Präsentation herunterladen
Die Präsentation wird geladen. Bitte warten

1
DMP KHK, Diabetes und COPD Klosterkirche , Remscheid - Lennep
All in one Aktuelle Therapie 2014 , 15:00 Uhr Klosterkirche , Remscheid - Lennep erklärt: „Eine individuelle Behandlung von Vorhofflimmern erfordert das Verständnis der Krankheitsmechanismen und deren Übersetzung in geeignete Parameter, die wir bei Patienten messen können. Wir hoffen, dass wir in den nächsten paar Jahren eine individualisierte Behandlung empfehlen und dadurch das hohe Sterberisiko dieser Krankheit verringern können. Es gibt noch viel Raum, die Behandlung von Vorhofflimmern zu optimieren, selbst wenn wir all die evidenzbasierten Therapien, die heutzutage verfügbar sind, anwenden. Zum Beispiel haben die neuen oralen Antikoagulanzien die Sterblichkeit nur um 5 bis 10 Prozent reduziert. Jeder vierte Vorhofflimmerpatient wird mindestens einmal pro Jahr wegen Vorhofflimmern ins Krankenhaus eingewiesen, was die hohe Erkrankungshäufigkeit und die enormen Versorgungskosten dieser Krankheit verdeutlicht. Dies ist die erste europäische Konsensuspublikation zur individuellen Behandlung von Vorhofflimmern, dem vielversprechendsten Weg, die Erkrankungshäufigkeit und das Sterberisiko bei Vorhofflimmern zu verringern.“ jedoch nur sehr einfache Anfänge auf dem Weg zu einer individualisierten Therapie. Der Konsensusbericht zeigt drei wesentliche Methoden auf, um die Behandlung von Vorhofflimmern basierend auf seinen Ursachen zu individualisieren: das Elektrokardiogramm (EKG), bildgebende Verfahren wie Echokardiographie und Magnetresonanztomographie (MRT) sowie Biomarker, das sind Proteine oder Gene, die im Blut gemessen werden, um den Typ des Vorhofflimmerns zu bestimmen.
, bildgebende Verfahren wie Echokardiographie und Magnetresonanztomographie (MRT) sowie Biomarker, das sind Proteine oder Gene, die im Blut gemessen werden, um den Typ des Vorhofflimmerns zu bestimmen.")
2
Therapie des Vorhofflimmerns –
Eine personalisierte Behandlungsstrategie Dr. med. Michael Müller – KARDIOPRAX

3
Prävalenz von Vorhofflimmern (USA 1990 – 2050)
VF ist die am weitesten verbreitete anhaltende Art der kardialen Arrhythmie, die 1–2 % der Bevölkerung betrifft Jährliche Kosten für das Gesundheitssystem ca EUR pro Patient I was born in sinus rhythm and I am not willing to die in atrial fibrillation Vorhofflimmern stellt heute mit großem Abstand die am häufigsten beobachtete Herzrhythmusstörung dar. Die Prävalenz dieser Vorhofrhythmusstörung beträgt in der Gesamtbevölkerung ca. 0,4-1 %. Es besteht eine deutliche altersabhängige Zunahme, sodass in der Bevölkerungsgruppe der über 65jährigen von einer Häufigkeit von 5-6 % auszugehen ist. Bei den über 80jähigen besteht bei ca. jedem Zehnten diese Herzrhythmusstörung. Für die Bundesrepublik ergibt sich somit eine geschätzte Patientenzahl von bis Da die Häufigkeit von unbemerktem Vorhofflimmern (silent atrial fibrillation) unbekannt groß ist, muss von einer noch höheren Prävalenz ausgegangen werden. Die demographische Entwicklung, mit einer immer älter werdenden Bevölkerung lässt die Zahl der Patienten mit Vorhofflimmern weiter steigen. If the same prevalence model were used, the projected number of adults with AF for the year 2050 would be 12.1 million (95% CI, 11.4 to 12.9) (2.4-fold increase from 2000), assuming no further increase in age-adjusted AF incidence beyond If we assume a continued increase in the incidence, then the projected number of adults with AF would be 15.9 million (3-fold increase from 2000) (Figure 2). Of the potential increase of 10.8 million persons with AF (5.1 in 2000 to 15.9 million in 2050), 3.8 million (35%) would be attributed to an increase in incidence and 7.0 million (65%) to increase in population size and shifting of the age distribution (2.4 million from population expansion and 4.6 million from increased longevity). Miyasaka et al, Circulation 2006
 unbekannt groß ist, muss von einer noch höheren Prävalenz. ausgegangen werden. Die demographische Entwicklung, mit einer immer älter werdenden. Bevölkerung lässt die Zahl der Patienten mit Vorhofflimmern weiter steigen. If the same prevalence model were used, the projected number of adults with AF for the year 2050 would be million (95% CI, 11.4 to 12.9) (2.4-fold increase from 2000), assuming no further increase in age-adjusted AF incidence. beyond If we assume a continued increase in the incidence, then the projected number of adults with AF would. be 15.9 million (3-fold increase from 2000) (Figure 2). Of the potential increase of 10.8 million persons with AF (5.1 in to 15.9 million in 2050), 3.8 million (35%) would be attributed to an increase in incidence and 7.0 million (65%) to. increase in population size and shifting of the age distribution (2.4 million from population expansion and 4.6 million from. increased longevity). Miyasaka et al, Circulation")
4
Vorhofflimmern ist nicht mehr / nur eine EKG Diagnose
Vorhofflimmern ist eine chronische, aggressive und progressive elektrische Erkrankung des Herzens Vorhofflimmern stellt heute mit großem Abstand die am häufigsten beobachtete Herzrhythmusstörung dar. Die Prävalenz dieser Vorhofrhythmusstörung beträgt in der Gesamtbevölkerung ca. 0,4-1 %. Es besteht eine deutliche altersabhängige Zunahme, sodass in der Bevölkerungsgruppe der über 65jährigen von einer Häufigkeit von 5-6 % auszugehen ist. Bei den über 80jähigen besteht bei ca. jedem Zehnten diese Herzrhythmusstörung. Für die Bundesrepublik ergibt sich somit eine geschätzte Patientenzahl von bis Da die Häufigkeit von unbemerktem Vorhofflimmern (silent atrial fibrillation) unbekannt groß ist, muss von einer noch höheren Prävalenz ausgegangen werden. Die demographische Entwicklung, mit einer immer älter werdenden Bevölkerung lässt die Zahl der Patienten mit Vorhofflimmern weiter steigen. In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
 unbekannt groß ist, muss von einer noch höheren Prävalenz. ausgegangen werden. Die demographische Entwicklung, mit einer immer älter werdenden. Bevölkerung lässt die Zahl der Patienten mit Vorhofflimmern weiter steigen. In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur. Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit. zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei. Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die. Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei. Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und. hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das. Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute. anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).")
5
Mortalität des Vorhofflimmerns
In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
6
Therapie von Vorhofflimmern: Was ist wichtig ?
Rhythmologische Diagnose Kardiovaskuläre Diagnose Symptome / Lebensqualität Risiken Therapieplanung Behandlung Nachbeobachtung In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
7
Therapie von Vorhofflimmern: Diagnose I
Rhythmologische Diagnose - Dokumentation von Vorhofflimmern - Krankheitsverlauf Häufigkeit und Dauer der Episoden ? - Erstdiagnose ? - paroxysmal, persistierend oder permanent - in den letzten 12 Monaten - in den letzten 3 Monaten ? In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
8
Progression von Vorhofflimmern - Standortbestimmung
Im Euro Heart Survey trat nach einjährigem Follow-up bei 15 % der Patienten mit paroxysmalem Vorhofflimmern eine Progression zu persistierendem oder permanentem Vorhofflimmern auf (1). Im CARAF-Register („Canadian Registry of atrial fibrillation“) betrug die Wahrscheinlichkeit einer Progression im ersten Jahr 9% und nach 5 Jahren 25% (2). Das deutsche RECORD-AF-Register zeigte bei 31% der Patienten mit paroxysmalen oder persistierenden Vorhofflimmern nach einem Jahr eine Progression zu permanentem Vorhofflimmern (3). Erstmals dokumentiert VF Stumm Paroxysmal Persistierend Lang-anhaltend persistierend Permanent VF = Vorhofflimmern. Bruggenjurgen et al, Value health 2007 Defaye et al, Pacing Clin Elektroph 1997 Dorian et al, Eur Heart J, 2000
. Im CARAF-Register („Canadian Registry of atrial fibrillation ) betrug die Wahrscheinlichkeit einer Progression im ersten Jahr 9% und nach 5 Jahren 25% (2). Das deutsche RECORD-AF-Register zeigte bei 31% der Patienten mit paroxysmalen oder persistierenden Vorhofflimmern nach einem Jahr eine Progression zu permanentem Vorhofflimmern (3). Erstmals dokumentiert. VF. Stumm. Paroxysmal. Persistierend. Lang-anhaltend persistierend. Permanent. VF = Vorhofflimmern. Bruggenjurgen et al, Value health Defaye et al, Pacing Clin Elektroph Dorian et al, Eur Heart J,")
9
Therapie von Vorhofflimmern: Diagnose II
Kardiovaskuläre Diagnose ? - Ausschluß sek. Ursachen (Hyperthyreose) - fast alle Patienten mit AF haben eine kardiovaskuläre Erkrankung im klinischen oder subklinischem Stadium („lone“ AF < 20%) Arterielle Hypertonie Diabetes mellitus KHK,DCM, Vitien In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
 - fast alle Patienten mit AF haben eine. kardiovaskuläre Erkrankung im klinischen oder. subklinischem Stadium („lone AF < 20%) Arterielle Hypertonie. Diabetes mellitus. KHK,DCM, Vitien. In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur. Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit. zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei. Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die. Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei. Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und. hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das. Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute. anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).")
10
Therapie von Vorhofflimmern: Diagnose II
Es gibt eine Reihe von unabhängigen kardiovaskulären Risikofaktoren für Vorhofflimmern : Prädisponierender Risikofaktor Erhöhung des Risikos für Vorhofflimmern Herzklappendefekt 1,8- bzw. 3,4-fach Herzinsuffizienz 4,5- bzw. 5,9-fach Arterielle Hypertonie 1,5- bzw. 1,4-fach Diabetes mellitus 1,4- bzw. 1,6-fach In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
11
Therapie von Vorhofflimmern: Diagnose III
Welche Untersuchungen sind erforderlich: „kleines Labor“ körperliche Untersuchung EKG, Bel.- EKG Echokardiographie Stressecho, Stress MRT, Herzkatheter ? Nur bei begründetem Verdacht auf eine schwerwiegende strukturelle Herzerkrankung In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
13
Therapie von Vorhofflimmern: Was ist wichtig ?
Rhythmologische Diagnose Kardiovaskuläre Diagnose Symptome / Lebensqualität Risiken Therapieplanung Behandlung Nachbeobachtung In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
14
Therapie von Vorhofflimmern: Symptome & Risiken
Symptome sind Leitindikator für die Therapie - asymptomatische Patienten - mild symptomatische Patienten - hochsymptomatische Patienten Aber: auch bei hochsymptomatischen Patienten können mehr als 50% der Episoden asymptomatisch sein AF-bezogene Risiken bedenken - thromboembolische Komplikationen - Herzinsuffizienz / Tachykardiomyopathie In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
15
Therapie von Vorhofflimmern: Symptome & Risiken
In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
16
Therapie von Vorhofflimmern: Praktisches Vorgehen
Walter hat Vorhofflimmern …. 53 Jahre, Lehrer ED von AF 2010 hochsymptomatisch (EHRA III-IV) art. Hypertonie, gute LV- Funktion, keine KHK
 art. Hypertonie, gute LV- Funktion, keine KHK.")
17
Therapie von Vorhofflimmern: Praktisches Vorgehen
Walter hat Vorhofflimmern …. Bild eines LZ - EKG

18
Therapie von Vorhofflimmern: Praktisches Vorgehen
Walter hat Vorhofflimmern …. % AF KV KV Flecainid ED Zeit

19
Therapie von Vorhofflimmern: Was ist wichtig ?
Rhythmologische Diagnose Kardiovaskuläre Diagnose Symptome / Lebensqualität Risiken Therapieplanung Behandlung Nachbeobachtung In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
20
Progression von Vorhofflimmern - Standortbestimmung
“Vorgelagerte” Behandlung von Begleiterkrankungen Antikoagulation Frequenzkontrolle Antiarrhythmische Medikamente Ablation Erstmals dokumentiert Kardioversion VF Stumm Paroxysmal Persistierend Lang-anhaltend persistierend Permanent VF = Vorhofflimmern. 1. The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31:2369–2429.
. Eur Heart J. 2010;31:2369–2429.")
21
Frage :. Ist der Erhalt des. Sinusrhythmus besser als
Frage : Ist der Erhalt des Sinusrhythmus besser als eine Frequenzkontrolle ?

22
Studienlage: Frequenz- vs.
Rhythmuskontrolle Eine post Hoc Analyse der AFFIRM Studie zeigte eine signifikant erniedrigte Mortalitätsrate ,wenn der Sinusrhythmus erhalten werden konnte, wo hingegen der Gebrauch von AA mit einer erhöhten Mortalitätsrate von 49% vergesellschaftet war . Ein relevanter Teil der Sterblichkeit in der Rhythmuskontrollgruppe kann auch durch zu frühes Absetzen der oralen Antikoagulation erklärt werden Kommentar Zum jetzigen Zeitpunkt muss man schlussfolgern, dass weder die Frequenzkontrolle noch die Rhythmuskontrolle bezüglich Lebensqualitat und Prognose der jeweils anderen Therapiestrategie signifikant uberlegen ist [6][7][8]. Zu beachten ist dabei, dass im Rahmen der Rhythmuskontrolle neben der elektrischen Kardioversion lediglich pharmakologische Masnahmen zur Anwendung kamen, deren Vermogen, Sinusrhythmus dauerhaft zu erhalten, sich als deutlich limitiert erwies. So zeigte sich beispielsweise bei Patienten mit persistierendem Vorhofflimmern (RACE und STAF-Studie), dass der Sinusrhythmus tatsachlich nur in weniger als 50% erhalten werden konnte. Man muss daher fairerweise dem Konzept des Sinusrhythmuserhalts einraumen, dass in den bisher durchgefuhrten Studien ein durchgehender Sinusrhythmuserhalt nur unzureichend erzielt werden konnte. Die Frage, wie denn die Studien ausgefallen waren, wenn es gelange, in z. B. >80–90% aller Falle den Sinusrhythmus durchgehend herzustellen, womoglich noch ohne Nebenwirkungen der pharmakologischen Therapie, ist von daher berechtigt. Diese Diskussion erfahrt unter anderem aus einer Posthoc- Analyse der AFFIRM-Studie Unterstutzung, die fur die Patienten, die effektiv im Sinusrhythmus gehalten werden konnten, eine signifikant niedrigere Sterblichkeitnachwies. Es bleibt also festzuhalten, dass die oben aufgefuhrten Ergebnisse ihre Bedeutung fur die nur inkomplett effektive, medikamentose Rezidivprophylaxe besitzen. Von daher sind zukunftige Studien von groser Bedeutung, die uberprufen, ob der langfristige Erhalt des physiologischen Sinusrhythmus mit nichtmedikamentosen Mitteln nicht doch bezuglich Prognose, Lebensqualitat und thrombembolischem Risiko dem frequenzkontrollierten Vorhofflimmern uberlegen ist. Daruber hinaus kann ein relevanter Teil der Sterblichkeit in der Rhythmuskontrollgruppe durch eine – aus heutiger Sicht – verfruhte Beendigung der oralen Antikoagulation erklart werden. In zukunftigen Untersuchungen wie auch in der jetzigen klinischen Praxis wird die Durchfuhrung der Antikoagulation bei einem Patienten mit Vorhofflimmern vom Vorliegen von Risikofaktoren abhangig gemacht werden und nicht mehr vom zeitweise erzielten Rhythmus. Lange Zeit hat man geglaubt, dass der Erhalt des Sinusrhythmus die Prognose der Patienten verbessert. Nach den Ergebnissen der Rhythmus- vs. Frequenzkontroll – Studien (PIAF, AFFIRM, RACE, STAF, Hot-CAFE) ist diese Annahme jedoch eindeutig wiederlegt worden. Seitdem ist es absolut gerechtfertigt, asymptomatische Patienten im Vorhofflimmern zu belassen und mit frequenzsenkenden Medikamenten zu behandeln (Betablocker, Calciumantagonisten, Digitalis PIAF Studie: 2000 Background Atrial fibrillation is the most commonly encountered sustained cardiac arrhythmia. Restoration and maintenance of sinus rhythm is believed by many physicians to be superior to rate control only. However, there are no prospective data that compare both therapeutic strategies. Methods The Pharmacological Intervention in Atrial Fibrillation (PIAF) trial was a randomised trial in 252 patients with atrial fibrillation of between 7 days and 360 days duration, which compared rate (group A, 125 patients) with rhythm control (group B, 127 patients). In group A, diltiazem was used as first-line therapy and amiodarone was used in group B. The primary study endpoint was improvement in symptoms related to atrial fibrillation. Findings Over the entire observation period of 1 year, a similar proportion of patients reported improvement in symptoms in both groups (76 responders at 12 months in group A vs 70 responders in group B, p=0·317). Amiodarone administration resulted in pharmacological restoration of sinus rhythm in 23% of patients. Walking distance in a 6 min walk test was better in group B compared with group A, but assessment of quality of life showed no differences between groups. The incidence of hospital admission was higher in group B (87 [69%] out of 127 vs 30 [24%] out of 125 in group A, p=0·001). Adverse drug effects more frequently led to a change in therapy in group B (31 [25%] patients compared with 17 [14%] in group A, p=0·036. Interpretation With respect to symptomatic improvement in patients with atrial fibrillation, the therapeutic strategies of rate versus rhythm control yielded similar clinical results overall. However, exercise tolerance is better with rhythm control, although hospital admission is more frequent. These data may serve as a basis to select therapy in individual patients. Figures and tables from this article: Figure 1. Trial profile Figure options Figure 2. Proportion of patients reporting improvement in clinical symptoms during follow-up There was no significant difference between both therapeutic strategies with respect to the primary study endpoint. Figure 3. Mean data and associated 95% Cl for 24 h average heart rate during atrial fibrillation assessed from Holter monitoring In group A, there was continuous decline in mean heart rate over the entire observation period. In group B, amiodarone was associated with significant initial decline in heart rate. At later observation times, the majority of group-B patients was in sinus rhythm. Figure 4. Maintenance of sinus rhythm during the observation period as assessed from patients with 24 h Holter recordings Figure 5. Mean data and associated 95% Cl in exercise tolerance as assessed by repeated 6 min walk tests Group-B patients showed significant increase in walking distance compared with group-A patients. STAF Studie: 2003 Objectives This study was designed to compare two treatment strategies in patients with atrial fibrillation (AF): rhythm-control (restoration and maintenance of sinus rhythm) and rate-control (pharmacologic or invasive rate-control and anticoagulation). Atrial fibrillation is the most common arrhythmia. It is unclear whether a strategy of rhythm- or rate-control is better in terms of mortality, morbidity, and quality of life. The Strategies of Treatment of Atrial Fibrillation (STAF) multicenter pilot trial randomized 200 patients (100 per group) with persistent AF to rhythm- or rate-control. The combined primary end point was a combination of death, cardiopulmonary resuscitation, cerebrovascular event, and systemic embolism. Results After 19.6 ± 8.9 months (range 0 to 36 months) there was no difference in the primary end point between rhythm-control (9/100; 5.54%/year) and rate-control (10/100; 6.09%/year; p = 0.99). The percentage of patients in sinus rhythm in the rhythm-control group after up to four cardioversions during the follow-up period (rate-control group) was 23% (0%) at 36 months. Eighteen primary end points occurred in atrial fibrillation; only one occurred in sinus rhythm (p = 0.049). Conclusions The STAF pilot study showed no differences between the two treatment strategies in all end points except hospitalizations. These data suggest that there was no benefit in attempting rhythm-control in these patients with a high risk of arrhythmia recurrence. It remains unclear whether the results in the rhythm-control group would have been better if sinus rhythm had been maintained in a higher proportion of patients, as all but one end point occurred during AF. AFFIRM Studie: 2004 BACKGROUND: The AFFIRM Study showed that treatment of patients with atrial fibrillation and a high risk for stroke or death with a rhythm-control strategy offered no survival advantage over a rate-control strategy in an intention-to-treat analysis. This article reports an "on-treatment" analysis of the relationship of survival to cardiac rhythm and treatment as they changed over time. METHODS AND RESULTS: Modeling techniques were used to determine the relationships among survival, baseline clinical variables, and time-dependent variables. The following baseline variables were significantly associated with an increased risk of death: increasing age, coronary artery disease, congestive heart failure, diabetes, stroke or transient ischemic attack, smoking, left ventricular dysfunction, and mitral regurgitation. Among the time-dependent variables, the presence of sinus rhythm (SR) was associated with a lower risk of death, as was warfarin use. Antiarrhythmic drugs (AADs) were associated with increased mortality only after adjustment for the presence of SR. Consistent with the original intention-to-treat analysis, AADs were no longer associated with mortality when SR was removed from the model. CONCLUSIONS: Warfarin use improves survival. SR is either an important determinant of survival or a marker for other factors associated with survival that were not recorded, determined, or included in the survival model. Currently available AADs are not associated with improved survival, which suggests that any beneficial antiarrhythmic effects of AADs are offset by their adverse effects. If an effective method for maintaining SR with fewer adverse effects were available, it might be beneficial. A post Hoc on treatment analysis revealed that the presence of sinus rhythm was associated with a significant reduction in mortality, whereas the use of AA increased mortality by 49% HOT CAFÉ Studie: 2004 STUDY OBJECTIVES: The relative risks and benefits of strategies of rate control vs rhythm control in patients with atrial fibrillation (AF) remain to be fully explored. DESIGN: The How to Treat Chronic Atrial Fibrillation (HOT CAFE) Polish trial was designed to evaluate in a randomized, multicenter, and prospective manner the feasibility and long-term outcomes of rate control vs rhythm control strategies in patients with persistent AF. PATIENTS: Our study population comprised 205 patients (134 men and 71 women; mean [+/- SD] age, / years) with a mean AF duration of / days. The mean observation period was 1.7 +/- 0.4 years. One hundred one patients were randomly assigned to the rate control group and received rate-slowing therapy guided by repeated 24-h Holter monitoring. Direct current cardioversion and atrioventricular junctional ablation with pacemaker placement were alternative nonpharmacologic strategies for patients with tachycardia that was resistant to medical therapy. One hundred four patients were randomized to sinus rhythm restoration and maintenance using serial cardioversion supported by a predefined stepwise antiarrhythmic drug regimen (ie, disopyramide, propafenone, sotalol, and amiodarone). In both groups, thromboembolic prophylaxis followed current guidelines. MEASUREMENTS AND RESULTS: At the end of follow-up, 63.5% of patients in the rhythm control arm remained in sinus rhythm. No significant differences in the composite end point (ie, all-cause mortality, number of thromboembolic events, or major bleeding) were found between the rate control group and the rhythm control group (odds ratio, 1.98; 95% confidence interval, 0.28 to 22.3; p > 0.71). The incidence of hospital admissions was much lower in the rate control arm (12% vs 74%, respectively; p < 0.001). New York Heart Association functional class improved in both study groups, while mean exercise tolerance, as measured by the maximal treadmill workload, improved only in the rhythm control group (5.2 +/- 5.1 vs 7.6 +/- 3.3 metabolic equivalents, respectively; p < 0.001). The rhythm control strategy led to an increased mean left ventricular fractional shortening (29 +/- 7% vs 31 +/- 7%, respectively; p < 0.01). One episode of pulmonary embolism occurred in the rate control group despite oral anticoagulation therapy, while three patients in the rhythm control arm of the study experienced ischemic strokes (not significant). CONCLUSIONS: The Polish HOT CAFE study revealed no significant differences in major end points between the rate control group and the rhythm control group. AF CHF Studie: 2008 It is common practice to restore and maintain sinus rhythm in patients with atrial fibrillation and heart failure. This approach is based in part on data indicating that atrial fibrillation is a predictor of death in patients with heart failure and suggesting that the suppression of atrial fibrillation may favorably affect the outcome. However, the benefits and risks of this approach have not been adequately studied. Full Text of Background... We conducted a multicenter, randomized trial comparing the maintenance of sinus rhythm (rhythm control) with control of the ventricular rate (rate control) in patients with a left ventricular ejection fraction of 35% or less, symptoms of congestive heart failure, and a history of atrial fibrillation. The primary outcome was the time to death from cardiovascular causes. Full Text of Methods... A total of 1376 patients were enrolled (682 in the rhythm-control group and 694 in the rate-control group) and were followed for a mean of 37 months. Of these patients, 182 (27%) in the rhythm-control group died from cardiovascular causes, as compared with 175 (25%) in the rate-control group (hazard ratio in the rhythm-control group, 1.06; 95% confidence interval, 0.86 to 1.30; P=0.59 by the log-rank test). Secondary outcomes were similar in the two groups, including death from any cause (32% in the rhythm-control group and 33% in the rate-control group), stroke (3% and 4%, respectively), worsening heart failure (28% and 31%), and the composite of death from cardiovascular causes, stroke, or worsening heart failure (43% and 46%). There were also no significant differences favoring either strategy in any predefined subgroup. J-Rhythm Studie 2009: Abstract Background Although previous clinical trials demonstrated the non-inferiority of a rate control to rhythm control strategy for management of atrial fibrillation (AF), the optimal treatment strategy for paroxysmal AF (PAF) remains unclear. Methods and Results A randomized, multicenter comparison of rate control vs rhythm control in Japanese patients with PAF (the Japanese Rhythm Management Trial for Atrial Fibrillation (J-RHYTHM) study) was conducted. The primary endpoint was a composite of total mortality, symptomatic cerebral infarction, systemic embolism, major bleeding, hospitalization for heart failure, or physical/psychological disability requiring alteration of treatment strategy. In the study, 823 patients with PAF were followed for a mean period of 578 days. The primary endpoint occurred in 64 patients (15.3%) assigned to rhythm control and in 89 patients (22.0%) to rate control (P=0.0128). No significant differences between the treatment strategies were observed in the incidences of death, stroke, bleeding and heart failure. Meanwhile, significantly fewer patients requested changes of assigned treatment strategy in the rhythm control vs the rate control group, which was accompanied by improvement in AF-specific quality of life scores. Conclusion The J-RHYTHM study showed that rhythm control was associated with fewer primary endpoints than rate control. However, mortality and cardiovascular morbidity were not affected by the treatment strategy (umin-CTR No. C ). Lewalter et al; Kardiologe 2008 ・ 2:181–205
, dass der Sinusrhythmus tatsachlich nur in weniger als 50% erhalten werden konnte. Man muss daher fairerweise dem Konzept des Sinusrhythmuserhalts einraumen, dass in den bisher durchgefuhrten Studien ein durchgehender Sinusrhythmuserhalt nur unzureichend erzielt werden konnte. Die Frage, wie denn die Studien ausgefallen waren, wenn es gelange, in z. B. >80–90% aller Falle den Sinusrhythmus durchgehend herzustellen, womoglich noch ohne Nebenwirkungen der pharmakologischen Therapie, ist von daher berechtigt. Diese Diskussion erfahrt unter anderem aus einer Posthoc- Analyse der AFFIRM-Studie Unterstutzung, die fur die Patienten, die effektiv im Sinusrhythmus gehalten werden konnten, eine signifikant niedrigere Sterblichkeitnachwies. Es bleibt also festzuhalten, dass die oben aufgefuhrten Ergebnisse ihre Bedeutung fur die nur inkomplett effektive, medikamentose Rezidivprophylaxe besitzen. Von daher sind zukunftige Studien von groser Bedeutung, die uberprufen, ob der langfristige Erhalt des physiologischen Sinusrhythmus mit nichtmedikamentosen Mitteln nicht doch bezuglich Prognose, Lebensqualitat und thrombembolischem Risiko. dem frequenzkontrollierten Vorhofflimmern uberlegen ist. Daruber hinaus kann ein relevanter Teil der Sterblichkeit in der Rhythmuskontrollgruppe durch eine – aus heutiger Sicht – verfruhte Beendigung der oralen Antikoagulation erklart werden. In zukunftigen Untersuchungen wie auch in der jetzigen klinischen Praxis wird die Durchfuhrung der Antikoagulation bei einem Patienten mit Vorhofflimmern vom Vorliegen von Risikofaktoren abhangig gemacht werden und nicht mehr vom zeitweise. erzielten Rhythmus. Lange Zeit hat man geglaubt, dass der Erhalt des Sinusrhythmus die Prognose der Patienten verbessert. Nach den Ergebnissen der Rhythmus- vs. Frequenzkontroll – Studien (PIAF, AFFIRM, RACE, STAF, Hot-CAFE) ist diese Annahme jedoch eindeutig wiederlegt worden. Seitdem ist es absolut gerechtfertigt, asymptomatische Patienten im Vorhofflimmern zu. belassen und mit frequenzsenkenden Medikamenten zu behandeln (Betablocker, Calciumantagonisten, Digitalis. PIAF Studie: Background. Atrial fibrillation is the most commonly encountered sustained cardiac arrhythmia. Restoration and maintenance of sinus rhythm is believed by many physicians to be superior to rate control only. However, there are no prospective data that compare both therapeutic strategies. Methods. The Pharmacological Intervention in Atrial Fibrillation (PIAF) trial was a randomised trial in 252 patients with atrial fibrillation of between 7 days and 360 days duration, which compared rate (group A, 125 patients) with rhythm control (group B, 127 patients). In group A, diltiazem was used as first-line therapy and amiodarone was used in group B. The primary study endpoint was improvement in symptoms related to atrial fibrillation. Findings. Over the entire observation period of 1 year, a similar proportion of patients reported improvement in symptoms in both groups (76 responders at 12 months in group A vs 70 responders in group B, p=0·317). Amiodarone administration resulted in pharmacological restoration of sinus rhythm in 23% of patients. Walking distance in a 6 min walk test was better in group B compared with group A, but assessment of quality of life showed no differences between groups. The incidence of hospital admission was higher in group B (87 [69%] out of 127 vs 30 [24%] out of 125 in group A, p=0·001). Adverse drug effects more frequently led to a change in therapy in group B (31 [25%] patients compared with 17 [14%] in group A, p=0·036. Interpretation. With respect to symptomatic improvement in patients with atrial fibrillation, the therapeutic strategies of rate versus rhythm control yielded similar clinical results overall. However, exercise tolerance is better with rhythm control, although hospital admission is more frequent. These data may serve as a basis to select therapy in individual patients. Figures and tables from this article: Figure 1. Trial profile. Figure options. Figure 2. Proportion of patients reporting improvement in clinical symptoms during follow-up. There was no significant difference between both therapeutic strategies with respect to the primary study endpoint. Figure 3. Mean data and associated 95% Cl for 24 h average heart rate during atrial fibrillation assessed from Holter monitoring. In group A, there was continuous decline in mean heart rate over the entire observation period. In group B, amiodarone was associated with significant initial decline in heart rate. At later observation times, the majority of group-B patients was in sinus rhythm. Figure 4. Maintenance of sinus rhythm during the observation period as assessed from patients with 24 h Holter recordings. Figure 5. Mean data and associated 95% Cl in exercise tolerance as assessed by repeated 6 min walk tests. Group-B patients showed significant increase in walking distance compared with group-A patients. STAF Studie: Objectives. This study was designed to compare two treatment strategies in patients with atrial fibrillation (AF): rhythm-control (restoration and maintenance of sinus rhythm) and rate-control (pharmacologic or invasive rate-control and anticoagulation). Atrial fibrillation is the most common arrhythmia. It is unclear whether a strategy of rhythm- or rate-control is better in terms of mortality, morbidity, and quality of life. The Strategies of Treatment of Atrial Fibrillation (STAF) multicenter pilot trial randomized 200 patients (100 per group) with persistent AF to rhythm- or rate-control. The combined primary end point was a combination of death, cardiopulmonary resuscitation, cerebrovascular event, and systemic embolism. Results. After 19.6 ± 8.9 months (range 0 to 36 months) there was no difference in the primary end point between rhythm-control (9/100; 5.54%/year) and rate-control (10/100; 6.09%/year; p = 0.99). The percentage of patients in sinus rhythm in the rhythm-control group after up to four cardioversions during the follow-up period (rate-control group) was 23% (0%) at 36 months. Eighteen primary end points occurred in atrial fibrillation; only one occurred in sinus rhythm (p = 0.049). Conclusions. The STAF pilot study showed no differences between the two treatment strategies in all end points except hospitalizations. These data suggest that there was no benefit in attempting rhythm-control in these patients with a high risk of arrhythmia recurrence. It remains unclear whether the results in the rhythm-control group would have been better if sinus rhythm had been maintained in a higher proportion of patients, as all but one end point occurred during AF. AFFIRM Studie: BACKGROUND: The AFFIRM Study showed that treatment of patients with atrial fibrillation and a high risk for stroke or death with a rhythm-control strategy offered no survival advantage over a rate-control strategy in an intention-to-treat analysis. This article reports an on-treatment analysis of the relationship of survival to cardiac rhythm and treatment as they changed over time. METHODS AND RESULTS: Modeling techniques were used to determine the relationships among survival, baseline clinical variables, and time-dependent variables. The following baseline variables were significantly associated with an increased risk of death: increasing age, coronary artery disease, congestive heart failure, diabetes, stroke or transient ischemic attack, smoking, left ventricular dysfunction, and mitral regurgitation. Among the time-dependent variables, the presence of sinus rhythm (SR) was associated with a lower risk of death, as was warfarin use. Antiarrhythmic drugs (AADs) were associated with increased mortality only after adjustment for the presence of SR. Consistent with the original intention-to-treat analysis, AADs were no longer associated with mortality when SR was removed from the model. CONCLUSIONS: Warfarin use improves survival. SR is either an important determinant of survival or a marker for other factors associated with survival that were not recorded, determined, or included in the survival model. Currently available AADs are not associated with improved survival, which suggests that any beneficial antiarrhythmic effects of AADs are offset by their adverse effects. If an effective method for maintaining SR with fewer adverse effects were available, it might be beneficial. A post Hoc on treatment analysis revealed that the presence of sinus rhythm was associated with a significant reduction in mortality, whereas the use of AA increased mortality by 49% HOT CAFÉ Studie: STUDY OBJECTIVES: The relative risks and benefits of strategies of rate control vs rhythm control in patients with atrial fibrillation (AF) remain to be fully explored. DESIGN: The How to Treat Chronic Atrial Fibrillation (HOT CAFE) Polish trial was designed to evaluate in a randomized, multicenter, and prospective manner the feasibility and long-term outcomes of rate control vs rhythm control strategies in patients with persistent AF. PATIENTS: Our study population comprised 205 patients (134 men and 71 women; mean [+/- SD] age, / years) with a mean AF duration of / days. The mean observation period was 1.7 +/- 0.4 years. One hundred one patients were randomly assigned to the rate control group and received rate-slowing therapy guided by repeated 24-h Holter monitoring. Direct current cardioversion and atrioventricular junctional ablation with pacemaker placement were alternative nonpharmacologic strategies for patients with tachycardia that was resistant to medical therapy. One hundred four patients were randomized to sinus rhythm restoration and maintenance using serial cardioversion supported by a predefined stepwise antiarrhythmic drug regimen (ie, disopyramide, propafenone, sotalol, and amiodarone). In both groups, thromboembolic prophylaxis followed current guidelines. MEASUREMENTS AND RESULTS: At the end of follow-up, 63.5% of patients in the rhythm control arm remained in sinus rhythm. No significant differences in the composite end point (ie, all-cause mortality, number of thromboembolic events, or major bleeding) were found between the rate control group and the rhythm control group (odds ratio, 1.98; 95% confidence interval, 0.28 to 22.3; p > 0.71). The incidence of hospital admissions was much lower in the rate control arm (12% vs 74%, respectively; p < 0.001). New York Heart Association functional class improved in both study groups, while mean exercise tolerance, as measured by the maximal treadmill workload, improved only in the rhythm control group (5.2 +/- 5.1 vs 7.6 +/- 3.3 metabolic equivalents, respectively; p < 0.001). The rhythm control strategy led to an increased mean left ventricular fractional shortening (29 +/- 7% vs 31 +/- 7%, respectively; p < 0.01). One episode of pulmonary embolism occurred in the rate control group despite oral anticoagulation therapy, while three patients in the rhythm control arm of the study experienced ischemic strokes (not significant). CONCLUSIONS: The Polish HOT CAFE study revealed no significant differences in major end points between the rate control group and the rhythm control group. AF CHF Studie: It is common practice to restore and maintain sinus rhythm in patients with atrial fibrillation and heart failure. This approach is based in part on data indicating that atrial fibrillation is a predictor of death in patients with heart failure and suggesting that the suppression of atrial fibrillation may favorably affect the outcome. However, the benefits and risks of this approach have not been adequately studied. Full Text of Background... We conducted a multicenter, randomized trial comparing the maintenance of sinus rhythm (rhythm control) with control of the ventricular rate (rate control) in patients with a left ventricular ejection fraction of 35% or less, symptoms of congestive heart failure, and a history of atrial fibrillation. The primary outcome was the time to death from cardiovascular causes. Full Text of Methods... A total of 1376 patients were enrolled (682 in the rhythm-control group and 694 in the rate-control group) and were followed for a mean of 37 months. Of these patients, 182 (27%) in the rhythm-control group died from cardiovascular causes, as compared with 175 (25%) in the rate-control group (hazard ratio in the rhythm-control group, 1.06; 95% confidence interval, 0.86 to 1.30; P=0.59 by the log-rank test). Secondary outcomes were similar in the two groups, including death from any cause (32% in the rhythm-control group and 33% in the rate-control group), stroke (3% and 4%, respectively), worsening heart failure (28% and 31%), and the composite of death from cardiovascular causes, stroke, or worsening heart failure (43% and 46%). There were also no significant differences favoring either strategy in any predefined subgroup. J-Rhythm Studie 2009: Abstract. Background Although previous clinical trials demonstrated the non-inferiority of a rate control to rhythm control strategy for management of atrial fibrillation (AF), the optimal treatment strategy for paroxysmal AF (PAF) remains unclear. Methods and Results A randomized, multicenter comparison of rate control vs rhythm control in Japanese patients with PAF (the Japanese Rhythm Management Trial for Atrial Fibrillation (J-RHYTHM) study) was conducted. The primary endpoint was a composite of total mortality, symptomatic cerebral infarction, systemic embolism, major bleeding, hospitalization for heart failure, or physical/psychological disability requiring alteration of treatment strategy. In the study, 823 patients with PAF were followed for a mean period of 578 days. The primary endpoint occurred in 64 patients (15.3%) assigned to rhythm control and in 89 patients (22.0%) to rate control (P=0.0128). No significant differences between the treatment strategies were observed in the incidences of death, stroke, bleeding and heart failure. Meanwhile, significantly fewer patients requested changes of assigned treatment strategy in the rhythm control vs the rate control group, which was accompanied by improvement in AF-specific quality of life scores. Conclusion The J-RHYTHM study showed that rhythm control was associated with fewer primary endpoints than rate control. However, mortality and cardiovascular morbidity were not affected by the treatment strategy (umin-CTR No. C ). Lewalter et al; Kardiologe 2008 ・ 2:181–205.")
23
Frequenzkontrolle bei Vorhofflimmern
Empfehlung / Evidenz I A Digoxin was associated with a significant increase in all-cause mortality in patients with AF after correcting for clinical characteristics an comorbidities, regardless of gender or of the presence or absence of HF. I A I B I B Eur Heart J 2010;31:

24
Optimale Frequenzkontrolle: wie streng?
614 Patienten Frequenzkontrolle moderat = < 110/min Beobachtungszeitraum 2-3 Jahre streng = < 80/min RACE II Studie Background Rate control is often the therapy of choice for atrial fibrillation. Guidelines recommend strict rate control, but this is not based on clinical evidence. We hypothesized that lenient rate control is not inferior to strict rate control for preventing cardiovascular morbidity and mortality in patients with permanent atrial fibrillation. Methods We randomly assigned 614 patients with permanent atrial fibrillation to undergo a lenient rate-control strategy (resting heart rate <110 beats per minute) or a strict ratecontrol strategy (resting heart rate <80 beats per minute and heart rate during moderate exercise <110 beats per minute). The primary outcome was a composite of death from cardiovascular causes, hospitalization for heart failure, and stroke, systemic ,embolism, bleeding, and life-threatening arrhythmic events. The duration of followup was at least 2 years, with a maximum of 3 years. Results The estimated cumulative incidence of the primary outcome at 3 years was 12.9% in the lenient-control group and 14.9% in the strict-control group, with an absolute difference with respect to the lenient-control group of −2.0 percentage points (90% confidence interval, −7.6 to 3.5; P<0.001 for the prespecified noninferiority margin). The frequencies of the components of the primary outcome were similar in the two groups. More patients in the lenient-control group met the heart-rate target or targets (304 [97.7%], vs. 203 [67.0%] in the strict-control group; P<0.001) with fewer total visits (75 [median, 0], vs. 684 [median, 2]; P<0.001). The frequencies of symptoms and adverse events were similar in the two groups. Conclusions In patients with permanent atrial fibrillation, lenient rate control is as effective as strict rate control and is easier to achieve. (ClinicalTrials.gov number, NCT ) NEJM 2010; 362:
 or a strict ratecontrol strategy (resting heart rate <80 beats per minute and heart rate during moderate. exercise <110 beats per minute). The primary outcome was a composite of death from cardiovascular causes, hospitalization for heart failure, and stroke, systemic ,embolism, bleeding, and life-threatening arrhythmic events. The duration of followup. was at least 2 years, with a maximum of 3 years. Results. The estimated cumulative incidence of the primary outcome at 3 years was 12.9% in the lenient-control group and 14.9% in the strict-control group, with an absolute difference with respect to the lenient-control group of −2.0 percentage points (90% confidence interval, −7.6 to 3.5; P<0.001 for the prespecified noninferiority margin). The frequencies of the components of the primary outcome were similar in the two groups. More patients in the lenient-control group met the heart-rate target or targets. (304 [97.7%], vs. 203 [67.0%] in the strict-control group; P<0.001) with fewer total visits (75 [median, 0], vs. 684 [median, 2]; P<0.001). The frequencies of symptoms and adverse events were similar in the two groups. Conclusions. In patients with permanent atrial fibrillation, lenient rate control is as effective as strict rate control and is easier to achieve. (ClinicalTrials.gov number, NCT ) NEJM 2010; 362:")
25
Therapie von Vorhofflimmern: Praktisches Vorgehen
Was möchte Walter …. % AF SR KV KV Flecainid ED Zeit

26
Frage 2: Wenn Rhythmuskontrolle - Wie ?

27
Amiodaron: Gute Wirksamkeit in der Rezidivprophylaxe
Solche Patienten, die allerdings als mittel bis hochsymptomatische gelten (EHRA II-IV) müssen bzw. sollten behandelt werden. In den aktuellen ESC -Leitlinien wird eine antiarrhythmische Therapie in Abhängigkeit der Grunderkrankung empfohlen, entweder mit einem Klasse I Antiarrhythmika (Flecainid, Propafenon), oder einem Klasse III Antiarrhythmika (Sotalol, Amiodaron, Dronedaron) zu behandeln (siehe Abbildung 1). Das neueste und anfangs sehr verheißungsvolle Medikament Dronedaron zeigte zwar erstmals und als einziges Antiarrhythmika eine Prognoseverbesserung (ATHENA), hat allerdings die geringste antiarrhythmische Potenz. Zudem zeigten weiterführende Studien eine Übersterblichkeit bei Herzinsuffizienz NYHA III und IV, sowie bei permanentem Vorhofflimmern (PALLAS). Insgesamt bleibt bei der antiarrhythmische Therapie, mit welcher Substanz auch immer, festzuhalten, dass etwa 70 % der Patienten 1 Jahr nach einer Kardioversion wieder im Vorhofflimmern sind (vs % ohne antiarrhythmische Therapie) Roy et al, NEJM 2000
 müssen bzw. sollten behandelt werden. In den aktuellen ESC -Leitlinien wird eine antiarrhythmische Therapie in Abhängigkeit der Grunderkrankung empfohlen, entweder mit. einem Klasse I Antiarrhythmika (Flecainid, Propafenon), oder einem Klasse III Antiarrhythmika (Sotalol, Amiodaron, Dronedaron) zu behandeln (siehe Abbildung 1). Das neueste und anfangs sehr verheißungsvolle Medikament Dronedaron zeigte zwar erstmals. und als einziges Antiarrhythmika eine Prognoseverbesserung (ATHENA), hat allerdings die geringste antiarrhythmische Potenz. Zudem zeigten weiterführende Studien eine Übersterblichkeit bei Herzinsuffizienz NYHA III und IV, sowie bei permanentem. Vorhofflimmern (PALLAS). Insgesamt bleibt bei der antiarrhythmische Therapie, mit welcher Substanz auch immer, festzuhalten, dass etwa 70 % der Patienten 1 Jahr nach einer Kardioversion wieder im. Vorhofflimmern sind (vs % ohne antiarrhythmische Therapie) Roy et al, NEJM")
28
Amiodaron: Nebenwirkungen
Retrospektive Analyse: 168 Patienten unter Amiodaron, Nachbeobachtung: 3 Jahre Chandhok et al, J Cardiovasc Electrophysiol 2007;18:714 f

29
Katheterablation von Vorhofflimmern
2012 wurden mehr als Katheterablationen inklusive Vorhofflimmerablationen an mehr als 300 Zentren mit steigender Tendenz durchgeführt (The EHRA White book 2013) In die RAAFT-2 benannte randomisierte Studie, die Dr. Carlos Morillo aus Hamilton/Kanada vorgestellt hat, waren 127 relativ junge Patienten mit symptomatischem paroxysmalem (87,5 Prozent) oder persistierendem Vorhofflimmern aufgenommen worden, davon die meisten an Zentren in Kanada und Deutschland. Die Studienteilnehmer, die so gut wie keine kardiovaskulären Begleiterkrankungen und insofern auch ein sehr niedriges Schlaganfallrisiko hatten, waren zuvor nicht mit Antiarrhythmika behandelt worden. Das Studienprotokoll sah vor, dass die der Radiofrequenz-Ablationstherapie zugeteilten Patienten innerhalb von vier bis sechs Wochen dieser Intervention unterzogen werden. In der Vergleichsgruppe mit medikamentöser Therapie gewährte man 90 Tage für die Einstellung auf die gewählten Antiarrhythmika, am häufigsten Flecainid und Propafenon. In der Nachbeobachtung verließ man sich nicht allein auf die Dokumentation symptomatischer Rezidive. Zur Erfassung auch von asymptomatischen Arrhythmie-Rückfällen wurden alle Patienten ab dem dritten Monat mit einem transtelefonischen Monitor (TTM) ausgestattet. Die Nachbeobachtung betrug bis zu zwei Jahre (im Schnitt 21 Monate). Primärer Endpunkt war die in dieser Zeit akkumulierte Rate der per EKG oder TTM objektivierten symptomatischen und asymptomatischen Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien). Arrhythmie-Rezidive signifikant reduziert Mit 55 Prozent im Vergleich zu 72 Prozent war diese Rate in der Gruppe mit Ablation signifikant niedriger, so das von Morillo präsentierte Hauptergebnis. Die relative Risikoreduktion durch die Ablation gab er mit 46 Prozent an. Auch die Rate der im EKG bestätigten symptomatischen Arrhythmie-Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien) wurde durch die interventionelle Therapie signifikant reduziert (47 versus 59 Prozent). Erneutes Auftreten von symptomatischem Vorhofflimmern wurde bei 41 Prozent (Ablation) und 57 Prozent (Medikation) aller Patienten festgestellt - auch dies ein signifikanter Unterschied zugunsten der Ablation. Auch in puncto Sicherheit schnitt die Ablation gut ab: Die Rate dafür relevanter Ereignisse und Komplikationen betrug 7,7 Prozent, im Vergleich zu 19,5 Prozent in der Gruppe mit Antiarrhythmika. Allerdings sind hier qualitative Unterschiede zu bedenken: Während in der Gruppe mit Ablation Tamponaden das Gros der Komplikationen bildeten, waren es in der Vergleichsgruppe vor allem Therapieabbrüche etwa infolge proarrhythmischer Effekte der Antiarrhythmika. Zu Todesfällen kam es in keiner von beiden Gruppen. Nach Ansicht von Morillo stützen diese Ergebnisse die Strategie, die Radiofrequenz-Ablation mit dem Ziel der Pulmonalvenenisolation künftig als First line therapie Catheter ablation success rates have improved over time based on a better understanding of atrial fibrillation, new techniques and technology, and greater doctor experience. In early studies, the majority of centers reported single procedure success rates of 60% or more for paroxysmal atrial fibrillation and 30% or less for persistent atrial fibrillation. For multiple procedures, the majority reported success rates of 70% or more for paroxysmal atrial fibrillation and 50% or more for persistent atrial fibrillation.1 Outcomes varied based on differences in technique, experience, skill, and follow-up. In 2005, the first worldwide, multicenter survey on catheter ablation was published using data from 181 centers from 1995–2002. It indicated that 52% of patients having an atrial fibrillation catheter ablation were successful and symptom-free without antiarrhythmic drugs. An additional 23.9% were successful but were on antiarrhythmic drugs. For many, those drugs did not work prior to the ablation. Achieving this success required a second procedure for 24.3%, and a third procedure for 3.1%. Success rates were highest in high-volume centers.2 The second worldwide multicenter survey, on catheter ablations performed from 2003–2006, has subsequently been published and showed an improvement in treatment success. The success rate was 70% without antiarrhythmic drugs vs. 52% in the first survey. The overall success rate, which included patients who continued to take antiarrhythmic drugs, was 80% in the second survey vs. 75.5% in the first. What that means is that only 10% of patients in the second survey had to remain on antiarrhythmic drugs vs. 23.9% in the first survey. More than one ablation procedure was needed to achieve these success rates, but the second survey did not indicate what percentage of patients had second and third procedures. When broken down by type of afib, the success rate without antiarrhythmic drugs was 75% for paroxysmal afib, 65% for persistent afib, and 63% for longstanding persistent afib.3 The second worldwide survey showed that doctors were starting to treat more patients with persistent and longstanding persistent atrial fibrillation with catheter ablation. In the first survey, only 53% of centers performed catheter ablation on patients with persistent atrial fibrillation whereas in the second, 86% of centers treated persistent afib. Similarly, only 20% of centers in the first survey treated patients with longstanding persistent atrial fibrillation, which increased to 47% of centers in the second worldwide survey. Since the second worldwide survey used data on procedures only up until 2006, safety and efficacy should be expected to be higher today using current procedures and experience rates, particularly in high-volume centers. Some centers today cite success rates of 80%–85% for first ablations and 95% for second ablations, but there are variances in how different centers measure success. Measuring Catheter Ablation Success The HRS Expert Consensus Statement set guidelines for catheter ablation trials. Immediately after the procedure, there is a three-month "blanking period" during which time atrial fibrillation episodes can occur as part of the body's healing response to the procedure. Any afib activity during that blanking period is not counted in a study's results. After the blanking period, the HRS Expert Consensus Statement defines success as "freedom from afib, atrial flutter or tachycardia" and discontinuation of antiarrhythmic medication. Patients participating in clinical studies should be followed at least 12 months and, at minimum, should have a 24-hour Holter monitor at three months, six months, one year, and two years.1 Not all doctors involved in clinical studies follow the HRS Expert Consensus Statement guidelines, so when looking at treatment success rates, it's important to look at these three factors: How treatment success was defined — Some studies have a strict definition of treatment success—freedom from atrial fibrillation and antiarrhythmic drugs after a single procedure—while others may count as successes patients who remain on antiarrhythmic medication or who have had multiple procedures. How success is defined can be meaningful because if a study shows a 90% success rate, but only 10% of patients were able to stop taking antiarrhythmic drugs, then you might question the effectiveness of the treatment. What type of monitoring was used after treatment — Most studies officially start tracking a patient's heart rhythm three months after a procedure as the first three months are considered a "blanking period". Monitoring methods include patient questionnaires about symptoms, an electrocardiogram (ECG) performed in the doctor's office, a Holter monitor (24-hour, 48-hour, seven-day, or longer), an event monitor, or an implantable loop recorder. An implantable loop recorder (a small device implanted under the skin in the chest area) is the most rigorous follow-up method, and the patient questionnaire is the least. Most studies use a 24- or 48-hour Holter monitor to determine whether atrial fibrillation episodes occur following treatment. What was the length of follow up — Most studies report on treatment successes and failures at one year following the procedure. Generally, success rates that are based on follow up of less than 12 months should be considered preliminary and subject to change as a sizeable percentage of people have an afib recurrence within the first year. In fact, about 30% of patients undergo a second procedure within the first year to treat atrial fibrillation recurrence. Only you can decide what defines treatment success for you. Success may mean freedom from atrial fibrillation and the ability to stop antiarrhythmic medication after one catheter ablation for some people, but for others, alleviation of symptoms, even though they have to remain on antiarrhythmic drugs, may mean success. If you're considering a procedure, ask about the catheter ablation success rate for the specific electrophysiologist and for the center in which it would be done. Also ask about how they define success, such as with or without antiarrhythmic drugs and the number of procedures, and how success is measured, such as by event monitoring, and at what intervals it is measured. It also wouldn't hurt to ask for their success rates and complication rates for the specific technology and tools to be used on you. If you're considering a catheter ablation, you need to know about Catheter Ablation Risks. Radiofrequency (RF) catheter ablation with pulmonary vein isolation is not only safe as a first-line treatment for paroxysmal or persistent atrial fibrillation (AF), it's more likely to suppress AF recurrences than is standard antiarrhythmic drug (AAD) therapy, suggests a randomized trial with a two-year follow-up—one of the longest for an AF-ablation trial [1]. A single ablation procedure reduced the risk of AF recurrence by a significant 44% compared with AAD. Dr Carlos Morillo Importantly, in the second Radiofrequency Ablation vs Antiarrhythmic Drugs as First-Line Therapy of Atrial Fibrillation (RAAFT 2) trial, which followed all patients with transtelephonic monitoring (TTM), RF ablation's significant advantage over AAD was in reducing bouts of AF that were either symptomatic or asymptomatic. "So to be able to claim victory with ablation, you really need to monitor these patients very judiciously," said RAAFT 2 co-principal investigator Dr Carlos Morillo (Hamilton Health Sciences-McMaster University, ON) when presenting the study here at the Heart Rhythm Society 2012 Scientific Sessions. Ablation also significantly cut the frequency of solely symptomatic AF, he said. "These findings support the indication of radiofrequency pulmonary vein isolation as first-line therapy in patients with paroxysmal atrial fibrillation," he said, pointing out that the catheter therapy is currently relegated to second-tier status for paroxysmal AF not responsive to AAD in the most recent Canadian Cardiovascular Society guidelines. US guidelines are even more restrictive. On the other hand, heartwire reported in 2010 that a European Society of Cardiology guidance supports catheter ablation for paroxysmal AF without an AAD attempt. RAAFT 2 shows that catheter ablation as performed in the trial is a good therapy for paroxysmal AF, Morillo told heartwire, but also "that there's still 50% of patients who, after one single ablation, have a recurrence. Still, that's much better than the 72% at two years with antiarrhythmic drugs. So it's much better but still has limitations." RAAFT 2 randomized 127 patients not previously treated with AAD—87.5% with a history of paroxysmal AF and the rest with persistent AF—either to undergo RF ablation within four to six weeks or to initiate AAD, with 90 days allowed for titrating doses. The patients, most from Canada or Germany but also some from Italy, the Czech Republic, and the US, had normal systolic function, and none had hypertension or heart failure. All were followed with TTM. "These were highly symptomatic patients," Morillo said, noting that patients averaged about 47 AF episodes within the previous six months; yet they were low risk for stroke, with CHADS2 scores averaging 0.5 in the ablation group and 0.7 among those getting AAD. In the ablation group, 15.2% required an additional ablation, including one during the initial treatment period and nine during follow-up. Seven patients (10.6%) went on AAD therapy. In the AAD group, 59% had to discontinue at least one antiarrhythmic drug and 29 patients (47.5%) underwent catheter ablation during the follow-up; AAD consisted usually of either flecainide or propafenone (Rythmol, GlaxoSmithKline). Morillo said patients in the trial were "highly committed," with 19% in both groups having been "fully compliant" with TTM (which meant transmissions biweekly and in the event of symptoms). In the ablation group, 86.4% were compliant at least 75% of the time, as were 78.7% of the AAD group. RAAFT-2 primary outcomes: Recurrence rates at two years for symptomatic or asymptomatic AF, atrial flutter, or atrial tachycardia lasting >30 seconds. End point Ablation, n=66 (%) AAD, n=61 (%) HR (95% CI) p Recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.02 Symptomatic recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.03 Symptomatic AF only ( ) 0.01 Recurrence by clinical criteria only ( ) 0.66 "Of note," Morillo said in his presentation, "when we excluded the transtelephonic monitor, we couldn't show any difference in recurrence of the primary outcome, 31% in the antiarrhythmic drug [group] and 24% in the catheter ablation [group], highlighting the need for very strict monitoring in these patients to be able to define a successful outcome." RF ablation also performed better than AAD for the trial's primary safety outcome, a cluster of adverse events specific to each therapy. In the ablation group, 7.7% of patients had an event in the safety cluster, which included death, tamponade, severe pulmonary vein stenosis, thromboembolism, vascular complications, phrenic nerve injury, or compete AV block within 30 days; tamponade accounted for nearly all of it. Of AAD patients, 19.7% experienced an event in the safety cluster, which contained death, torsades de pointes, bradycardia requiring a pacemaker, syncope, QRS-interval prolongation >50% of baseline, atrial flutter, or any other significant event leading to drug withdrawal—which accounted for most of the events. The literature suggests that most patients with paroxysmal AF require more than one ablation to control symptoms, Morillo said, and based on RAAFT 2, it's far more likely to happen within a year of the first ablation. "Actually, we haven't seen many recurring in the second year."
 In die RAAFT-2 benannte randomisierte Studie, die Dr. Carlos Morillo aus Hamilton/Kanada vorgestellt hat, waren 127 relativ junge Patienten mit symptomatischem paroxysmalem (87,5 Prozent) oder persistierendem Vorhofflimmern aufgenommen worden, davon die meisten an Zentren in Kanada und Deutschland. Die Studienteilnehmer, die so gut wie keine kardiovaskulären Begleiterkrankungen und insofern auch ein sehr niedriges Schlaganfallrisiko hatten, waren zuvor nicht mit Antiarrhythmika behandelt worden. Das Studienprotokoll sah vor, dass die der Radiofrequenz-Ablationstherapie zugeteilten Patienten innerhalb von vier bis sechs Wochen dieser Intervention unterzogen werden. In der Vergleichsgruppe mit medikamentöser Therapie gewährte man 90 Tage für die Einstellung auf die gewählten Antiarrhythmika, am häufigsten Flecainid und Propafenon. In der Nachbeobachtung verließ man sich nicht allein auf die Dokumentation symptomatischer Rezidive. Zur Erfassung auch von asymptomatischen Arrhythmie-Rückfällen wurden alle Patienten ab dem dritten Monat mit einem transtelefonischen Monitor (TTM) ausgestattet. Die Nachbeobachtung betrug bis zu zwei Jahre (im Schnitt 21 Monate). Primärer Endpunkt war die in dieser Zeit akkumulierte Rate der per EKG oder TTM objektivierten symptomatischen und asymptomatischen Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien). Arrhythmie-Rezidive signifikant reduziert. Mit 55 Prozent im Vergleich zu 72 Prozent war diese Rate in der Gruppe mit Ablation signifikant niedriger, so das von Morillo präsentierte Hauptergebnis. Die relative Risikoreduktion durch die Ablation gab er mit 46 Prozent an. Auch die Rate der im EKG bestätigten symptomatischen Arrhythmie-Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien) wurde durch die interventionelle Therapie signifikant reduziert (47 versus 59 Prozent). Erneutes Auftreten von symptomatischem Vorhofflimmern wurde bei 41 Prozent (Ablation) und 57 Prozent (Medikation) aller Patienten festgestellt - auch dies ein signifikanter Unterschied zugunsten der Ablation. Auch in puncto Sicherheit schnitt die Ablation gut ab: Die Rate dafür relevanter Ereignisse und Komplikationen betrug 7,7 Prozent, im Vergleich zu 19,5 Prozent in der Gruppe mit Antiarrhythmika. Allerdings sind hier qualitative Unterschiede zu bedenken: Während in der Gruppe mit Ablation Tamponaden das Gros der Komplikationen bildeten, waren es in der Vergleichsgruppe vor allem Therapieabbrüche etwa infolge proarrhythmischer Effekte der Antiarrhythmika. Zu Todesfällen kam es in keiner von beiden Gruppen. Nach Ansicht von Morillo stützen diese Ergebnisse die Strategie, die Radiofrequenz-Ablation mit dem Ziel der Pulmonalvenenisolation künftig als First line therapie. Catheter ablation success rates have improved over time based on a better understanding of atrial fibrillation, new techniques and technology, and greater doctor experience. In early studies, the majority of centers reported single procedure success rates of 60% or more for paroxysmal atrial fibrillation and 30% or less for persistent atrial fibrillation. For multiple procedures, the majority reported success rates of 70% or more for paroxysmal atrial fibrillation and 50% or more for persistent atrial fibrillation.1 Outcomes varied based on differences in technique, experience, skill, and follow-up. In 2005, the first worldwide, multicenter survey on catheter ablation was published using data from 181 centers from 1995–2002. It indicated that 52% of patients having an atrial fibrillation catheter ablation were successful and symptom-free without antiarrhythmic drugs. An additional 23.9% were successful but were on antiarrhythmic drugs. For many, those drugs did not work prior to the ablation. Achieving this success required a second procedure for 24.3%, and a third procedure for 3.1%. Success rates were highest in high-volume centers.2. The second worldwide multicenter survey, on catheter ablations performed from 2003–2006, has subsequently been published and showed an improvement in treatment success. The success rate was 70% without antiarrhythmic drugs vs. 52% in the first survey. The overall success rate, which included patients who continued to take antiarrhythmic drugs, was 80% in the second survey vs. 75.5% in the first. What that means is that only 10% of patients in the second survey had to remain on antiarrhythmic drugs vs. 23.9% in the first survey. More than one ablation procedure was needed to achieve these success rates, but the second survey did not indicate what percentage of patients had second and third procedures. When broken down by type of afib, the success rate without antiarrhythmic drugs was 75% for paroxysmal afib, 65% for persistent afib, and 63% for longstanding persistent afib.3. The second worldwide survey showed that doctors were starting to treat more patients with persistent and longstanding persistent atrial fibrillation with catheter ablation. In the first survey, only 53% of centers performed catheter ablation on patients with persistent atrial fibrillation whereas in the second, 86% of centers treated persistent afib. Similarly, only 20% of centers in the first survey treated patients with longstanding persistent atrial fibrillation, which increased to 47% of centers in the second worldwide survey. Since the second worldwide survey used data on procedures only up until 2006, safety and efficacy should be expected to be higher today using current procedures and experience rates, particularly in high-volume centers. Some centers today cite success rates of 80%–85% for first ablations and 95% for second ablations, but there are variances in how different centers measure success. Measuring Catheter Ablation Success. The HRS Expert Consensus Statement set guidelines for catheter ablation trials. Immediately after the procedure, there is a three-month blanking period during which time atrial fibrillation episodes can occur as part of the body s healing response to the procedure. Any afib activity during that blanking period is not counted in a study s results. After the blanking period, the HRS Expert Consensus Statement defines success as freedom from afib, atrial flutter or tachycardia and discontinuation of antiarrhythmic medication. Patients participating in clinical studies should be followed at least 12 months and, at minimum, should have a 24-hour Holter monitor at three months, six months, one year, and two years.1. Not all doctors involved in clinical studies follow the HRS Expert Consensus Statement guidelines, so when looking at treatment success rates, it s important to look at these three factors: How treatment success was defined — Some studies have a strict definition of treatment success—freedom from atrial fibrillation and antiarrhythmic drugs after a single procedure—while others may count as successes patients who remain on antiarrhythmic medication or who have had multiple procedures. How success is defined can be meaningful because if a study shows a 90% success rate, but only 10% of patients were able to stop taking antiarrhythmic drugs, then you might question the effectiveness of the treatment. What type of monitoring was used after treatment — Most studies officially start tracking a patient s heart rhythm three months after a procedure as the first three months are considered a blanking period . Monitoring methods include patient questionnaires about symptoms, an electrocardiogram (ECG) performed in the doctor s office, a Holter monitor (24-hour, 48-hour, seven-day, or longer), an event monitor, or an implantable loop recorder. An implantable loop recorder (a small device implanted under the skin in the chest area) is the most rigorous follow-up method, and the patient questionnaire is the least. Most studies use a 24- or 48-hour Holter monitor to determine whether atrial fibrillation episodes occur following treatment. What was the length of follow up — Most studies report on treatment successes and failures at one year following the procedure. Generally, success rates that are based on follow up of less than 12 months should be considered preliminary and subject to change as a sizeable percentage of people have an afib recurrence within the first year. In fact, about 30% of patients undergo a second procedure within the first year to treat atrial fibrillation recurrence. Only you can decide what defines treatment success for you. Success may mean freedom from atrial fibrillation and the ability to stop antiarrhythmic medication after one catheter ablation for some people, but for others, alleviation of symptoms, even though they have to remain on antiarrhythmic drugs, may mean success. If you re considering a procedure, ask about the catheter ablation success rate for the specific electrophysiologist and for the center in which it would be done. Also ask about how they define success, such as with or without antiarrhythmic drugs and the number of procedures, and how success is measured, such as by event monitoring, and at what intervals it is measured. It also wouldn t hurt to ask for their success rates and complication rates for the specific technology and tools to be used on you. If you re considering a catheter ablation, you need to know about Catheter Ablation Risks. Radiofrequency (RF) catheter ablation with pulmonary vein isolation is not only safe as a first-line treatment for paroxysmal or persistent atrial fibrillation (AF), it s more likely to suppress AF recurrences than is standard antiarrhythmic drug (AAD) therapy, suggests a randomized trial with a two-year follow-up—one of the longest for an AF-ablation trial [1]. A single ablation procedure reduced the risk of AF recurrence by a significant 44% compared with AAD. Dr Carlos Morillo. Importantly, in the second Radiofrequency Ablation vs Antiarrhythmic Drugs as First-Line Therapy of Atrial Fibrillation (RAAFT 2) trial, which followed all patients with transtelephonic monitoring (TTM), RF ablation s significant advantage over AAD was in reducing bouts of AF that were either symptomatic or asymptomatic. So to be able to claim victory with ablation, you really need to monitor these patients very judiciously, said RAAFT 2 co-principal investigator Dr Carlos Morillo (Hamilton Health Sciences-McMaster University, ON) when presenting the study here at the Heart Rhythm Society 2012 Scientific Sessions. Ablation also significantly cut the frequency of solely symptomatic AF, he said. These findings support the indication of radiofrequency pulmonary vein isolation as first-line therapy in patients with paroxysmal atrial fibrillation, he said, pointing out that the catheter therapy is currently relegated to second-tier status for paroxysmal AF not responsive to AAD in the most recent Canadian Cardiovascular Society guidelines. US guidelines are even more restrictive. On the other hand, heartwire reported in 2010 that a European Society of Cardiology guidance supports catheter ablation for paroxysmal AF without an AAD attempt. RAAFT 2 shows that catheter ablation as performed in the trial is a good therapy for paroxysmal AF, Morillo told heartwire, but also that there s still 50% of patients who, after one single ablation, have a recurrence. Still, that s much better than the 72% at two years with antiarrhythmic drugs. So it s much better but still has limitations. RAAFT 2 randomized 127 patients not previously treated with AAD—87.5% with a history of paroxysmal AF and the rest with persistent AF—either to undergo RF ablation within four to six weeks or to initiate AAD, with 90 days allowed for titrating doses. The patients, most from Canada or Germany but also some from Italy, the Czech Republic, and the US, had normal systolic function, and none had hypertension or heart failure. All were followed with TTM. These were highly symptomatic patients, Morillo said, noting that patients averaged about 47 AF episodes within the previous six months; yet they were low risk for stroke, with CHADS2 scores averaging 0.5 in the ablation group and 0.7 among those getting AAD. In the ablation group, 15.2% required an additional ablation, including one during the initial treatment period and nine during follow-up. Seven patients (10.6%) went on AAD therapy. In the AAD group, 59% had to discontinue at least one antiarrhythmic drug and 29 patients (47.5%) underwent catheter ablation during the follow-up; AAD consisted usually of either flecainide or propafenone (Rythmol, GlaxoSmithKline). Morillo said patients in the trial were highly committed, with 19% in both groups having been fully compliant with TTM (which meant transmissions biweekly and in the event of symptoms). In the ablation group, 86.4% were compliant at least 75% of the time, as were 78.7% of the AAD group. RAAFT-2 primary outcomes: Recurrence rates at two years for symptomatic or asymptomatic AF, atrial flutter, or atrial tachycardia lasting >30 seconds. End point Ablation, n=66 (%) AAD, n=61 (%) HR (95% CI) p Recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.02 Symptomatic recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.03 Symptomatic AF only ( ) 0.01 Recurrence by clinical criteria only ( ) 0.66 Of note, Morillo said in his presentation, when we excluded the transtelephonic monitor, we couldn t show any difference in recurrence of the primary outcome, 31% in the antiarrhythmic drug [group] and 24% in the catheter ablation [group], highlighting the need for very strict monitoring in these patients to be able to define a successful outcome. RF ablation also performed better than AAD for the trial s primary safety outcome, a cluster of adverse events specific to each therapy. In the ablation group, 7.7% of patients had an event in the safety cluster, which included death, tamponade, severe pulmonary vein stenosis, thromboembolism, vascular complications, phrenic nerve injury, or compete AV block within 30 days; tamponade accounted for nearly all of it. Of AAD patients, 19.7% experienced an event in the safety cluster, which contained death, torsades de pointes, bradycardia requiring a pacemaker, syncope, QRS-interval prolongation >50% of baseline, atrial flutter, or any other significant event leading to drug withdrawal—which accounted for most of the events. The literature suggests that most patients with paroxysmal AF require more than one ablation to control symptoms, Morillo said, and based on RAAFT 2, it s far more likely to happen within a year of the first ablation. Actually, we haven t seen many recurring in the second year.")
30
Katheterablation von Vorhofflimmern
Triggermechanismen Mikroreentry- kreise Ganglionäre Plexi Non PV Trigger Schätzungsweise 1 Million Menschen in Deutschland leiden an Vorhofflimmern Das Risiko steigt mit dem Lebensalter • unter 50 Jahre unter 1% • über 60 Jahre 4% - 6% • über 80 Jahre 9% - 16% PV Trigger

31
Neue Ansätze in der Pathophysiologie des Vorhofflimmerns
"The DECAAF results show that stage of atrial fibrosis prior to ablation is a new, powerful, independent predictor of outcome,” said lead investigator Nasir Marrouche, MD, from the CARMA Center at the University of Utah in Salt Lake City, USA."By performing this imaging before ablative treatment we can triage patients according to likelihood of treatment success, and avoid ablative procedures in those patients for whom it is unlikely to work. If a patient has late stage 3 or stage 4 fibrosis their chance of being cured is only 30-35% which is really low, but if they’re in an early stage their chance of cure is 60-80%,” he said.The DECAAF trial included 260 atrial fibrillation (AF) patients with atrial fibrosis who were undergoing ablation. The patients, from 15 centers in USA, Europe and Australia were a mean age of 59 years, and 64.6% of them had paroxysmal AF. High resolution Delayed Enhancement MRI (DE‐MRI) was performed up to 30 days before ablation in all patients to determine the presence and extent of atrial fibrosis, while post- ablation DE-MRI was performed at 90-days follow-up in 177 of the subjects, to determine the extent of residual ablation. At the 90-day follow-up, recurrence of arrhythmia was noted in 88 of the 260 patients (33.8%) based on Holter monitors and electrocardiograms. Multivariate analysis revealed two independent predictors of successful ablation or recurrent symptoms were stage of atrial fibrosis before ablation (P<0.001) as well as residual fibrosis after (P<0.001). Specifically, patients whose pre-ablation fibrosis was stage 1 (defined as less than 10% damaged atrial tissue) had an 85.8% success rate, those with stage 2 (10% - 20% damage) had a 63.3% success rate, those with stage 3 (20% - 30% damage) had a 55% success rate and those with stage 4 (more than 30% damage) had a 31% success rate. For every increased percentage of fibrosis before ablation, there was 6.3% increased risk of recurrent symptoms after ablation (hazard ratio [HR] 1.063), said Dr. Marrouche. Similarly, for every percentage of residual fibrosis there was an 8.2% increased risk of recurrent symptoms (HR 1.082). A secondary finding of the study, based on post-ablation imaging, showed that the type of ablation clinicians used also had an impact on success rates. The choice of procedure was not dictated in the study protocol and was left to the discretion of individual treating physicians. After comparing pre-ablation images of fibrotic tissue, with post-ablation images showing the extent of residual fibrosis, a surprise finding was that pulmonary vein ablation, which is the standard-of-care in atrial fibrillation ablation candidates, is not the best ablative approach, said Dr. Marrouche. “We do ablation around the pulmonary veins because we have assumed for years that the trigger for AF comes from the vein – that’s the standard of care,” he said. “But what we found in DECAAF is that ablation of the veins did not predict outcome. In fact, the most important predictor of outcome, along with stage of atrial fibrosis, was the degree of ablation of the fibrotic tissue. Rather than targeting the pulmonary veins, procedures which ablated fibrotic tissue produced better outcomes - the more that was targeted, the better the outcome.”
 patients with atrial fibrosis who were undergoing ablation. The patients, from 15 centers in USA, Europe and Australia were a mean age of 59 years, and 64.6% of them had paroxysmal AF. High resolution Delayed Enhancement MRI (DE‐MRI) was performed up to 30 days before ablation in all patients to determine the presence and extent of atrial fibrosis, while post- ablation DE-MRI was performed at 90-days follow-up in 177 of the subjects, to determine the extent of residual ablation. At the 90-day follow-up, recurrence of arrhythmia was noted in 88 of the 260 patients (33.8%) based on Holter monitors and electrocardiograms. Multivariate analysis revealed two independent predictors of successful ablation or recurrent symptoms were stage of atrial fibrosis before ablation (P<0.001) as well as residual fibrosis after (P<0.001). Specifically, patients whose pre-ablation fibrosis was stage 1 (defined as less than 10% damaged atrial tissue) had an 85.8% success rate, those with stage 2 (10% - 20% damage) had a 63.3% success rate, those with stage 3 (20% - 30% damage) had a 55% success rate and those with stage 4 (more than 30% damage) had a 31% success rate. For every increased percentage of fibrosis before ablation, there was 6.3% increased risk of recurrent symptoms after ablation (hazard ratio [HR] 1.063), said Dr. Marrouche. Similarly, for every percentage of residual fibrosis there was an 8.2% increased risk of recurrent symptoms (HR 1.082). A secondary finding of the study, based on post-ablation imaging, showed that the type of ablation clinicians used also had an impact on success rates. The choice of procedure was not dictated in the study protocol and was left to the discretion of individual treating physicians. After comparing pre-ablation images of fibrotic tissue, with post-ablation images showing the extent of residual fibrosis, a surprise finding was that pulmonary vein ablation, which is the standard-of-care in atrial fibrillation ablation candidates, is not the best ablative approach, said Dr. Marrouche. We do ablation around the pulmonary veins because we have assumed for years that the trigger for AF comes from the vein – that’s the standard of care, he said. But what we found in DECAAF is that ablation of the veins did not predict outcome. In fact, the most important predictor of outcome, along with stage of atrial fibrosis, was the degree of ablation of the fibrotic tissue. Rather than targeting the pulmonary veins, procedures which ablated fibrotic tissue produced better outcomes - the more that was targeted, the better the outcome.")
33
Treatment of atrial fibrillation by the ablation of localized sources
Focal Imulse and Rotor Mapping = „FIRM“ Mapping Computational maps were analyzed to reveal sustained localized sources of human AF in the form of focal impulse 15, 26 or rotor 6 maps (FIRM) as shown in animal models but not previously in human AF 6, 27. Rotors were identified as rotational activity around a center (using isopotential movies and isochronal activation maps). Focal beats in AF were identified at their point of origin from surrounding diastole from isopotential movies and isochronal maps. We diagnosed rotors or focal beat sources only if sustained throughout several recording epochs (arbitrarily > 50 cycles), to exclude transient rotational and/or centrifugal activation that by definition cannot represent sources but likely represent wavebreak and/or passive activation that are highly variable in fibrillation. Narayan et al; JACC 2012, Vol 60; No 7,
 as shown in animal models but not previously in human AF 6, 27. Rotors were identified as rotational activity around a center. (using isopotential movies and isochronal activation maps). Focal beats in AF were identified at their point of origin from surrounding diastole from isopotential movies and isochronal maps. We diagnosed rotors or focal beat sources only if sustained throughout. several recording epochs (arbitrarily > 50 cycles), to exclude transient rotational and/or centrifugal activation that by definition cannot represent sources but likely represent wavebreak and/or passive activation that are highly variable in fibrillation. Narayan et al; JACC 2012, Vol 60; No 7,")
34
Step 1: Segmentale oder zirkumferenzielle PV Isolation
Stepwise ablation approach für persistierendes und permamentes Vorhofflimmern Haissaguerre J Interv Card Electrophysiol; 2006 Step 1: Segmentale oder zirkumferenzielle PV Isolation Step 2: Ablation einer Dachlinie Afli persistierend Step 3: Ablation im CS und von CFAE Afli persistierend Step 4: Mitralisthmusablation Afli persistierend Step 5: Optional: rechts atrial/SVC Ablation Afli persistierend Step 6: KV und Verifizierung der Lücke Afli persistierend Dr. Michael Müller

35
Techniken der Ablation bei Vorhofflimmern

36
Single procedure sucess rate 57%
Ablation vs antiarrhythmische Therapie Meta analysis, Calkins, Circulation 2009 Katheterablation →63 Studien Antiarrhythmische Therapie →34 Studien Single procedure sucess rate 57% Multiple procedure success rate off AAD 71% Multiple procedure success rate on AAD 77% Success rate for AAD 52% 17% ≥ 2 procedures Sixty-three RFA and 34 AAD studies were included in the reviews. Patients enrolled in RFA studies tended to be younger (mean age, 55 versus 62 years), had longer duration of atrial fibrillation (6.0 versus 3.1 years), and had failed a greater number of prior drug trials (2.6 versus 1.7). The single-procedure success rate of ablation off AAD therapy was 57% (95% CI, 50% to 64%), the multiple procedure success rate off AAD was 71% (95% CI, 65% to 77%), and the multiple procedure success rate on AAD or with unknown AAD usage was 77% (95% CI, 73% to 81%). In comparison, the success rate for AAD therapy was 52% (95% CI, 47% to 57%). A major complication of catheter ablation occurred in 4.9% of patients. Adverse events for AAD studies, although more common (30% versus 5%), were less severe. Conclusions— Studies of RFA for treatment of atrial fibrillation report higher efficacy rates than do studies of AAD therapy and a lower rate of complications. In 2005, the first worldwide, multicenter survey on catheter ablation was published using data from 181 centers from 1995–2002. It indicated that 52% of patients having an atrial fibrillation catheter ablation were successful and symptom-free without antiarrhythmic drugs. An additional 23.9% were successful but were on antiarrhythmic drugs. For many, those drugs did not work prior to the ablation. Achieving this success required a second procedure for 24.3%, and a third procedure for 3.1%. Success rates were highest in high-volume centers.2 The second worldwide multicenter survey, on catheter ablations performed from 2003–2006, has subsequently been published and showed an improvement in treatment success. The success rate was 70% without antiarrhythmic drugs vs. 52% in the first survey. The overall success rate, which included patients who continued to take antiarrhythmic drugs, was 80% in the second survey vs. 75.5% in the first. What that means is that only 10% of patients in the second survey had to remain on antiarrhythmic drugs vs. 23.9% in the first survey. More than one ablation procedure was needed to achieve these success rates, but the second survey did not indicate what percentage of patients had second and third procedures. When broken down by type of afib, the success rate without antiarrhythmic drugs was 75% for paroxysmal afib, 65% for persistent afib, and 63% for longstanding persistent afib.3 The second worldwide survey showed that doctors were starting to treat more patients with persistent and longstanding persistent atrial fibrillation with catheter ablation. In the first survey, only 53% of centers performed catheter ablation on patients with persistent atrial fibrillation whereas in the second, 86% of centers treated persistent afib. Similarly, only 20% of centers in the first survey treated patients with longstanding persistent atrial fibrillation, which increased to 47% of centers in the second worldwide survey. Since the second worldwide survey used data on procedures only up until 2006, safety and efficacy should be expected to be higher today using current procedures and experience rates, particularly in high-volume centers. Some centers today cite success rates of 80%–85% for first ablations and 95% for second ablations, but there are variances in how different centers measure success. Measuring Catheter Ablation Success The HRS Expert Consensus Statement set guidelines for catheter ablation trials. Immediately after the procedure, there is a three-month "blanking period" during which time atrial fibrillation episodes can occur as part of the body's healing response to the procedure. Any afib activity during that blanking period is not counted in a study's results. After the blanking period, the HRS Expert Consensus Statement defines success as "freedom from afib, atrial flutter or tachycardia" and discontinuation of antiarrhythmic medication. Patients participating in clinical studies should be followed at least 12 months and, at minimum, should have a 24-hour Holter monitor at three months, six months, one year, and two years.1 Not all doctors involved in clinical studies follow the HRS Expert Consensus Statement guidelines, so when looking at treatment success rates, it's important to look at these three factors: How treatment success was defined — Some studies have a strict definition of treatment success—freedom from atrial fibrillation and antiarrhythmic drugs after a single procedure—while others may count as successes patients who remain on antiarrhythmic medication or who have had multiple procedures. How success is defined can be meaningful because if a study shows a 90% success rate, but only 10% of patients were able to stop taking antiarrhythmic drugs, then you might question the effectiveness of the treatment. What type of monitoring was used after treatment — Most studies officially start tracking a patient's heart rhythm three months after a procedure as the first three months are considered a "blanking period". Monitoring methods include patient questionnaires about symptoms, an electrocardiogram (ECG) performed in the doctor's office, a Holter monitor (24-hour, 48-hour, seven-day, or longer), an event monitor, or an implantable loop recorder. An implantable loop recorder (a small device implanted under the skin in the chest area) is the most rigorous follow-up method, and the patient questionnaire is the least. Most studies use a 24- or 48-hour Holter monitor to determine whether atrial fibrillation episodes occur following treatment. What was the length of follow up — Most studies report on treatment successes and failures at one year following the procedure. Generally, success rates that are based on follow up of less than 12 months should be considered preliminary and subject to change as a sizeable percentage of people have an afib recurrence within the first year. In fact, about 30% of patients undergo a second procedure within the first year to treat atrial fibrillation recurrence. Only you can decide what defines treatment success for you. Success may mean freedom from atrial fibrillation and the ability to stop antiarrhythmic medication after one catheter ablation for some people, but for others, alleviation of symptoms, even though they have to remain on antiarrhythmic drugs, may mean success. If you're considering a procedure, ask about the catheter ablation success rate for the specific electrophysiologist and for the center in which it would be done. Also ask about how they define success, such as with or without antiarrhythmic drugs and the number of procedures, and how success is measured, such as by event monitoring, and at what intervals it is measured. It also wouldn't hurt to ask for their success rates and complication rates for the specific technology and tools to be used on you. If you're considering a catheter ablation, you need to know about Catheter Ablation Risks. Radiofrequency (RF) catheter ablation with pulmonary vein isolation is not only safe as a first-line treatment for paroxysmal or persistent atrial fibrillation (AF), it's more likely to suppress AF recurrences than is standard antiarrhythmic drug (AAD) therapy, suggests a randomized trial with a two-year follow-up—one of the longest for an AF-ablation trial [1]. A single ablation procedure reduced the risk of AF recurrence by a significant 44% compared with AAD. Dr Carlos Morillo Importantly, in the second Radiofrequency Ablation vs Antiarrhythmic Drugs as First-Line Therapy of Atrial Fibrillation (RAAFT 2) trial, which followed all patients with transtelephonic monitoring (TTM), RF ablation's significant advantage over AAD was in reducing bouts of AF that were either symptomatic or asymptomatic. "So to be able to claim victory with ablation, you really need to monitor these patients very judiciously," said RAAFT 2 co-principal investigator Dr Carlos Morillo (Hamilton Health Sciences-McMaster University, ON) when presenting the study here at the Heart Rhythm Society 2012 Scientific Sessions. Ablation also significantly cut the frequency of solely symptomatic AF, he said. "These findings support the indication of radiofrequency pulmonary vein isolation as first-line therapy in patients with paroxysmal atrial fibrillation," he said, pointing out that the catheter therapy is currently relegated to second-tier status for paroxysmal AF not responsive to AAD in the most recent Canadian Cardiovascular Society guidelines. US guidelines are even more restrictive. On the other hand, heartwire reported in 2010 that a European Society of Cardiology guidance supports catheter ablation for paroxysmal AF without an AAD attempt. RAAFT 2 shows that catheter ablation as performed in the trial is a good therapy for paroxysmal AF, Morillo told heartwire, but also "that there's still 50% of patients who, after one single ablation, have a recurrence. Still, that's much better than the 72% at two years with antiarrhythmic drugs. So it's much better but still has limitations." RAAFT 2 randomized 127 patients not previously treated with AAD—87.5% with a history of paroxysmal AF and the rest with persistent AF—either to undergo RF ablation within four to six weeks or to initiate AAD, with 90 days allowed for titrating doses. The patients, most from Canada or Germany but also some from Italy, the Czech Republic, and the US, had normal systolic function, and none had hypertension or heart failure. All were followed with TTM. "These were highly symptomatic patients," Morillo said, noting that patients averaged about 47 AF episodes within the previous six months; yet they were low risk for stroke, with CHADS2 scores averaging 0.5 in the ablation group and 0.7 among those getting AAD. In the ablation group, 15.2% required an additional ablation, including one during the initial treatment period and nine during follow-up. Seven patients (10.6%) went on AAD therapy. In the AAD group, 59% had to discontinue at least one antiarrhythmic drug and 29 patients (47.5%) underwent catheter ablation during the follow-up; AAD consisted usually of either flecainide or propafenone (Rythmol, GlaxoSmithKline). Morillo said patients in the trial were "highly committed," with 19% in both groups having been "fully compliant" with TTM (which meant transmissions biweekly and in the event of symptoms). In the ablation group, 86.4% were compliant at least 75% of the time, as were 78.7% of the AAD group. RAAFT-2 primary outcomes: Recurrence rates at two years for symptomatic or asymptomatic AF, atrial flutter, or atrial tachycardia lasting >30 seconds. End point Ablation, n=66 (%) AAD, n=61 (%) HR (95% CI) p Recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.02 Symptomatic recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.03 Symptomatic AF only ( ) 0.01 Recurrence by clinical criteria only ( ) 0.66 "Of note," Morillo said in his presentation, "when we excluded the transtelephonic monitor, we couldn't show any difference in recurrence of the primary outcome, 31% in the antiarrhythmic drug [group] and 24% in the catheter ablation [group], highlighting the need for very strict monitoring in these patients to be able to define a successful outcome." RF ablation also performed better than AAD for the trial's primary safety outcome, a cluster of adverse events specific to each therapy. In the ablation group, 7.7% of patients had an event in the safety cluster, which included death, tamponade, severe pulmonary vein stenosis, thromboembolism, vascular complications, phrenic nerve injury, or compete AV block within 30 days; tamponade accounted for nearly all of it. Of AAD patients, 19.7% experienced an event in the safety cluster, which contained death, torsades de pointes, bradycardia requiring a pacemaker, syncope, QRS-interval prolongation >50% of baseline, atrial flutter, or any other significant event leading to drug withdrawal—which accounted for most of the events. The literature suggests that most patients with paroxysmal AF require more than one ablation to control symptoms, Morillo said, and based on RAAFT 2, it's far more likely to happen within a year of the first ablation. "Actually, we haven't seen many recurring in the second year."
, had longer duration of atrial fibrillation (6.0 versus 3.1 years), and had failed a greater number of prior drug trials (2.6 versus 1.7). The single-procedure success rate of ablation off AAD therapy was 57% (95% CI, 50% to 64%), the multiple procedure success rate off AAD was 71% (95% CI, 65% to 77%), and the multiple procedure success rate on AAD or with unknown AAD usage was 77% (95% CI, 73% to 81%). In comparison, the success rate for AAD therapy was 52% (95% CI, 47% to 57%). A major complication of catheter ablation occurred in 4.9% of patients. Adverse events for AAD studies, although more common (30% versus 5%), were less severe. Conclusions— Studies of RFA for treatment of atrial fibrillation report higher efficacy rates than do studies of AAD therapy and a lower rate of complications. In 2005, the first worldwide, multicenter survey on catheter ablation was published using data from 181 centers from 1995–2002. It indicated that 52% of patients having an atrial fibrillation catheter ablation were successful and symptom-free without antiarrhythmic drugs. An additional 23.9% were successful but were on antiarrhythmic drugs. For many, those drugs did not work prior to the ablation. Achieving this success required a second procedure for 24.3%, and a third procedure for 3.1%. Success rates were highest in high-volume centers.2. The second worldwide multicenter survey, on catheter ablations performed from 2003–2006, has subsequently been published and showed an improvement in treatment success. The success rate was 70% without antiarrhythmic drugs vs. 52% in the first survey. The overall success rate, which included patients who continued to take antiarrhythmic drugs, was 80% in the second survey vs. 75.5% in the first. What that means is that only 10% of patients in the second survey had to remain on antiarrhythmic drugs vs. 23.9% in the first survey. More than one ablation procedure was needed to achieve these success rates, but the second survey did not indicate what percentage of patients had second and third procedures. When broken down by type of afib, the success rate without antiarrhythmic drugs was 75% for paroxysmal afib, 65% for persistent afib, and 63% for longstanding persistent afib.3. The second worldwide survey showed that doctors were starting to treat more patients with persistent and longstanding persistent atrial fibrillation with catheter ablation. In the first survey, only 53% of centers performed catheter ablation on patients with persistent atrial fibrillation whereas in the second, 86% of centers treated persistent afib. Similarly, only 20% of centers in the first survey treated patients with longstanding persistent atrial fibrillation, which increased to 47% of centers in the second worldwide survey. Since the second worldwide survey used data on procedures only up until 2006, safety and efficacy should be expected to be higher today using current procedures and experience rates, particularly in high-volume centers. Some centers today cite success rates of 80%–85% for first ablations and 95% for second ablations, but there are variances in how different centers measure success. Measuring Catheter Ablation Success. The HRS Expert Consensus Statement set guidelines for catheter ablation trials. Immediately after the procedure, there is a three-month blanking period during which time atrial fibrillation episodes can occur as part of the body s healing response to the procedure. Any afib activity during that blanking period is not counted in a study s results. After the blanking period, the HRS Expert Consensus Statement defines success as freedom from afib, atrial flutter or tachycardia and discontinuation of antiarrhythmic medication. Patients participating in clinical studies should be followed at least 12 months and, at minimum, should have a 24-hour Holter monitor at three months, six months, one year, and two years.1. Not all doctors involved in clinical studies follow the HRS Expert Consensus Statement guidelines, so when looking at treatment success rates, it s important to look at these three factors: How treatment success was defined — Some studies have a strict definition of treatment success—freedom from atrial fibrillation and antiarrhythmic drugs after a single procedure—while others may count as successes patients who remain on antiarrhythmic medication or who have had multiple procedures. How success is defined can be meaningful because if a study shows a 90% success rate, but only 10% of patients were able to stop taking antiarrhythmic drugs, then you might question the effectiveness of the treatment. What type of monitoring was used after treatment — Most studies officially start tracking a patient s heart rhythm three months after a procedure as the first three months are considered a blanking period . Monitoring methods include patient questionnaires about symptoms, an electrocardiogram (ECG) performed in the doctor s office, a Holter monitor (24-hour, 48-hour, seven-day, or longer), an event monitor, or an implantable loop recorder. An implantable loop recorder (a small device implanted under the skin in the chest area) is the most rigorous follow-up method, and the patient questionnaire is the least. Most studies use a 24- or 48-hour Holter monitor to determine whether atrial fibrillation episodes occur following treatment. What was the length of follow up — Most studies report on treatment successes and failures at one year following the procedure. Generally, success rates that are based on follow up of less than 12 months should be considered preliminary and subject to change as a sizeable percentage of people have an afib recurrence within the first year. In fact, about 30% of patients undergo a second procedure within the first year to treat atrial fibrillation recurrence. Only you can decide what defines treatment success for you. Success may mean freedom from atrial fibrillation and the ability to stop antiarrhythmic medication after one catheter ablation for some people, but for others, alleviation of symptoms, even though they have to remain on antiarrhythmic drugs, may mean success. If you re considering a procedure, ask about the catheter ablation success rate for the specific electrophysiologist and for the center in which it would be done. Also ask about how they define success, such as with or without antiarrhythmic drugs and the number of procedures, and how success is measured, such as by event monitoring, and at what intervals it is measured. It also wouldn t hurt to ask for their success rates and complication rates for the specific technology and tools to be used on you. If you re considering a catheter ablation, you need to know about Catheter Ablation Risks. Radiofrequency (RF) catheter ablation with pulmonary vein isolation is not only safe as a first-line treatment for paroxysmal or persistent atrial fibrillation (AF), it s more likely to suppress AF recurrences than is standard antiarrhythmic drug (AAD) therapy, suggests a randomized trial with a two-year follow-up—one of the longest for an AF-ablation trial [1]. A single ablation procedure reduced the risk of AF recurrence by a significant 44% compared with AAD. Dr Carlos Morillo. Importantly, in the second Radiofrequency Ablation vs Antiarrhythmic Drugs as First-Line Therapy of Atrial Fibrillation (RAAFT 2) trial, which followed all patients with transtelephonic monitoring (TTM), RF ablation s significant advantage over AAD was in reducing bouts of AF that were either symptomatic or asymptomatic. So to be able to claim victory with ablation, you really need to monitor these patients very judiciously, said RAAFT 2 co-principal investigator Dr Carlos Morillo (Hamilton Health Sciences-McMaster University, ON) when presenting the study here at the Heart Rhythm Society 2012 Scientific Sessions. Ablation also significantly cut the frequency of solely symptomatic AF, he said. These findings support the indication of radiofrequency pulmonary vein isolation as first-line therapy in patients with paroxysmal atrial fibrillation, he said, pointing out that the catheter therapy is currently relegated to second-tier status for paroxysmal AF not responsive to AAD in the most recent Canadian Cardiovascular Society guidelines. US guidelines are even more restrictive. On the other hand, heartwire reported in 2010 that a European Society of Cardiology guidance supports catheter ablation for paroxysmal AF without an AAD attempt. RAAFT 2 shows that catheter ablation as performed in the trial is a good therapy for paroxysmal AF, Morillo told heartwire, but also that there s still 50% of patients who, after one single ablation, have a recurrence. Still, that s much better than the 72% at two years with antiarrhythmic drugs. So it s much better but still has limitations. RAAFT 2 randomized 127 patients not previously treated with AAD—87.5% with a history of paroxysmal AF and the rest with persistent AF—either to undergo RF ablation within four to six weeks or to initiate AAD, with 90 days allowed for titrating doses. The patients, most from Canada or Germany but also some from Italy, the Czech Republic, and the US, had normal systolic function, and none had hypertension or heart failure. All were followed with TTM. These were highly symptomatic patients, Morillo said, noting that patients averaged about 47 AF episodes within the previous six months; yet they were low risk for stroke, with CHADS2 scores averaging 0.5 in the ablation group and 0.7 among those getting AAD. In the ablation group, 15.2% required an additional ablation, including one during the initial treatment period and nine during follow-up. Seven patients (10.6%) went on AAD therapy. In the AAD group, 59% had to discontinue at least one antiarrhythmic drug and 29 patients (47.5%) underwent catheter ablation during the follow-up; AAD consisted usually of either flecainide or propafenone (Rythmol, GlaxoSmithKline). Morillo said patients in the trial were highly committed, with 19% in both groups having been fully compliant with TTM (which meant transmissions biweekly and in the event of symptoms). In the ablation group, 86.4% were compliant at least 75% of the time, as were 78.7% of the AAD group. RAAFT-2 primary outcomes: Recurrence rates at two years for symptomatic or asymptomatic AF, atrial flutter, or atrial tachycardia lasting >30 seconds. End point Ablation, n=66 (%) AAD, n=61 (%) HR (95% CI) p Recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.02 Symptomatic recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.03 Symptomatic AF only ( ) 0.01 Recurrence by clinical criteria only ( ) 0.66 Of note, Morillo said in his presentation, when we excluded the transtelephonic monitor, we couldn t show any difference in recurrence of the primary outcome, 31% in the antiarrhythmic drug [group] and 24% in the catheter ablation [group], highlighting the need for very strict monitoring in these patients to be able to define a successful outcome. RF ablation also performed better than AAD for the trial s primary safety outcome, a cluster of adverse events specific to each therapy. In the ablation group, 7.7% of patients had an event in the safety cluster, which included death, tamponade, severe pulmonary vein stenosis, thromboembolism, vascular complications, phrenic nerve injury, or compete AV block within 30 days; tamponade accounted for nearly all of it. Of AAD patients, 19.7% experienced an event in the safety cluster, which contained death, torsades de pointes, bradycardia requiring a pacemaker, syncope, QRS-interval prolongation >50% of baseline, atrial flutter, or any other significant event leading to drug withdrawal—which accounted for most of the events. The literature suggests that most patients with paroxysmal AF require more than one ablation to control symptoms, Morillo said, and based on RAAFT 2, it s far more likely to happen within a year of the first ablation. Actually, we haven t seen many recurring in the second year.")
37
Ablation bei paroxysmalem Vorhofflimmern
5 – Jahreserfolg N = 161, paroxysmales Vorhofflimmern, normale LV Funktion Nach 1 Ablation Nach letzter Ablation Long-Term Results of Catheter Ablation in Paroxysmal Atrial Fibrillation Lessons From a 5-Year Follow-Up Feifan Ouyang, MD*; Roland Tilz, MD*; Julian Chun, MD; Boris Schmidt, MD; Erik Wissner, MD; Thomas Zerm, MD; Kars Neven, MD; Bulent Köktürk, MD; Melanie Konstantinidou, MD; Andreas Metzner, MD; Alexander Fuernkranz, MD Karl-Heinz Kuck, MD From the II Med. Abteilung, Asklepios Klinik St. Georg, Hamburg, Germany. Correspondence to Feifan Ouyang, MD, II Med. Abteilung, Allgemeines Krankenhaus St. Georg, Lohm hlenstrasse 5, Hamburg, Germany. Background— Paroxysmal atrial fibrillation (AF) naturally progresses toward chronic AF at an estimated rate of 15% to 30% over a 1- to 3-year period. Pulmonary vein (PV) isolation is increasingly performed for the treatment of drug-refractory paroxysmal AF. The long-term data on clinical outcome after circumferential PV isolation are limited. Methods and Results— From 2003 to late 2004, 161 patients (121 men; age, 59.8±9.7 years) with symptomatic paroxysmal AF and normal left ventricular function underwent circumferential PV isolation guided by 3-dimensional mapping and double Lasso technique. Right-sided and left-sided continuous circular lesions encircling the ipsilateral PVs were placed with irrigated radiofrequency energy. The procedure end point was the absence of all PV spikes for at least 30 minutes after PV isolation verified by 2 Lasso catheters placed within the ipsilateral PVs. Sinus rhythm was present in 75 patients (46.6%) after the initial procedure during a median follow-up period of 4.8 years (0.33 to 5.5 years). A second procedure was performed in 66 and a third procedure in 12 patients. Recovered PV isolation conduction was observed in 62 of 66 patients (94.0%) during the second and in 8 of 12 patients (66.7%) during the third procedure. After a median of 1 (1 to 3) procedure, stable sinus rhythm was achieved in 128 of 161 patients (79.5%), whereas clinical improvement occurred in an additional 21 of 161 patients (13.0%) during a median follow-up of 4.6 years (0.33 to 5.5 years). Four patients in stable sinus rhythm died during follow-up. Progression toward chronic AF was observed in 4 patients (2.4%); however, only 2 patients reported symptoms. Conclusion— In patients with paroxysmal AF and normal left ventricular function, circumferential PV isolation results in stable sinus rhythm in the majority of patients, and low incidence of chronic AF was observed after ablation during up to 5 years of follow-up. Sinusrhythmus: 46,6% Sinusrhythmus: 79,7% 41% ≥ 2 Ablationen Ouyang et al. Circulation 2010;122:2368
 naturally progresses toward chronic AF at an estimated rate of 15% to 30% over a 1- to 3-year period. Pulmonary vein (PV) isolation is increasingly performed for the treatment of drug-refractory paroxysmal AF. The long-term data on clinical outcome after circumferential PV isolation are limited. Methods and Results— From 2003 to late 2004, 161 patients (121 men; age, 59.8±9.7 years) with symptomatic paroxysmal AF and normal left ventricular function underwent circumferential PV isolation guided by 3-dimensional mapping and double Lasso technique. Right-sided and left-sided continuous circular lesions encircling the ipsilateral PVs were placed with irrigated radiofrequency energy. The procedure end point was the absence of all PV spikes for at least 30 minutes after PV isolation verified by 2 Lasso catheters placed within the ipsilateral PVs. Sinus rhythm was present in 75 patients (46.6%) after the initial procedure during a median follow-up period of 4.8 years (0.33 to 5.5 years). A second procedure was performed in 66 and a third procedure in 12 patients. Recovered PV isolation conduction was observed in 62 of 66 patients (94.0%) during the second and in 8 of 12 patients (66.7%) during the third procedure. After a median of 1 (1 to 3) procedure, stable sinus rhythm was achieved in 128 of 161 patients (79.5%), whereas clinical improvement occurred in an additional 21 of 161 patients (13.0%) during a median follow-up of 4.6 years (0.33 to 5.5 years). Four patients in stable sinus rhythm died during follow-up. Progression toward chronic AF was observed in 4 patients (2.4%); however, only 2 patients reported symptoms. Conclusion— In patients with paroxysmal AF and normal left ventricular function, circumferential PV isolation results in stable sinus rhythm in the majority of patients, and low incidence of chronic AF was observed after ablation during up to 5 years of follow-up. Sinusrhythmus: 46,6% Sinusrhythmus: 79,7% 41% ≥ 2 Ablationen. Ouyang et al. Circulation 2010;122:2368.")
38
Update Worldwide Survey on Catheter Ablation of atrial fibrillation
Update Worldwide Survey on Catheter Ablation of atrial fibrillation. Cappato et al; CircEP 2010 Die kathetergestützte Ablationstherapie als Methode zur Rhythmuskontrolle bei Vorhofflimmern durchläuft derzeit eine rasante Entwicklung. Ziel der Ablation ist, Trigger des Vorhofflimmerns zu eliminieren oder vom arrhythmogenen Substrat zu trennen und/oder dieses Substrat so zu verändern, dass sich die Arrhythmie nicht mehr ausbreiten kann. Das geschieht heute am häufigsten durch die Pulmonalvenenisolation. Die meisten Leitlinien sind bezüglich der Ablationstherapie noch eher restriktiv. Empfohlen wird sie in der Regel bei symptomatischen Patienten, bei denen mindestens ein vorangegangener Therapieversuch mit Antiarrhythmika nicht erfolgreich war. Einzig die 2010 aktualisierten europäischen Leitlinien gehen schon einen kleinen Schritt weiter: Danach kommt in ausgewählten Einzelfällen nach Absprache mit dem Patienten die Katheterablation als Rhythmus erhaltende Behandlung der ersten Wahl schon heute in Betracht. Ein Kollektiv von relativ gesunden Patienten Diese noch sehr vorsichtige Empfehlung (Empfehlungsgrad IIb) wird demnächst wohl mit mehr Nachdruck formuliert werden können. Denn aktuell beim Kongress "Heart Rhythm 2012" in Boston vorgestellte neue Studiendaten stärken der Ablationstherapie als First-Line-Option klar den Rücken. In die RAAFT-2 benannte randomisierte Studie, die Dr. Carlos Morillo aus Hamilton/Kanada vorgestellt hat, waren 127 relativ junge Patienten mit symptomatischem paroxysmalem (87,5 Prozent) oder persistierendem Vorhofflimmern aufgenommen worden, davon die meisten an Zentren in Kanada und Deutschland. Die Studienteilnehmer, die so gut wie keine kardiovaskulären Begleiterkrankungen und insofern auch ein sehr niedriges Schlaganfallrisiko hatten, waren zuvor nicht mit Antiarrhythmika behandelt worden. Das Studienprotokoll sah vor, dass die der Radiofrequenz-Ablationstherapie zugeteilten Patienten innerhalb von vier bis sechs Wochen dieser Intervention unterzogen werden. In der Vergleichsgruppe mit medikamentöser Therapie gewährte man 90 Tage für die Einstellung auf die gewählten Antiarrhythmika, am häufigsten Flecainid und Propafenon. In der Nachbeobachtung verließ man sich nicht allein auf die Dokumentation symptomatischer Rezidive. Zur Erfassung auch von asymptomatischen Arrhythmie-Rückfällen wurden alle Patienten ab dem dritten Monat mit einem transtelefonischen Monitor (TTM) ausgestattet. Die Nachbeobachtung betrug bis zu zwei Jahre (im Schnitt 21 Monate). Primärer Endpunkt war die in dieser Zeit akkumulierte Rate der per EKG oder TTM objektivierten symptomatischen und asymptomatischen Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien). Arrhythmie-Rezidive signifikant reduziert Mit 55 Prozent im Vergleich zu 72 Prozent war diese Rate in der Gruppe mit Ablation signifikant niedriger, so das von Morillo präsentierte Hauptergebnis. Die relative Risikoreduktion durch die Ablation gab er mit 46 Prozent an. Auch die Rate der im EKG bestätigten symptomatischen Arrhythmie-Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien) wurde durch die interventionelle Therapie signifikant reduziert (47 versus 59 Prozent). Erneutes Auftreten von symptomatischem Vorhofflimmern wurde bei 41 Prozent (Ablation) und 57 Prozent (Medikation) aller Patienten festgestellt - auch dies ein signifikanter Unterschied zugunsten der Ablation. Auch in puncto Sicherheit schnitt die Ablation gut ab: Die Rate dafür relevanter Ereignisse und Komplikationen betrug 7,7 Prozent, im Vergleich zu 19,5 Prozent in der Gruppe mit Antiarrhythmika. Allerdings sind hier qualitative Unterschiede zu bedenken: Während in der Gruppe mit Ablation Tamponaden das Gros der Komplikationen bildeten, waren es in der Vergleichsgruppe vor allem Therapieabbrüche etwa infolge proarrhythmischer Effekte der Antiarrhythmika. Zu Todesfällen kam es in keiner von beiden Gruppen. Nach Ansicht von Morillo stützen diese Ergebnisse die Strategie, die Radiofrequenz-Ablation mit dem Ziel der Pulmonalvenenisolation künftig als First line therapie Catheter ablation success rates have improved over time based on a better understanding of atrial fibrillation, new techniques and technology, and greater doctor experience. In early studies, the majority of centers reported single procedure success rates of 60% or more for paroxysmal atrial fibrillation and 30% or less for persistent atrial fibrillation. For multiple procedures, the majority reported success rates of 70% or more for paroxysmal atrial fibrillation and 50% or more for persistent atrial fibrillation.1 Outcomes varied based on differences in technique, experience, skill, and follow-up. In 2005, the first worldwide, multicenter survey on catheter ablation was published using data from 181 centers from 1995–2002. It indicated that 52% of patients having an atrial fibrillation catheter ablation were successful and symptom-free without antiarrhythmic drugs. An additional 23.9% were successful but were on antiarrhythmic drugs. For many, those drugs did not work prior to the ablation. Achieving this success required a second procedure for 24.3%, and a third procedure for 3.1%. Success rates were highest in high-volume centers.2 The second worldwide multicenter survey, on catheter ablations performed from 2003–2006, has subsequently been published and showed an improvement in treatment success. The success rate was 70% without antiarrhythmic drugs vs. 52% in the first survey. The overall success rate, which included patients who continued to take antiarrhythmic drugs, was 80% in the second survey vs. 75.5% in the first. What that means is that only 10% of patients in the second survey had to remain on antiarrhythmic drugs vs. 23.9% in the first survey. More than one ablation procedure was needed to achieve these success rates, but the second survey did not indicate what percentage of patients had second and third procedures. When broken down by type of afib, the success rate without antiarrhythmic drugs was 75% for paroxysmal afib, 65% for persistent afib, and 63% for longstanding persistent afib.3 The second worldwide survey showed that doctors were starting to treat more patients with persistent and longstanding persistent atrial fibrillation with catheter ablation. In the first survey, only 53% of centers performed catheter ablation on patients with persistent atrial fibrillation whereas in the second, 86% of centers treated persistent afib. Similarly, only 20% of centers in the first survey treated patients with longstanding persistent atrial fibrillation, which increased to 47% of centers in the second worldwide survey. Since the second worldwide survey used data on procedures only up until 2006, safety and efficacy should be expected to be higher today using current procedures and experience rates, particularly in high-volume centers. Some centers today cite success rates of 80%–85% for first ablations and 95% for second ablations, but there are variances in how different centers measure success. Measuring Catheter Ablation Success The HRS Expert Consensus Statement set guidelines for catheter ablation trials. Immediately after the procedure, there is a three-month "blanking period" during which time atrial fibrillation episodes can occur as part of the body's healing response to the procedure. Any afib activity during that blanking period is not counted in a study's results. After the blanking period, the HRS Expert Consensus Statement defines success as "freedom from afib, atrial flutter or tachycardia" and discontinuation of antiarrhythmic medication. Patients participating in clinical studies should be followed at least 12 months and, at minimum, should have a 24-hour Holter monitor at three months, six months, one year, and two years.1 Not all doctors involved in clinical studies follow the HRS Expert Consensus Statement guidelines, so when looking at treatment success rates, it's important to look at these three factors: How treatment success was defined — Some studies have a strict definition of treatment success—freedom from atrial fibrillation and antiarrhythmic drugs after a single procedure—while others may count as successes patients who remain on antiarrhythmic medication or who have had multiple procedures. How success is defined can be meaningful because if a study shows a 90% success rate, but only 10% of patients were able to stop taking antiarrhythmic drugs, then you might question the effectiveness of the treatment. What type of monitoring was used after treatment — Most studies officially start tracking a patient's heart rhythm three months after a procedure as the first three months are considered a "blanking period". Monitoring methods include patient questionnaires about symptoms, an electrocardiogram (ECG) performed in the doctor's office, a Holter monitor (24-hour, 48-hour, seven-day, or longer), an event monitor, or an implantable loop recorder. An implantable loop recorder (a small device implanted under the skin in the chest area) is the most rigorous follow-up method, and the patient questionnaire is the least. Most studies use a 24- or 48-hour Holter monitor to determine whether atrial fibrillation episodes occur following treatment. What was the length of follow up — Most studies report on treatment successes and failures at one year following the procedure. Generally, success rates that are based on follow up of less than 12 months should be considered preliminary and subject to change as a sizeable percentage of people have an afib recurrence within the first year. In fact, about 30% of patients undergo a second procedure within the first year to treat atrial fibrillation recurrence. Only you can decide what defines treatment success for you. Success may mean freedom from atrial fibrillation and the ability to stop antiarrhythmic medication after one catheter ablation for some people, but for others, alleviation of symptoms, even though they have to remain on antiarrhythmic drugs, may mean success. If you're considering a procedure, ask about the catheter ablation success rate for the specific electrophysiologist and for the center in which it would be done. Also ask about how they define success, such as with or without antiarrhythmic drugs and the number of procedures, and how success is measured, such as by event monitoring, and at what intervals it is measured. It also wouldn't hurt to ask for their success rates and complication rates for the specific technology and tools to be used on you. If you're considering a catheter ablation, you need to know about Catheter Ablation Risks. Radiofrequency (RF) catheter ablation with pulmonary vein isolation is not only safe as a first-line treatment for paroxysmal or persistent atrial fibrillation (AF), it's more likely to suppress AF recurrences than is standard antiarrhythmic drug (AAD) therapy, suggests a randomized trial with a two-year follow-up—one of the longest for an AF-ablation trial [1]. A single ablation procedure reduced the risk of AF recurrence by a significant 44% compared with AAD. Dr Carlos Morillo Importantly, in the second Radiofrequency Ablation vs Antiarrhythmic Drugs as First-Line Therapy of Atrial Fibrillation (RAAFT 2) trial, which followed all patients with transtelephonic monitoring (TTM), RF ablation's significant advantage over AAD was in reducing bouts of AF that were either symptomatic or asymptomatic. "So to be able to claim victory with ablation, you really need to monitor these patients very judiciously," said RAAFT 2 co-principal investigator Dr Carlos Morillo (Hamilton Health Sciences-McMaster University, ON) when presenting the study here at the Heart Rhythm Society 2012 Scientific Sessions. Ablation also significantly cut the frequency of solely symptomatic AF, he said. "These findings support the indication of radiofrequency pulmonary vein isolation as first-line therapy in patients with paroxysmal atrial fibrillation," he said, pointing out that the catheter therapy is currently relegated to second-tier status for paroxysmal AF not responsive to AAD in the most recent Canadian Cardiovascular Society guidelines. US guidelines are even more restrictive. On the other hand, heartwire reported in 2010 that a European Society of Cardiology guidance supports catheter ablation for paroxysmal AF without an AAD attempt. RAAFT 2 shows that catheter ablation as performed in the trial is a good therapy for paroxysmal AF, Morillo told heartwire, but also "that there's still 50% of patients who, after one single ablation, have a recurrence. Still, that's much better than the 72% at two years with antiarrhythmic drugs. So it's much better but still has limitations." RAAFT 2 randomized 127 patients not previously treated with AAD—87.5% with a history of paroxysmal AF and the rest with persistent AF—either to undergo RF ablation within four to six weeks or to initiate AAD, with 90 days allowed for titrating doses. The patients, most from Canada or Germany but also some from Italy, the Czech Republic, and the US, had normal systolic function, and none had hypertension or heart failure. All were followed with TTM. "These were highly symptomatic patients," Morillo said, noting that patients averaged about 47 AF episodes within the previous six months; yet they were low risk for stroke, with CHADS2 scores averaging 0.5 in the ablation group and 0.7 among those getting AAD. In the ablation group, 15.2% required an additional ablation, including one during the initial treatment period and nine during follow-up. Seven patients (10.6%) went on AAD therapy. In the AAD group, 59% had to discontinue at least one antiarrhythmic drug and 29 patients (47.5%) underwent catheter ablation during the follow-up; AAD consisted usually of either flecainide or propafenone (Rythmol, GlaxoSmithKline). Morillo said patients in the trial were "highly committed," with 19% in both groups having been "fully compliant" with TTM (which meant transmissions biweekly and in the event of symptoms). In the ablation group, 86.4% were compliant at least 75% of the time, as were 78.7% of the AAD group. RAAFT-2 primary outcomes: Recurrence rates at two years for symptomatic or asymptomatic AF, atrial flutter, or atrial tachycardia lasting >30 seconds. End point Ablation, n=66 (%) AAD, n=61 (%) HR (95% CI) p Recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.02 Symptomatic recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.03 Symptomatic AF only ( ) 0.01 Recurrence by clinical criteria only ( ) 0.66 "Of note," Morillo said in his presentation, "when we excluded the transtelephonic monitor, we couldn't show any difference in recurrence of the primary outcome, 31% in the antiarrhythmic drug [group] and 24% in the catheter ablation [group], highlighting the need for very strict monitoring in these patients to be able to define a successful outcome." RF ablation also performed better than AAD for the trial's primary safety outcome, a cluster of adverse events specific to each therapy. In the ablation group, 7.7% of patients had an event in the safety cluster, which included death, tamponade, severe pulmonary vein stenosis, thromboembolism, vascular complications, phrenic nerve injury, or compete AV block within 30 days; tamponade accounted for nearly all of it. Of AAD patients, 19.7% experienced an event in the safety cluster, which contained death, torsades de pointes, bradycardia requiring a pacemaker, syncope, QRS-interval prolongation >50% of baseline, atrial flutter, or any other significant event leading to drug withdrawal—which accounted for most of the events. The literature suggests that most patients with paroxysmal AF require more than one ablation to control symptoms, Morillo said, and based on RAAFT 2, it's far more likely to happen within a year of the first ablation. "Actually, we haven't seen many recurring in the second year."
 wird demnächst wohl mit mehr Nachdruck formuliert werden können. Denn aktuell beim Kongress Heart Rhythm 2012 in Boston vorgestellte neue Studiendaten stärken der Ablationstherapie als First-Line-Option klar den Rücken. In die RAAFT-2 benannte randomisierte Studie, die Dr. Carlos Morillo aus Hamilton/Kanada vorgestellt hat, waren 127 relativ junge Patienten mit symptomatischem paroxysmalem (87,5 Prozent) oder persistierendem Vorhofflimmern aufgenommen worden, davon die meisten an Zentren in Kanada und Deutschland. Die Studienteilnehmer, die so gut wie keine kardiovaskulären Begleiterkrankungen und insofern auch ein sehr niedriges Schlaganfallrisiko hatten, waren zuvor nicht mit Antiarrhythmika behandelt worden. Das Studienprotokoll sah vor, dass die der Radiofrequenz-Ablationstherapie zugeteilten Patienten innerhalb von vier bis sechs Wochen dieser Intervention unterzogen werden. In der Vergleichsgruppe mit medikamentöser Therapie gewährte man 90 Tage für die Einstellung auf die gewählten Antiarrhythmika, am häufigsten Flecainid und Propafenon. In der Nachbeobachtung verließ man sich nicht allein auf die Dokumentation symptomatischer Rezidive. Zur Erfassung auch von asymptomatischen Arrhythmie-Rückfällen wurden alle Patienten ab dem dritten Monat mit einem transtelefonischen Monitor (TTM) ausgestattet. Die Nachbeobachtung betrug bis zu zwei Jahre (im Schnitt 21 Monate). Primärer Endpunkt war die in dieser Zeit akkumulierte Rate der per EKG oder TTM objektivierten symptomatischen und asymptomatischen Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien). Arrhythmie-Rezidive signifikant reduziert. Mit 55 Prozent im Vergleich zu 72 Prozent war diese Rate in der Gruppe mit Ablation signifikant niedriger, so das von Morillo präsentierte Hauptergebnis. Die relative Risikoreduktion durch die Ablation gab er mit 46 Prozent an. Auch die Rate der im EKG bestätigten symptomatischen Arrhythmie-Rezidive (Vorhofflimmern, Vorhofflattern, atrialen Tachykardien) wurde durch die interventionelle Therapie signifikant reduziert (47 versus 59 Prozent). Erneutes Auftreten von symptomatischem Vorhofflimmern wurde bei 41 Prozent (Ablation) und 57 Prozent (Medikation) aller Patienten festgestellt - auch dies ein signifikanter Unterschied zugunsten der Ablation. Auch in puncto Sicherheit schnitt die Ablation gut ab: Die Rate dafür relevanter Ereignisse und Komplikationen betrug 7,7 Prozent, im Vergleich zu 19,5 Prozent in der Gruppe mit Antiarrhythmika. Allerdings sind hier qualitative Unterschiede zu bedenken: Während in der Gruppe mit Ablation Tamponaden das Gros der Komplikationen bildeten, waren es in der Vergleichsgruppe vor allem Therapieabbrüche etwa infolge proarrhythmischer Effekte der Antiarrhythmika. Zu Todesfällen kam es in keiner von beiden Gruppen. Nach Ansicht von Morillo stützen diese Ergebnisse die Strategie, die Radiofrequenz-Ablation mit dem Ziel der Pulmonalvenenisolation künftig als First line therapie. Catheter ablation success rates have improved over time based on a better understanding of atrial fibrillation, new techniques and technology, and greater doctor experience. In early studies, the majority of centers reported single procedure success rates of 60% or more for paroxysmal atrial fibrillation and 30% or less for persistent atrial fibrillation. For multiple procedures, the majority reported success rates of 70% or more for paroxysmal atrial fibrillation and 50% or more for persistent atrial fibrillation.1 Outcomes varied based on differences in technique, experience, skill, and follow-up. In 2005, the first worldwide, multicenter survey on catheter ablation was published using data from 181 centers from 1995–2002. It indicated that 52% of patients having an atrial fibrillation catheter ablation were successful and symptom-free without antiarrhythmic drugs. An additional 23.9% were successful but were on antiarrhythmic drugs. For many, those drugs did not work prior to the ablation. Achieving this success required a second procedure for 24.3%, and a third procedure for 3.1%. Success rates were highest in high-volume centers.2. The second worldwide multicenter survey, on catheter ablations performed from 2003–2006, has subsequently been published and showed an improvement in treatment success. The success rate was 70% without antiarrhythmic drugs vs. 52% in the first survey. The overall success rate, which included patients who continued to take antiarrhythmic drugs, was 80% in the second survey vs. 75.5% in the first. What that means is that only 10% of patients in the second survey had to remain on antiarrhythmic drugs vs. 23.9% in the first survey. More than one ablation procedure was needed to achieve these success rates, but the second survey did not indicate what percentage of patients had second and third procedures. When broken down by type of afib, the success rate without antiarrhythmic drugs was 75% for paroxysmal afib, 65% for persistent afib, and 63% for longstanding persistent afib.3. The second worldwide survey showed that doctors were starting to treat more patients with persistent and longstanding persistent atrial fibrillation with catheter ablation. In the first survey, only 53% of centers performed catheter ablation on patients with persistent atrial fibrillation whereas in the second, 86% of centers treated persistent afib. Similarly, only 20% of centers in the first survey treated patients with longstanding persistent atrial fibrillation, which increased to 47% of centers in the second worldwide survey. Since the second worldwide survey used data on procedures only up until 2006, safety and efficacy should be expected to be higher today using current procedures and experience rates, particularly in high-volume centers. Some centers today cite success rates of 80%–85% for first ablations and 95% for second ablations, but there are variances in how different centers measure success. Measuring Catheter Ablation Success. The HRS Expert Consensus Statement set guidelines for catheter ablation trials. Immediately after the procedure, there is a three-month blanking period during which time atrial fibrillation episodes can occur as part of the body s healing response to the procedure. Any afib activity during that blanking period is not counted in a study s results. After the blanking period, the HRS Expert Consensus Statement defines success as freedom from afib, atrial flutter or tachycardia and discontinuation of antiarrhythmic medication. Patients participating in clinical studies should be followed at least 12 months and, at minimum, should have a 24-hour Holter monitor at three months, six months, one year, and two years.1. Not all doctors involved in clinical studies follow the HRS Expert Consensus Statement guidelines, so when looking at treatment success rates, it s important to look at these three factors: How treatment success was defined — Some studies have a strict definition of treatment success—freedom from atrial fibrillation and antiarrhythmic drugs after a single procedure—while others may count as successes patients who remain on antiarrhythmic medication or who have had multiple procedures. How success is defined can be meaningful because if a study shows a 90% success rate, but only 10% of patients were able to stop taking antiarrhythmic drugs, then you might question the effectiveness of the treatment. What type of monitoring was used after treatment — Most studies officially start tracking a patient s heart rhythm three months after a procedure as the first three months are considered a blanking period . Monitoring methods include patient questionnaires about symptoms, an electrocardiogram (ECG) performed in the doctor s office, a Holter monitor (24-hour, 48-hour, seven-day, or longer), an event monitor, or an implantable loop recorder. An implantable loop recorder (a small device implanted under the skin in the chest area) is the most rigorous follow-up method, and the patient questionnaire is the least. Most studies use a 24- or 48-hour Holter monitor to determine whether atrial fibrillation episodes occur following treatment. What was the length of follow up — Most studies report on treatment successes and failures at one year following the procedure. Generally, success rates that are based on follow up of less than 12 months should be considered preliminary and subject to change as a sizeable percentage of people have an afib recurrence within the first year. In fact, about 30% of patients undergo a second procedure within the first year to treat atrial fibrillation recurrence. Only you can decide what defines treatment success for you. Success may mean freedom from atrial fibrillation and the ability to stop antiarrhythmic medication after one catheter ablation for some people, but for others, alleviation of symptoms, even though they have to remain on antiarrhythmic drugs, may mean success. If you re considering a procedure, ask about the catheter ablation success rate for the specific electrophysiologist and for the center in which it would be done. Also ask about how they define success, such as with or without antiarrhythmic drugs and the number of procedures, and how success is measured, such as by event monitoring, and at what intervals it is measured. It also wouldn t hurt to ask for their success rates and complication rates for the specific technology and tools to be used on you. If you re considering a catheter ablation, you need to know about Catheter Ablation Risks. Radiofrequency (RF) catheter ablation with pulmonary vein isolation is not only safe as a first-line treatment for paroxysmal or persistent atrial fibrillation (AF), it s more likely to suppress AF recurrences than is standard antiarrhythmic drug (AAD) therapy, suggests a randomized trial with a two-year follow-up—one of the longest for an AF-ablation trial [1]. A single ablation procedure reduced the risk of AF recurrence by a significant 44% compared with AAD. Dr Carlos Morillo. Importantly, in the second Radiofrequency Ablation vs Antiarrhythmic Drugs as First-Line Therapy of Atrial Fibrillation (RAAFT 2) trial, which followed all patients with transtelephonic monitoring (TTM), RF ablation s significant advantage over AAD was in reducing bouts of AF that were either symptomatic or asymptomatic. So to be able to claim victory with ablation, you really need to monitor these patients very judiciously, said RAAFT 2 co-principal investigator Dr Carlos Morillo (Hamilton Health Sciences-McMaster University, ON) when presenting the study here at the Heart Rhythm Society 2012 Scientific Sessions. Ablation also significantly cut the frequency of solely symptomatic AF, he said. These findings support the indication of radiofrequency pulmonary vein isolation as first-line therapy in patients with paroxysmal atrial fibrillation, he said, pointing out that the catheter therapy is currently relegated to second-tier status for paroxysmal AF not responsive to AAD in the most recent Canadian Cardiovascular Society guidelines. US guidelines are even more restrictive. On the other hand, heartwire reported in 2010 that a European Society of Cardiology guidance supports catheter ablation for paroxysmal AF without an AAD attempt. RAAFT 2 shows that catheter ablation as performed in the trial is a good therapy for paroxysmal AF, Morillo told heartwire, but also that there s still 50% of patients who, after one single ablation, have a recurrence. Still, that s much better than the 72% at two years with antiarrhythmic drugs. So it s much better but still has limitations. RAAFT 2 randomized 127 patients not previously treated with AAD—87.5% with a history of paroxysmal AF and the rest with persistent AF—either to undergo RF ablation within four to six weeks or to initiate AAD, with 90 days allowed for titrating doses. The patients, most from Canada or Germany but also some from Italy, the Czech Republic, and the US, had normal systolic function, and none had hypertension or heart failure. All were followed with TTM. These were highly symptomatic patients, Morillo said, noting that patients averaged about 47 AF episodes within the previous six months; yet they were low risk for stroke, with CHADS2 scores averaging 0.5 in the ablation group and 0.7 among those getting AAD. In the ablation group, 15.2% required an additional ablation, including one during the initial treatment period and nine during follow-up. Seven patients (10.6%) went on AAD therapy. In the AAD group, 59% had to discontinue at least one antiarrhythmic drug and 29 patients (47.5%) underwent catheter ablation during the follow-up; AAD consisted usually of either flecainide or propafenone (Rythmol, GlaxoSmithKline). Morillo said patients in the trial were highly committed, with 19% in both groups having been fully compliant with TTM (which meant transmissions biweekly and in the event of symptoms). In the ablation group, 86.4% were compliant at least 75% of the time, as were 78.7% of the AAD group. RAAFT-2 primary outcomes: Recurrence rates at two years for symptomatic or asymptomatic AF, atrial flutter, or atrial tachycardia lasting >30 seconds. End point Ablation, n=66 (%) AAD, n=61 (%) HR (95% CI) p Recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.02 Symptomatic recurrence of AF, atrial flutter, or atrial tachycardia ( ) 0.03 Symptomatic AF only ( ) 0.01 Recurrence by clinical criteria only ( ) 0.66 Of note, Morillo said in his presentation, when we excluded the transtelephonic monitor, we couldn t show any difference in recurrence of the primary outcome, 31% in the antiarrhythmic drug [group] and 24% in the catheter ablation [group], highlighting the need for very strict monitoring in these patients to be able to define a successful outcome. RF ablation also performed better than AAD for the trial s primary safety outcome, a cluster of adverse events specific to each therapy. In the ablation group, 7.7% of patients had an event in the safety cluster, which included death, tamponade, severe pulmonary vein stenosis, thromboembolism, vascular complications, phrenic nerve injury, or compete AV block within 30 days; tamponade accounted for nearly all of it. Of AAD patients, 19.7% experienced an event in the safety cluster, which contained death, torsades de pointes, bradycardia requiring a pacemaker, syncope, QRS-interval prolongation >50% of baseline, atrial flutter, or any other significant event leading to drug withdrawal—which accounted for most of the events. The literature suggests that most patients with paroxysmal AF require more than one ablation to control symptoms, Morillo said, and based on RAAFT 2, it s far more likely to happen within a year of the first ablation. Actually, we haven t seen many recurring in the second year.")
39
Update Worldwide Survey on Catheter Ablation of atrial fibrillation
Update Worldwide Survey on Catheter Ablation of atrial fibrillation. Cappato et al; CircEP 2010

40
EHRA – 2012 Focussed Update of the ESC Guidelines for the Management of atrial fibrillation

41
Update Worldwide Survey on Catheter Ablation of atrial fibrillation
Update Worldwide Survey on Catheter Ablation of atrial fibrillation. Cappato et al; CircEP 2010

42
Design of the CABANA Pilot Study
CABANA Pilot Study; ACC 2010 Inclusion Criteria Atrial fibrillation Warranting Therapy >65 yr of age or <65 yr with 1 CVA risk factor Eligible for ablation and/ or drug therapy Drug Rx and AC Rate control Rhythm Rx 1° ablation & AC PV isolation Adjunctive Follow-up 12 months R 60 patients were enrolled, 65% ablation, 41% AAD, follow up nine month 2 paroxysmal AF episodes (1 hour) over 4 months or >1 persistent AF episode (>1 week) 65 yr of age, or <65 yr with 1 risk factors Hypertension Diabetes Heart failure Prior CVA or TIA LA size >5.0 cm (Vol In 40 cc/m2) EF 35 % Eligible for ablation and 2 rhythm control and/or 3 rate control drugs In addition to the STOP-AF trial, Packer presented the results from the pilot Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) study. In contrast to the first study, CABANA included more difficult-to-treat patients, with roughly two-thirds of patients having persistent or long-standing persistent AF. Individuals enrolled in the trial also had more comorbidities, including coronary artery disease, hypertension, and diabetes mellitus. Although the primary end point of the study was freedom from AF, the study was designed to test the feasibility of a long-awaited clinical trial assessing hard clinical end points, including mortality and stroke, with AF ablation. In the pilot study, 60 patients were enrolled and followed for nine months following a three-month blanking period. At the completion of the trial, 65% of patients treated with catheter ablation were free from symptomatic AF, compared with 41% treated with antiarrhythmic drugs, a significant 58% reduction in relative risk. In terms of the recurrence of any AF, atrial flutter, or atrial tachycardia, 72% treated with drug therapy had a recurring event compared with 66% of those treated with ablation, a nonsignificant difference. During the morning press conference, Packer noted that the late recurrence of AF might reduce the long-term effectiveness of ablation and said there is some concern that the relative effectiveness of the two therapies could be similar over time. The results of CABANA are less impressive than the STOP-AF trial, but the patients differed significantly, he said. "There is another critical point, and I think this is the real message of a trial like CABANA: it's not about the recurrence of atrial fibrillation," he said. "It has to be about mortality. It has to be about other aggravating issues like stroke. It has to be about cost, and it has to be about complications. In a way you could say that the recurrence of atrial fibrillation is a surrogate. If these patients have a very good quality of life at low cost to the healthcare system, then we're talking benefit." The CABANA trial, sponsored by the National Heart, Lung, and Blood Institute, as well as Duke University, St Jude Medical, and Biosense Webster, is now enrolling and will include up to 3000 patients followed for an estimated duration of five years. The primary end point is total mortality, and secondary end points include a host of cardiovascular end points, including hospitalizations, bleeding, and stroke, among others. During the late-breaking clinical-trials session, Dr John Camm (St George's Hospital Medical School, London, UK) questioned whether CABANA is sufficiently powered to address these hard cardiovascular end points and whether or not The CABANA trial that is now underway is designed to enroll a sufficiently large number of patients, and continue for a long enough period of time to determine if there is a mortality benefit to catheter ablation of AF.118 In addition, the CABANA study will investigate other outcomes of AF ablation and drug therapy including cardiovascular death, occurrence of disabling stroke, serious bleeding, and cardiac arrest. Rather than comparing any specific drug therapy against an individual ablative intervention, this trial will examine pharmacologic rate and rhythm control strategies and ablative intervention with the intention of eliminating AF. It is hoped that this study will collect mortality information and will expand our understanding of the role of drug and non-drug therapy in those with advancing age, underlying heart disease, and more established AF, which will be applicable to a broader range of patients commonly seen in real life clinical practice. Finally, this trial will gather information needed for assessing the impact
 over 4 months or >1 persistent AF episode (>1 week) 65 yr of age, or <65 yr with 1 risk factors. Hypertension. Diabetes. Heart failure. Prior CVA or TIA. LA size >5.0 cm (Vol In 40 cc/m2) EF 35 % Eligible for ablation and 2 rhythm control and/or 3 rate control drugs. In addition to the STOP-AF trial, Packer presented the results from the pilot Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) study. In contrast to the first study, CABANA included more difficult-to-treat patients, with roughly two-thirds of patients having persistent or long-standing persistent AF. Individuals enrolled in the trial also had more comorbidities, including coronary artery disease, hypertension, and diabetes mellitus. Although the primary end point of the study was freedom from AF, the study was designed to test the feasibility of a long-awaited clinical trial assessing hard clinical end points, including mortality and stroke, with AF ablation. In the pilot study, 60 patients were enrolled and followed for nine months following a three-month blanking period. At the completion of the trial, 65% of patients treated with catheter ablation were free from symptomatic AF, compared with 41% treated with antiarrhythmic drugs, a significant 58% reduction in relative risk. In terms of the recurrence of any AF, atrial flutter, or atrial tachycardia, 72% treated with drug therapy had a recurring event compared with 66% of those treated with ablation, a nonsignificant difference. During the morning press conference, Packer noted that the late recurrence of AF might reduce the long-term effectiveness of ablation and said there is some concern that the relative effectiveness of the two therapies could be similar over time. The results of CABANA are less impressive than the STOP-AF trial, but the patients differed significantly, he said. There is another critical point, and I think this is the real message of a trial like CABANA: it s not about the recurrence of atrial fibrillation, he said. It has to be about mortality. It has to be about other aggravating issues like stroke. It has to be about cost, and it has to be about complications. In a way you could say that the recurrence of atrial fibrillation is a surrogate. If these patients have a very good quality of life at low cost to the healthcare system, then we re talking benefit. The CABANA trial, sponsored by the National Heart, Lung, and Blood Institute, as well as Duke University, St Jude Medical, and Biosense Webster, is now enrolling and will include up to 3000 patients followed for an estimated duration of five years. The primary end point is total mortality, and secondary end points include a host of cardiovascular end points, including hospitalizations, bleeding, and stroke, among others. During the late-breaking clinical-trials session, Dr John Camm (St George s Hospital Medical School, London, UK) questioned whether CABANA is sufficiently powered to address these hard cardiovascular end points and whether or not. The CABANA trial that is now underway is designed to enroll a sufficiently large number of patients, and continue for a long enough period of time to determine. if there is a mortality benefit to catheter ablation of AF.118 In addition, the CABANA study will investigate other outcomes of AF ablation and drug therapy including cardiovascular death, occurrence of disabling stroke, serious bleeding, and cardiac arrest. Rather than comparing any specific drug therapy against an individual. ablative intervention, this trial will examine pharmacologic rate and rhythm control strategies and ablative intervention with the intention of eliminating AF. It is hoped that this study will collect mortality information and will expand our understanding of the role of drug and non-drug therapy in those with advancing age, underlying heart disease, and more established AF, which will be applicable to a broader range of patients commonly seen in real life clinical practice. Finally, this trial will gather information needed for assessing the impact.")
43
CABANA Pilot Study Treatment
CABANA Pilot Study; ACC 2010 Drug Therapy n=31 Ablation n=29 29 (100) 100 80 60 40 20 100 80 60 40 20 n=25 89% 22 71% n=13 46% % % n=11 38% Neue Daten zur Katheterablation bei Vorhofflimmern In einer kleinen Pilotstudie blieben Patienten tendenziell länger symptomfrei als mit Medikamenten. Für die CABANA-Studie werden weltweit Probanden rekrutiert, die randomisiert eine Ablationsbehandlung oder eine frequenz- oder rhythmuskontrollierende Therapie erhalten. Das Ziel wird sein, die Gesamtmortalität zu untersuchen. Eine Pilotstudie dazu mit 60 Patienten wurde am ACC-Kongress in Atlanta, USA, vorgestellt. Anlass für die Studie war die Tatsache, dass rund die Hälfte der Patienten nicht auf medikamentöse Rhythmuskontrolle anspricht und die Arznei teilweise schwere Nebenwirkungen hervorruft. 60 Patienten mit Vorhofflimmern, von denen zwei Drittel eine persistierende Arrhythmie hatten, wurden untersucht. Geachtet wurde hierbei darauf, mit welcher Therapie sich das Wiederauftreten der Arrhythmie länger aufschieben ließ. Komorbiditäten 80 Prozent dieser Patienten litten unter Bluthochdruck, 18 Prozent hatten Diabetes, 35 Prozent eine koronare Herzkrankheit und 36 Prozent hatten eine milde bis mittlere Herzinsuffizienz. Bei 48 Prozent war bereits eine linksatriale Vergrößerung feststellbar. Fast ein Drittel der Probanden hatten früher bereits Medikamente zur Rhythmuskontrolle erhalten. Die Patienten wurden randomisiert auf eine Medikamentengruppe und eine Katheterablationsgruppe aufgeteilt. 87 Prozent der Medikamentengruppe erhielten Mittel zur Rhythmuskontrolle, während bei den restlichen 13 Prozent die Herzfrequenz medikamentös kontrolliert wurde. Die Katheterablation erwies sich effektiver als die medikamentöse Therapie hinsichtlich der Prävention von wiederkehrendem symptomatischem Vorhofflimmern. Allerdings war der Behandlungserfolg bei diesen Patienten, die teilweise unter persistierendem Vorhofflimmern litten, geringer, als dies in anderen randomisierten klinischen Studien berichtet wurde. n=6 21% 5 16% 4 13% n=1 4% Rate Rhythm Rate & rhythm PV isolation WACA/ antral isolation Linear Abl CFAE GP
 n=25 89% % n=13 46% % % n=11 38% Neue Daten zur Katheterablation bei Vorhofflimmern. In einer kleinen Pilotstudie blieben Patienten tendenziell länger symptomfrei als mit Medikamenten. Für die CABANA-Studie werden weltweit Probanden rekrutiert, die randomisiert eine Ablationsbehandlung oder eine frequenz- oder rhythmuskontrollierende Therapie erhalten. Das Ziel wird sein, die Gesamtmortalität zu untersuchen. Eine Pilotstudie dazu mit 60 Patienten wurde am ACC-Kongress in Atlanta, USA, vorgestellt. Anlass für die Studie war die Tatsache, dass rund die Hälfte der Patienten nicht auf medikamentöse Rhythmuskontrolle anspricht und die Arznei teilweise schwere Nebenwirkungen hervorruft. 60 Patienten mit Vorhofflimmern, von denen zwei Drittel eine persistierende Arrhythmie hatten, wurden untersucht. Geachtet wurde hierbei darauf, mit welcher Therapie sich das Wiederauftreten der Arrhythmie länger aufschieben ließ. Komorbiditäten. 80 Prozent dieser Patienten litten unter Bluthochdruck, 18 Prozent hatten Diabetes, 35 Prozent eine koronare Herzkrankheit und 36 Prozent hatten eine milde bis mittlere Herzinsuffizienz. Bei 48 Prozent war bereits eine linksatriale Vergrößerung feststellbar. Fast ein Drittel der Probanden hatten früher bereits Medikamente zur Rhythmuskontrolle erhalten. Die Patienten wurden randomisiert auf eine Medikamentengruppe und eine Katheterablationsgruppe aufgeteilt. 87 Prozent der Medikamentengruppe erhielten Mittel zur Rhythmuskontrolle, während bei den restlichen 13 Prozent die Herzfrequenz medikamentös kontrolliert wurde. Die Katheterablation erwies sich effektiver als die medikamentöse Therapie hinsichtlich der Prävention von wiederkehrendem symptomatischem Vorhofflimmern. Allerdings war der Behandlungserfolg bei diesen Patienten, die teilweise unter persistierendem Vorhofflimmern litten, geringer, als dies in anderen randomisierten klinischen Studien berichtet wurde. n=6. 21% 5. 16% 4. 13% n=1. 4% Rate. Rhythm. Rate & rhythm. PV isolation. WACA/ antral isolation. Linear Abl. CFAE. GP.")
44
Freedom from Recurrence of Symptomatic
Atrial Fibrillation Post Blanking Period HR 0.42 ( ) P=0.033 Ablation 65% Freedom from AF recurrence Blanking period* 41% Drug Rx 24% Time (months)
 P= Ablation. 65% Freedom from AF recurrence. Blanking period* 41% Drug Rx. 24% Time (months)")
45
Welches Verfahren – The simpler, the better ?

46
Welches Verfahren – The simpler, the better ?

47
Welches Verfahren – The simpler, the better ?

48
Welches Verfahren – The simpler, the better ?

49
Welches Verfahren – The simpler, the better ?

50
Welches Verfahren – The simpler, the better ?

51
Welches Verfahren – The simpler, the better ? Cerebrale Mikroembolien

52
Therapie von Vorhofflimmern: Was ist wichtig ?
Rhythmologische Diagnose Kardiovaskuläre Diagnose Symptome / Lebensqualität Risiken Therapieplanung Behandlung Nachbeobachtung In der Framingham - Studie verdoppelt chronisches Vorhofflimmern im Vergleich zur Kontrollgruppe die Mortalität. Eine 3-fach höhere Mortalität wurde bei Männern mit zusätzlicher koronarer Herzerkrankung beobachtet. Der Nachweis von Vorhofflimmern bei Patienten mit einem akuten Myokardinfarkt oder nach Herzoperationen verschlechtert die Prognose zusätzlich. Die Sterblichkeit bei persistierendem Vorhofflimmern ist höher als bei Paroxysmalem. Hauptgrund für die höhere Mortalität ist vor allem das Auftreten von Thromboembolien und hier im Besonderen das Entstehen von apoplektischen Insulten. Vorhofflimmern erhöht das Risiko eines Schlaganfalls um das 5fache. Das Risiko für einen Schlaganfall wird heute anhand von Risikoscores ermittelt (CHADS2 und CHA2DS2 VASc Score).
.")
53
Therapie von Vorhofflimmern: Nachbeobachtung
Mittel: Regelmäßige klinische Kontrolle in der Rhythmussprechstunde LZ EKG 7 Tage EKG Event Recorder (externer oder auch implantierbarer) Telemedizin Entscheidung über Dauer der oralen Antikoagulation: CHA2DS2 VAsC Score HASBLED Score
 Telemedizin. Entscheidung über Dauer der oralen Antikoagulation: CHA2DS2 VAsC Score. HASBLED Score.")
54
Zusammenfassung I Anamnese, Symptome und Behandlungsziele
Entscheidend für die individuell optimale AF-Therapie sind Anamnese, Symptome und Behandlungsziele Die Zielstellung „AF“ und Minderung AF bezogener Risiken ist für viele asymptomatische / mild symptomatische Patienten eine gute Strategie Für die Zielstellung SR kommen Antiarrhythmika und kurative Therapien/ Katheterablation in Betracht Die Zukunft der Therapie von AF liegt in der Ablation

55
Zusammenfassung II Paroxysmales Vorhofflimmern
Wann Ablation ? Paroxysmales Vorhofflimmern „second line“: bei Versagen der antiarrhythmischen Medikation (Flecainid, Propafenon, Dromedaron, Amiodaron) „first line“: bei ausgewählten Patienten ohne strukturelle Herzerkrankung Persistierendes Vorhofflimmern „second line“: bei medikamentöser Therapierefraktärität Evtl. Hybridtherapie mit Antiarrhthmika Häufig sind zwei Ablationssitzungen notwendig
 „first line : bei ausgewählten Patienten ohne strukturelle Herzerkrankung. Persistierendes Vorhofflimmern. „second line : bei medikamentöser Therapierefraktärität. Evtl. Hybridtherapie mit Antiarrhthmika. Häufig sind zwei Ablationssitzungen notwendig.")
56
Vielen Dank für Ihre Aufmerksamkeit

Ähnliche Präsentationen
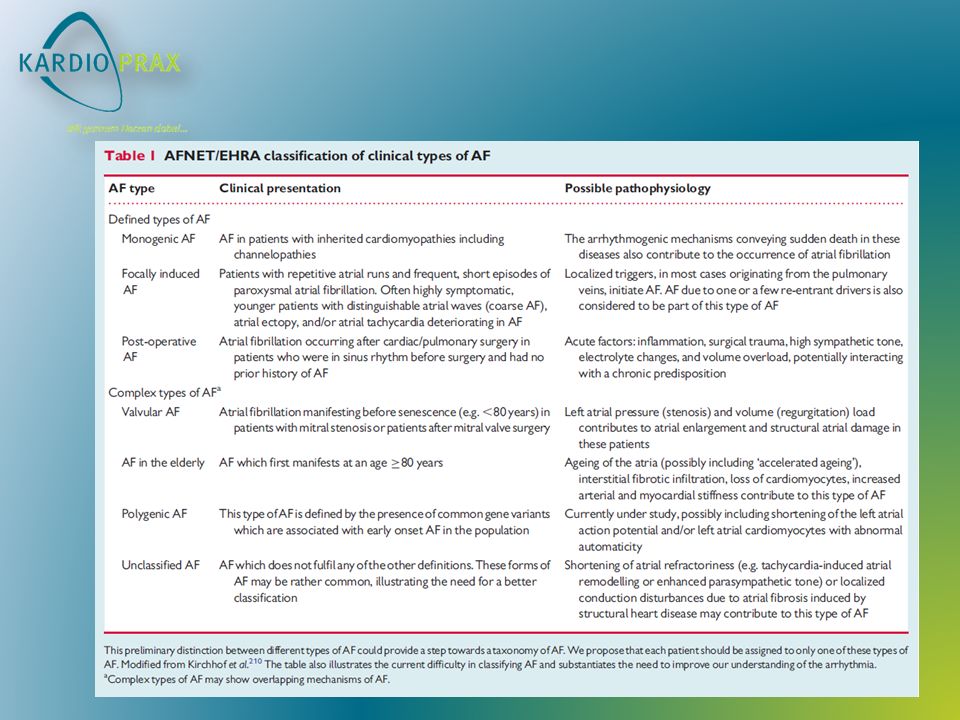
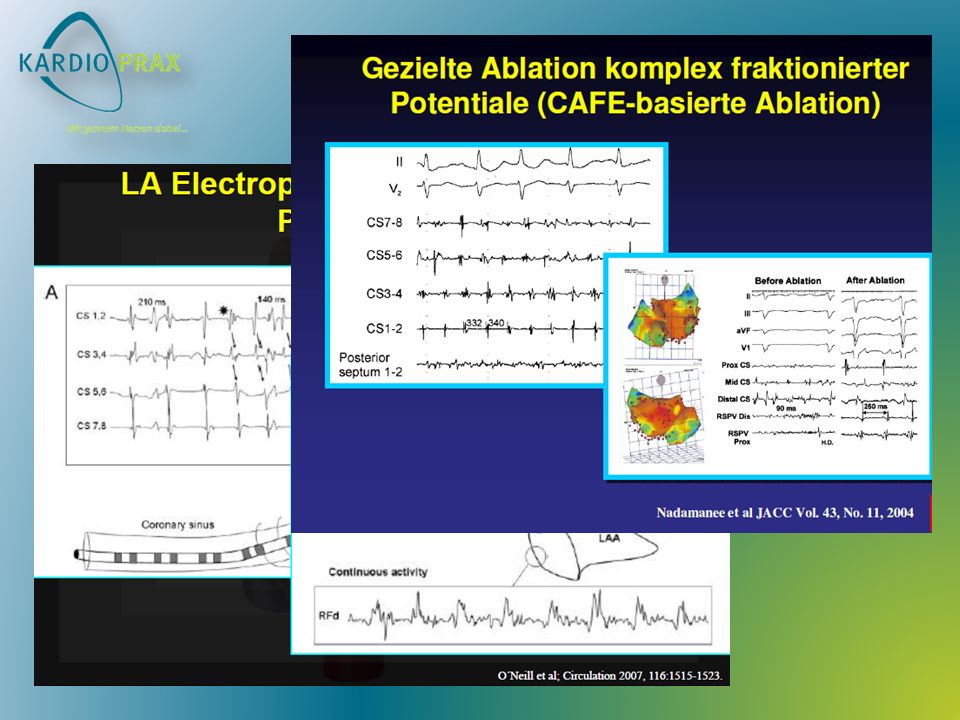









 bei Herzinsuffizienz>")









