verbessert bei Tumoren < 20mm (99,1% vs. 88,5%) Sensitivität bei Tumoren < 20mm verbessert, (90,9% vs. 72,7%, ns.) Bisher keine Leitlinienempfehlung Multicenter Validation Study of the Sentinel Lymph Node Concept in Cervical Cancer: AGO Study Group. Altgassen et al. JCO 26:
 Tumoren > 20mm: 83,6% NPV signifikant verbessert bei Tumoren. < 20mm (99,1% vs. 88,5%) Sensitivität bei Tumoren < 20mm verbessert, (90,9% vs. 72,7%, ns.) Bisher keine Leitlinienempfehlung. Multicenter Validation Study of the Sentinel Lymph Node Concept in Cervical Cancer: AGO Study Group. Altgassen et al. JCO 26:")
58
Laparoskopie Operative Therapie: Tumor< 4 cm, L0, G1/G2
LRH + lsk. LNE Tumor< 4 cm, L0, G1/G2 schnelle Rekonvaleszenz Nervenschonend Kosmetik Erfahrung des Operateurs hohe Lernkurve Roboter-assistiert (Da Vinci®)
")
59
Adjuvante Radiatio eine adjuvante Radiotherapie reduziert das Lokalrezidivrisiko, verbessert jedoch nicht das Gesamtüberleben bei Vorliegen von Risikofaktoren sollte ein adjuvante Radio(chemo)therapie erfolgen (nach Leitlinie): positive Lymphknoten, Tumorgröße ≥ 4 cm, tiefe Stromainvasion, R1-Resektion, ausgedehnte parametrane Infiltration, inadäquate Lymphadenektomie (n < 15), Lymphangiosis/ Hämangiosis
therapie erfolgen (nach Leitlinie): positive Lymphknoten, Tumorgröße ≥ 4 cm, tiefe Stromainvasion, R1-Resektion, ausgedehnte parametrane Infiltration, inadäquate Lymphadenektomie (n < 15), Lymphangiosis/ Hämangiosis.")
60
Rezidivsituation: OP oder Systemtherapie?
Rezidivrate gesamt 10–42% ca pro Jahr in Deutschland Rezidivrate FIGO IB–IIA 10–20% FIGO IIB–IVA 50–70% Rezidivrate nach primärer Radiotherapie Lokalrezidiv Fernmetastasen IB 10% 16% IIA 17% 31% IIB 23% 26% III 42% 39% IVA 74% 75% 1-Jahres-Überlebensrate < 15% 3-Jahres-Überlebensrate < 10% Mittleres Überleben, metastasierte Erkrankung 3–6 Monate

61
Exenteration Exenteration nur indiziert, wenn lokales Geschehen und R0-Situation erreichbar erscheint Fernmetastasen werden als Kontraindikation angesehen Keine Daten zu Metastasen-chirurgie plus Exenteration Abhängig von Lokalisation und Größe des Rezidivs Keine Infiltration der Beckenwand Keine paraaortalen Lymphknotenmetastasen Interdisziplinäres Team

62
Chemotherapie: Progressionsfreies Überleben
PFS: Cisplatin: 2.9 Monate CTop: 4.6 Monate p=0.017 Long et al., JCO Randomized Phase III Trial of Cisplatin With or Without Topotecan in Carcinoma of the Uterine Cervix: A Gynecologic Oncology Group Study

63
Chemotherapie: Gesamtüberleben
PFS: Cisplatin: 6.5 Monate CTop: 9.4 Monate p=0.014 Signifikanter Überlebensvorteil einer Kombinationstherapie gg. Cisplatin mono

64
Rezidiv, Metastasen 1. Bei Rezidiv oder Metastasen des Zervixkarzinoms sollte die Möglichkeit der operativen Resektion geprüft werden. 2. Bei Inoperabilität und bislang nicht durchgeführter Strahlentherapie ist eine Radio- (chemo) therapie indiziert. 3. Sind weder Operation, alleinige Chemotherapie noch Strahlentherapie möglich, ist eine Systemtherapie indiziert.
 therapie indiziert. 3. Sind weder Operation, alleinige Chemotherapie noch Strahlentherapie möglich, ist eine Systemtherapie indiziert.")
65
Vielen Dank Neue FIGO-Klassifikation
Maßgeschneiderte operative Therapie: Konisation, Trachelektomie, Radikale Hysterektomie, LNE Sentinel-Konzepte Laparoskopische Verfahren nehmen zu Überarbeitung der Leitlinien Sommer 2010 geplant

Ähnliche Präsentationen









: wann ist ein Blasenerhalt möglich?>")









